Case reports
← vista completaPublished on December 12, 2018 | http://doi.org/10.5867/medwave.2018.08.7379
A case report of intramyocardial bridge on right coronary artery
Reporte de un caso de puente intramiocárdico en arteria coronaria derecha
Abstract
Intramyocardial bridges are a coronary circulation anomaly. They usually occur on the path of the anterior descending artery and are classified as superficial or deep. During a routine autopsy, we found—and report—an intramyocardial bridge in large part of the right coronary artery pathway, including the sinoatrial and posterior descending branch. The patient did not show signs of coronary insufficiency, and died from an acute respiratory failure caused by aspiration pneumonia. Due to the infrequency of cases of intramyocardial bridges of the right coronary artery without concomitant clinical symptoms or signs, we conducted a literature review in this regard.
Introduction
The coronary circulation is responsible for nourishing heart tissue. The main coronary arteries, and their medium-sized branches, are located in the connective tissue of the subepicardial space. However, the penetrating branches are usually intramyocardial. In some people (about 1%) the subepicardial branches describe an intramural course[1]. In these cases, myocardium that covers the artery is defined as a myocardial bridge and the artery is denominated the mural coronary artery or tunneled segment[2].
The cardiac contraction causes an increase of pressure, that can decrease considerably the caliber of the coronary mural arteries. This can produce episodes of ischemia when cardiac activity is increased, as in exercise, stress, fever, etc.[3].
Mural coronary artery is classified as superficial and deep. The hemodynamic impact of them is due to factors such as depth, length, orientation and the presence of connective or adipose tissue accumulated around the tunneled segment. They are classified according to the degree of clinical affection they generate, and based on these; decisions are made for treatment[4]. Most times the course of this condition is asymptomatic, so its diagnosis is an incidental finding[2],[5]. In other patients, it causes alterations in blood flow, which predisposes to atherosclerosis[6], myocardial infarction and sudden death[7].
A study conducted in 1985 in Germany, with 1056 necropsies, found 26% of intramyocardial bridges of which 88% were located in the anterior descending artery[8]. In a smaller series in 1961 up to 86% of this anomaly was recorded[9]. Data from Poland, in 2001, found 41% of intramyocardial bridges in necropsies[10].
Although variants of intramyocardial bridges affecting branches responsible for irrigation of the sinus and atrioventricular nodes have been reported, they are rare[11],[12]. In this report we describe the case of a 42 yeard old man who died of aspiration pneumonia, who during the dissection protocol found an intramyocardial bridge in the right coronary artery whose clinical relevance can not be established.
Clinical case
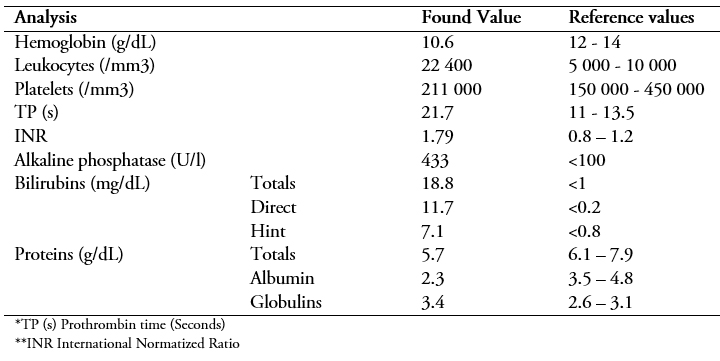
A 42 years-old-man in a situation of social abandonment, with a history of chronic alcohol abuse and malnutrition, arrived at emergency after being found unconscious on public roads. The patient reported that he was drinking alcohol for 3 days in a row. He presented severe dehydration, altered state of consciousness with a tendency to sleep, and was oriented in person but not in space or time. In the regional physical examination, he presented jaundice of skin and mucous membranes and traces of blood in the mouth. Breathing sounds were diminished in both pulmonary fields. The heart sounds were rhythmic and normophonetic. In the abdomen, there was collateral circulation and severe ascites. Due to this clinical picture, he was hospitalized with the diagnosis of alcohol intoxication, hepatic encephalopathy grade I, liver cirrhosis, portal hypertension, and malnutrition. The findings in the laboratory analyzes are presented in Table 1.
 Full size
Full size Later during his hospitalization, he presented a case compatible with pneumonia due to aspiration of gastric content that produced acute respiratory failure. He received antibiotic treatment with Ceftriaxone and Metronidazole without presenting clinical improvement, after which he presented cardiorespiratory arrest without response to cardiopulmonary resuscitation.
