Reporte de caso
← vista completaPublicado el 19 de junio de 2024 | http://doi.org/10.5867/medwave.2024.05.2914
Reticulohistiocitosis multicéntrica reveladora de cáncer de mama ductal in situ: reporte de caso con aspectos dermatoscópicos e histopatológicos
Multicentric reticulohistiocytosis revealing a ductal breast cancer in situ: A case report with dermoscopic and histopathological findings
Resumen
La reticulohistiocitosis multicéntrica es una enfermedad inflamatoria, una histiocitosis de células no Langerhans, poco frecuente y de etiología desconocida. Se clasifica como multicéntrica al presentar compromiso multisistémico. La enfermedad afecta predominantemente a la piel y las articulaciones, pero es posible la afectación visceral. Las manifestaciones cutáneas se caracterizan por múltiples nódulos y pápulas de color eritemato-marronáceas, pruriginosas en la cara, manos, cuello y tronco. Se asocia a enfermedades autoinmunes y neoplasias malignas, observándose entre el 20 y el 30% de los pacientes con reticulohistiocitosis multicéntrica. Su diagnóstico se realiza sobre la base de la histopatología de tejidos afectados. Al ser una enfermedad poco reportada, no existe tratamiento estandarizado. Se reporta un caso de reticulohistiocitosis multicéntrica como manifestación paraneoplásica a un cáncer ductal de mama, siendo tratadas con éxito, sin recidivas luego de dos años de seguimiento. Pocos casos se han reportado en la literatura de reticulohistiocitosis multicéntrica asociado a cáncer mamario.
Ideas clave
- La reticulohistiocitosis multicéntrica es una enfermedad inflamatoria, una histiocitosis de células no Langerhans, poco frecuente y de etiología desconocida.
- Sólo se han descrito aproximadamente 300 casos en la literatura.
- Existen muy pocos casos reportados en la literatura de la asociación de reticulohistiocitosis y cáncer mamario.
- Esta asociación es un ejemplo de la importancia de la búsqueda neoplásica en esta enfermedad.
Introducción
La reticulohistiocitosis multicéntrica es una enfermedad inflamatoria, una histiocitosis de células no Langerhans, poco frecuente y de etiología desconocida [1,2,3,4,5,6]. Sólo se han descrito aproximadamente 300 casos en la literatura [4]. La enfermedad afecta predominantemente a la piel y las articulaciones, pero es posible la afectación visceral [3,4,5,6,7]. Compromete mayormente a mujeres en la quinta y sexta década de la vida con una relación mujer-hombre de 3 a 1 [4,5,6].
Las manifestaciones cutáneas se caracterizan por múltiples nódulos y pápulas de color eritemato-marronáceas, pruriginosas en la cara, manos, cuello y tronco [1,8,9]. Las pápulas periungueales en "collar de cuentas de coral", se encuentran presentes en la mitad de los pacientes y representa un signo típico de reticulohistiocitosis multicéntrica [1,10]. En ocasiones el cuadro clínico puede confundirse con una dermatomiositis o artritis reumatoidea [1,4].
Son síntomas frecuentes de reticulohistiocitosis multicéntrica: fiebre, mal estado general, astenia y pérdida de peso [1]. La afectación sistémica incluye derrame pleural, derrame pericárdico, insuficiencia cardiaca congestiva y linfadenopatía mesentérica [4]. Se asocia a hiperlipidemia, prueba de la tuberculina positiva, vasculitis sistémica, enfermedades autoinmunes y neoplasias malignas. Siendo observada la asociación con neoplasias malignas (en general), entre 20 y 30% de pacientes con reticulohistiocitosis multicéntrica [1,2,3,4,5,6,7,8,9,10].
El diagnóstico de reticulohistiocitosis multicéntrica se realiza sobre la base de la histopatología de tejidos afectados [1,4,5,9], observándose un infiltrado típico compuesto por histiocitos y células gigantes multinucleadas con citoplasma eosinófilo y aspecto de vidrio deslustrado [1,2,3,4,5,6,7,8,9,10]. La dermatoscopía puede ser útil para el diagnóstico, con la detección de manchas amarillas/naranjas que es muy indicativa de infiltrado histiocítico en la dermis [8].
Deben realizarse investigaciones radiológicas en todos los pacientes con reticulohistiocitosis multicéntrica para detectar posibles neoplasias acordes al sexo y edad de presentación [6,9]. La tomografía por emisión de positrones/tomografía computarizada con 18F-fluorodesoxiglucosa (FDG-PET/CT) tiene alta sensibilidad y especificidad global para detectar cáncer. Sin embargo, es un examen costoso y de difícil acceso [1,7].
Aunque no existe tratamiento estandarizado para la reticulohistiocitosis multicéntrica, se usan antiinflamatorios no esteroideos, corticosteroides sistémicos, inmunosupresores (como ciclofosfamida, clorambucilo y metotrexato) y biológicos anti-TNF-a, como el etanercept y el infliximab [1]. Los bifosfonatos han demostrado eficacia tanto en la afectación cutánea como en la articular, y pueden usarse como monoterapia o como terapia combinada [1,2]. El reticulohistiocitoma cutáneo se puede extirpar quirúrgicamente, con bajo riesgo de recidiva [2].
El presente manuscrito, expone un reporte de reticulohistiocitosis multicéntrica, poco documentada en la literatura. A partir de este diagnóstico y tamizaje neoplásico, se encontró cáncer mamario asociado.
Caso clínico
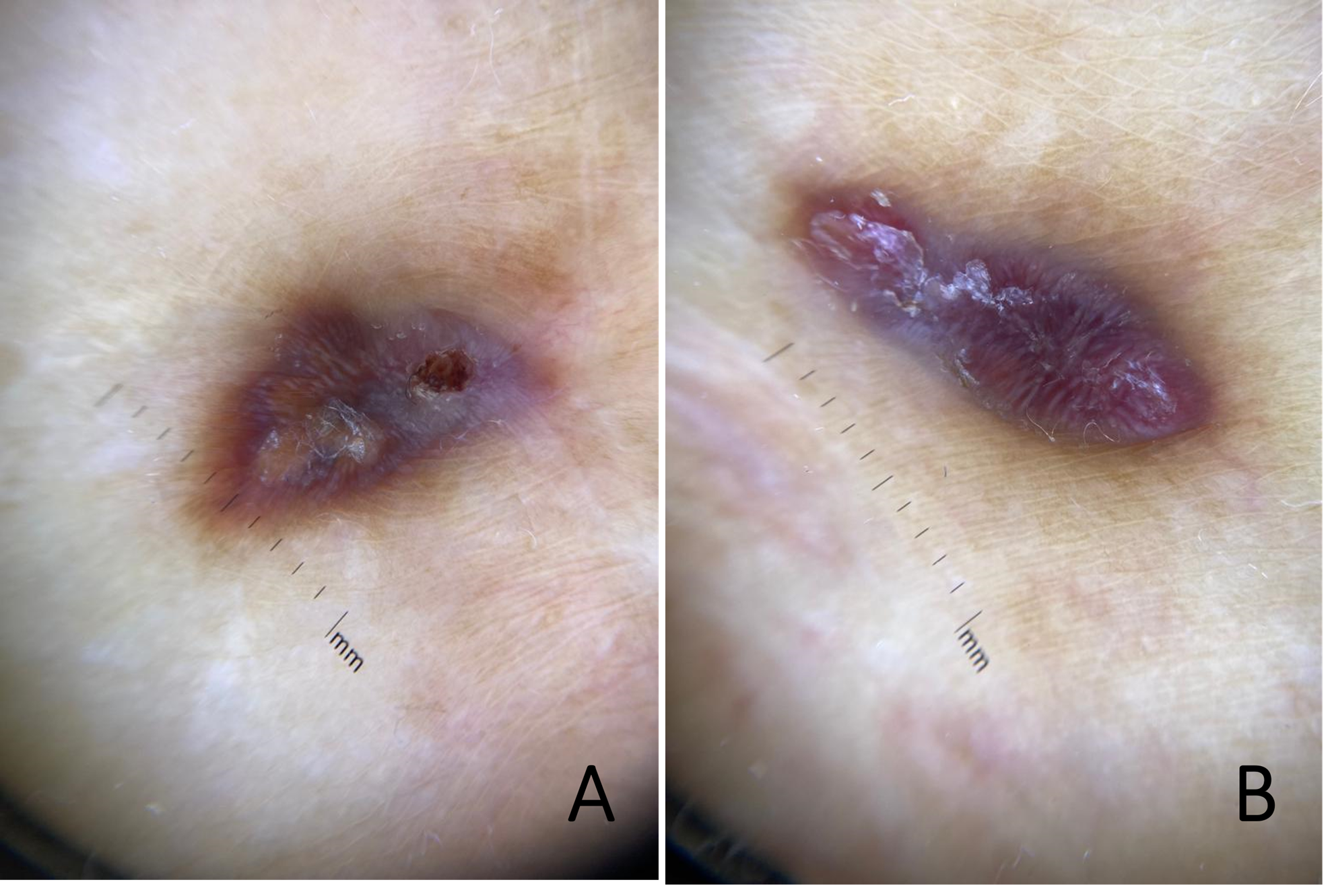
Acudió una paciente de 76 años, con antecedentes de daño hepático crónico no alcohólico, con lesiones en abdomen asintomáticas contiguas a cicatriz de colecistectomía de tres meses de evolución. El examen físico reveló cicatriz sagital abdominal y dos lesiones nodulares eritematosas violáceas bien delimitadas en relación con la cicatriz (Figura 1). No se observaron signos clínicos de compromiso articular. El examen dermatoscópico lesional mostró un fondo eritemato-violáceo, con áreas anaranjadas asociado a un velo blanquecino, estructuras blancas brillantes, descamación, hiperpigmentación difusa periférica (Figura 2A y 2B) y erosión superficial (Figura 2B).