The corpse was transferred to the facilities of the regional morgue where the liver disease was confirmed, and the findings compatible with aspiration pneumonia. Later, when not being claimed, and according to legal procedures, the body was donated to the amphitheater of the Faculty of Medicine of Universidad Nacional San Agustín, where it was preserved in formaldehyde and dissected for academic purposes. During the dissection, a liver with a dry weight of 3550 g and adrenal glands with increased size was found.
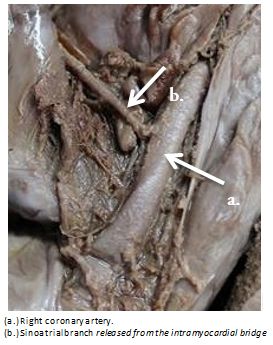
In the thoracic dissection, a heart with measurements of 13 cm (from the origin of the pulmonary trunk to the apex of the heart) and 6 cm (between the most distant ends of both atrial apices) was found. To expose the coronary arteries, the epicardium and adipose tissue adjacent to these were removed using the anatomical reference of the coronary sulci and the appendages of the right and left atria. In this way, the presence of an intramyocardial bridge in the right coronary artery of great extension was exposed; that began approximately 2 cm after its exit from the wall of the ascending aorta artery and included the sinoatrial branch (which irrigates part of the right atrium and the sinus node) (Figure 1) and reached the portion of the posterior surface of the heart, extending to the posterior descending branch. The depth of the intramyocardial bridge was between 2 and 3 mm, although somewhat greater in the distal half of the posterior descending branch, where dissection and isolation were more difficult (Figure 2). Regarding dissection of the left coronary artery, no abnormalities were found, both in the anterior descending branch and in the circumflex branch, in which the obtuse marginal and left marginal branches were dissected, without finding any intramyocardial bridge (Figures 3).
 Full size
Full size 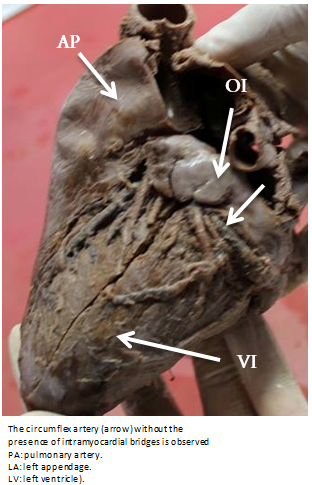 Full size
Full size 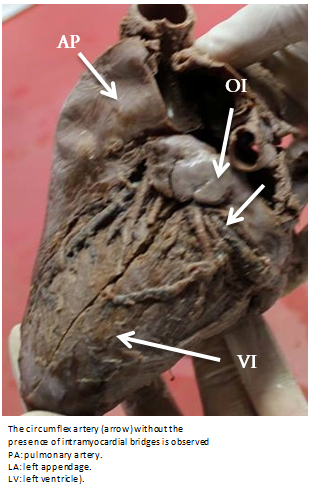 Full size
Full size Discussion
The frequency of intramyocardial bridges found in studies based on necropsies is very different in comparison to the frequency obtained in imaging procedures (coronary angiography, computerized tomography). The finding of intramyocardial bridges in autopsies indicates a variable frequency between 15-85%. In clinical practice, those who are diagnosed through angiography varies between 0.5 to 15%[13],[14],[15].
The relatively high frequency of its finding in several studies, makes the intramyocardial bridges usually are considered by some authors as normal anatomical variants, but there is no consensus on this. The anterior descending artery often has intramyocardial portions in its course, however, it does not usually cause ischemic manifestations[1]. It is very uncommon for intramyocardial bridges to produce clinical manifestations; in many cases, these anomalies are diagnosed as incidental findings in procedures such as coronary angiography or computed tomography, when they are performed in patients with valvular diseases or ischemic heart disease[16],[17]. Its presence occurs especially in cases of secondary ventricular hypertrophy (aortic stenosis, hypertension), primary (hypertrophic cardiomyopathy) and/or associated with adrenal stimulation[1].
For this reason, it can be considered that intramyocardial bridges are a condition that itself, rarely, causes pathologies clinically manifest. Even, some authors point out that these bridges are present in more than 1% of normal human hearts[1].
Although, we have found reports of heart failure, arrhythmia, angina, myocardial infarction and even sudden death (the only symptom, for example, in young athletes)[12],[15],[18],[19],[20]. Angina, in its stable and unstable variants, is the most frequent form of presentation[21]. For example, in a study executed in a population of patients evaluated for chest pain, multidetector computed tomography showed 86 intramyocardial bridges in 82 of the 393 patients (20.9%)[22]. These cases could occur if the segment is particularly long or deep. Some authors support the idea that systolic compression of an intramural anterior descending artery can alter the coronary flow and precipitate myocardial ischemia[13]. The most severe forms of presentation (infarction, arrhythmia, sudden death) are usually related to prolonged ischemia, thrombosis in the intramyocardial bridge or myocardial stunning[21].