Dos pápulas violáceas en relación con cicatriz abdominal de colecistectomía.

Pápulas, hiperpigmentación difusa periférica y erosión superficial.
Dermatoscopia muestra pápulas con fondo eritemato-violáceo, con áreas anaranjadas. Asociado a un velo blanquecino, se presentan estructuras blanco-brillantes, descamación, hiperpigmentación difusa periférica (Figura 2A y 2B) y erosión superficial (Figura 2B).
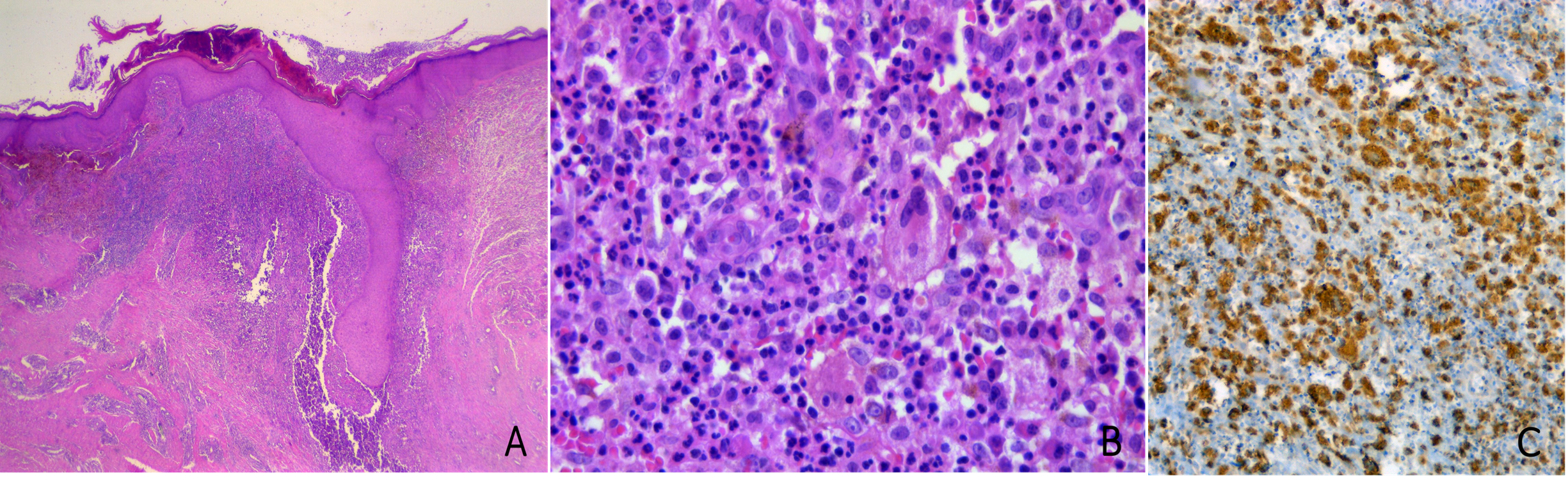
Se realizó biopsia de las dos lesiones abdominales de reticulohistiocitosis multicéntrica encontradas. El examen histopatológico mostró un infiltrado inflamatorio de localización nodular y perifolicular, con histiocitos y algunas células gigantes multinucleadas con citoplasma granular eosinófilo y en “esmerilado”, asociado a linfocitos, neutrófilos y células plasmáticas (Figura 3A y 3B). El estudio inmunohistoquímico mostró que las células histiocíticas son positivas para CD68, mientras que negativas para CD1a, proteína S100 y CD34 (Figura 3C). Los hallazgos morfológicos e inmunohistoquímicos fueron compatibles con reticulohistiocitosis multicéntrica.
Hallazgos histopatológicos.
Figura 3A Imagen a bajo aumento correspondiente al infiltrado nodular superficial y perifolicular (H-E, magnitud original 40x).
Figura 3B Detalle celular del infiltrado, con células histiocíticas y células gigantes multinucleadas, con citoplasma granular y eosinófilo, entremezclado con linfocitos, neutrófilos y células plasmáticas (H-E, magnitud original 400x).
Figura 3C Estudio inmunohistoquímico realizado mostró que las células histiocíticas son positivas para CD68. El resto del estudio inmunohistoquímico fue negativo para CD1a, proteína S100 y CD34.