The frequency of asymptomatic patients with intramyocardial bridges may seem surprising considering that angiographic data show 50% narrowing of the bridging artery during systole. This frequency could be explained because the largest coronary blood flow occurs during the diastole. However, delayed the diastolic reopening of the compressed artery during systole may explain impaired coronary flow during diastole in symptomatic patients[13].
In our case report, the man of the study seems not to have had clinical manifestations that make us suspect a symptomatic repercussion of the intramyocardial bridge that postmortem was found, because although we do not have all the accessibility that could have revealed other relevant data of the patient's medical history, the reasons for his death were related to chronic alcoholism, malnutrition, and social abandonment.
The anterior descending artery in its proximal and middle thirds is the most common site of muscle bridges[1],[21]. For example, in a study carried out in Warsaw, it was observed a higher prevalence of the intramyocardial bridge in the anterior descending artery (43.2%) than in the right coronary artery (18.4%)[23]. Also in studies performed by computerized tomography, the anterior descending artery was affected more frequently too (87.2%)[22]. The finding of an intramyocardial bridge in the anterior descending artery is so common that even in some studies, such as one based on cinecoronariographies, it was shown that of all the cases described as intramyocardial bridges, 100% corresponded to the anterior descending artery[24]. Similarly, a work performed in a hemodynamic service obtained the same result[25].
However, in this case it was found that the bridge was located entirely in the right coronary artery, including its sinoatrial branch and the posterior descending artery, which is quite unusual since the intramyocardial bridge usually encompasses an artery segment of variable length (between 4 and 25 mm) and not all[26].
Few studies have reported the presence of intramyocardial bridges in the right coronary artery. One of them is a case report in Taiwan, in which it was detected in a 49-year-old man after undergoing angiography[18]; another case was reported in an 81-year-old woman who was being attended in the emergency unit due to a myocardial infarction[12]. In addition, in a study carried out in Brasilia, it was found in the trunk of the right coronary artery of a total of 90 corpses[11]. In an unusual case was also reported the finding of two intramyocardial bridges, which affect the right coronary artery and the anterior descending artery in a 54-year-old man undergoing angiography[19] and finally another case, revealed by angiography the presence of a broad intramyocardial bridge located between the anterior descending artery, the intermediate branch, and the first marginal obtuse branch, which produced chest pain in a 46-year-old man during exercise[20].
Conclusions
The presented case describes an unusual variant of intramyocardial bridge in the path of the right coronary artery, both by the location and by the extension of the bridge, which can be considered as a very rare finding within the totality of cases of myocardial bridges.
The review of the literature forces us to consider intramyocardial bridges as generators, although infrequent, of ischemic pathologies in both elderly and young people, which could potentially trigger sudden death due to arrhythmias or acute myocardial infarction.
Notes
From the editor
The authors originally submitted this article in Spanish and subsequently translated it into English. The Journal has not copyedited this version.
Roles of authorship
KCA, OML, RPO, conceived the report design. KCA, CDT, ZRL, DGS, YNA collected the data and wrote the first version of the manuscript. All authors made critical contributions in the drafting and approval of the final version.
Ethical aspects
This work has been approved by the Ethics Committee of the Honorio Delgado Regional Hospital of Arequipa through Oficio No. -290-2018-GRA/GRS/GR-HRHD/DG-OCDI issued on April 26, 2018.
Note by the authors
The case report was presented at the 2nd International Congress of Clinical Anatomy and the 5th Argentine Congress of Clinical Anatomy, after which the summary was published by the Revista Argentina de Anatomía Clínica (https://revistas.unc.edu.ar/index.php/anatclinar/article/view/19336/19245).
After that, the final version of the article was modified with the recommendations received at the congress. In addition, a clinical orientation was given, adding data corresponding to the patient's clinical history and the development of his disease.
Acknowledgements
To Drs. Herbert Arenas Beltrán, Roxana Paz Aliaga and Magnolia Sierra Delgado, professors of anatomy of the Faculty of Medicine of the National University of San Agustín for facilitating access to the anatomy amphitheatre in order to carry out this work.
Declaration of conflicts of interest
The authors have completed the ICMJE conflict of interest declaration form, and declare that they have not received funding for the completion of the report; have no financial relationships with organizations that might have an interest in the published article in the last three years; and have no other relationships or activities that could influence the published article. Forms can be requested by contacting the responsible author or the editorial board of the Journal.
Statement of funding
The authors state that there were no external sources of funding.