Dado que la reticulohistiocitosis multicéntrica puede ser un fenómeno paraneoplásico, se realizó una tomografía por emisión de positrones/tomografía computarizada con 18F-fluorodesoxiglucosa para detectar posibles neoplasias malignas ocultas. La imagen resultante mostró una captación anormal de fluorodesoxiglucosa en mama izquierda. También se observó una elevada captación de fluorodesoxiglucosa en los ganglios linfáticos axilares izquierdos, lo que consideramos como un signo de posible malignidad interna. La mamografía mostró microcalcificaciones en mama BI-RADS 4B. Se realizó una biopsia de tejido mamario, que detectó un carcinoma ductal de mama.
Luego de tres meses de la extirpación quirúrgica de las lesiones cutáneas de reticulohistiocitosis multicéntrica, se observó recurrencia de las mismas, de similares características.
La paciente fue sometida a mastectomía parcial izquierda y linfadenectomía axilar, seguidas de radioterapia y terapia con tamoxifeno. A 12 meses de la cirugía, se observó regresión parcial de reticulohistiocitosis multicéntrica, sin recidiva del cáncer mamario. Se cita a control regularmente para seguimiento de las lesiones. Luego de dos años de controles seriados, no ha presentado recidiva de las lesiones.
Discusión
La reticulohistiocitosis multicéntrica es una enfermedad poco frecuente con mayor prevalencia en mujeres que se acompaña de la aparición de lesiones cutáneas y tiene importante asociación con neoplasias malignas [7]. Si bien la fisiopatología es desconocida, se considera que la reticulohistiocitosis multicéntrica tiene una base inmunológica [2,3]. Se ha propuesto la presencia de una proliferación aberrante de histiocitos, produciendo la liberación de citoquinas, interleucina-1, 6, 12 y factor de necrosis tumoral α, generando una respuesta inflamatoria constante en el tiempo [2,3]. El papel de los histiocitos en mecanismos fisiopatológicos como la reparación de tejidos, la respuesta inmunitaria y el desarrollo de neoplasias, apoyaría esta teoría [3].
Presentamos el caso de una paciente con reticulohistiocitosis multicéntrica en que el examen histológico de las lesiones permitió esclarecer el diagnóstico principal y posterior búsqueda de neoplasia oculta, detectando un carcinoma ductal de mama. La reticulohistiocitosis multicéntrica se caracteriza por afectación cutánea que consiste en múltiples pápulas y nódulos cutáneos de color marrón/rojiza, las cuales fueron observadas en la región abdominal de la paciente. La dermatoscopía fue útil en el diagnóstico, observándose manchas amarillas/naranjas las cuales son altamente sugestivas de infiltrado histiocítico en la dermis [1]. Histológicamente, la reticulohistiocitosis multicéntrica consiste en células gigantes multinucleadas y citoplasma eosinifílico [1,2,3,4,5,6,7,8,9,10], estos hallazgos en la biopsia permitieron establecer el diagnóstico. Este caso sugiere la búsqueda activa de neoplasias dirigidas según rango etario y sexo. Se solicitó una tomografía por emisión de positrones/tomografía computarizada con 18F-fluorodesoxiglucosa, ya que entrega información importante acerca de procesos inflamatorios o granulomatosos; además, detecta tumores de forma exitosa [1,7]. Este examen mostró captación anormal en la mama izquierda y la mamografía mostró microcalcificaciones BI-RADS 4B. La biopsia mamaria reveló carcinoma ductal de mama. En esta ocasión, la extirpación quirúrgica de las lesiones cutáneas no fue exitosa. Sin embargo, luego de la mastectomía, radioterapia y tamoxifeno, no se evidenciaron recidivas tanto del cáncer mamario, como de las lesiones de reticulohistiocitosis multicéntrica en un seguimiento de dos años. Un caso similar fue reportado por Dell’Antonia et al [1]. Este caso ilustra la importancia de la detección temprana de lesiones sospechosas de reticulohistiocitosis multicéntrica y tratamiento acorde. Debido a que es una enfermedad con evolución impredecible, se recomienda el seguimiento regular del caso para vigilar el desarrollo o recurrencia de neoplasias.
Conclusiones
La reticulohistiocitosis multicéntrica es una enfermedad inflamatoria, poco frecuente y de etiología desconocida, caracterizada por manifestaciones cutáneas, articulares y viscerales. Por su alta asociación con neoplasias, se sugiere el estudio radiológico de acuerdo a edad y sexo. Debido a que es una enfermedad con evolución impredecible, se recomienda el seguimiento regular para vigilar el desarrollo o recidiva de neoplasia. Aunque no existe tratamiento estandarizado, la detección y tratamiento oportuno es importante para evitar la progresión de la enfermedad.
