Research papers
← vista completaPublished on September 25, 2020 | http://doi.org/10.5867/medwave.2020.08.8032
Excess mortality in Metropolitan Lima during the COVID-19 pandemic: A district level comparison
Exceso de mortalidad en Lima Metropolitana durante la pandemia de COVID-19: comparación a nivel distrital
Abstract
Objective To compare excess mortality by district quintiles according to the Human Development Index (HDI) in Metropolitan Lima, the capital of Peru, and analyze the socioeconomic factors associated with excess mortality within the context of COVID-19.
Methods Retrospective cross-sectional analysis of the mortality records from non-violent causes registered in the National Death Information System in the 50 districts of Metropolitan Lima of the first 24 weeks of the years 2019 and 2020. Descriptive analysis was performed using contingency tables and time series graphs by sex, age group, and quintile of the district of residence according to the HDI. Negative binomial regression analysis was performed to identify possible explanatory factors for excess mortality.
Results An excess of 20 093 non-violent deaths and 2,979 confirmed deaths from COVID-19 were registered in Metropolitan Lima during the study period. The increase was observed primarily in men and adults aged 60 and over. Residents in the districts belonging to the fifth quintile, according to HDI, presented, in most cases, the lowest rates. Multivariate analysis revealed that a higher HDI level (p = 0.009) and a higher proportion of inhabitants living in extreme poverty (p = 0.014) decreased the excess mortality.
Conclusion Excess of non-violent deaths in Metropolitan Lima is higher in the quintiles with the lowest HDI, in men, and the age group from 60 to more years of age. The study of social and economic health determinants in Peru is crucial for the design of measures to be taken by the government against the COVID-19 pandemic.
Main messages
- In Metropolitan Lima, there was an excess of 20 093 non-violent deaths during the first 24 weeks of 2020 compared to the previous year.
- Excess of non-violent deaths in Metropolitan Lima is higher in the quintiles with the lowest Human Development Index, in men, and the age group from 60 to more years of age.
- We recommend the replication of this analysis during different stages of the pandemic as a proxy indicator of the impact of the measures implemented by the Peruvian government.
Introduction
The current pandemic caused by the SARS-CoV-2 virus has registered unprecedented morbidity and mortality figures in the 21st century. Up to the end of June 2020, nine and a half million cases had been reported, with almost half a million deaths worldwide seven months after its inception[1]. Peru is one of the most affected Latin American countries with more than 250 000 cases and almost 9000 deaths from this disease[1]. In addition, Peru is among the 15 countries with the highest number of deaths worldwide, with higher figures than countries such as China, a country with a 42-fold greater population density[1]. For this reason, based on the incidence, severity, and deaths from COVID-19, health systems have collapsed, generating a global health crisis.
Recent reports point to excess mortality during the COVID-19 pandemic, mainly in European countries. Spain, the United Kingdom, and Italy have the highest figures for excess mortality per million inhabitants (between 800 and 900 deaths per million inhabitants)[2]. Despite the early prevention measures implemented by the government of Peru, the country ranks sixth with an excess of 400 deaths per million inhabitants. Likewise, regarding registration of the number of fatalities compared to the averages of previous years, Peru ranks first, with an excess of registrations greater than 100% compared to the usual figures[2], possibly due to the lack of care in severe cases, the shortage of hospital beds and intensive care units, and the lack of timely treatment of patients with chronic diseases as a consequence of the pandemic.
Most countries have established mandatory lockdowns as a home-based prevention model due to the lack of an effective treatment or vaccine against SARS-CoV-2. However, this model can present serious limitations for vulnerable families living in socioeconomic conditions that do not favor lockdown compliance[3]. It has been reported that a lower socioeconomic level and the absence of formal education were associated with a higher risk of COVID-19 infection, with a relative risk of 2.19 for the lowest quartile versus the least poor (95% confidence interval: 1.80 to 2.66) and a relative risk of 2.00 for those without certified educational level compared to those with a university degree (95% confidence interval: 1.66 to 2.42)[4]. However, most studies focus on clinical or therapeutic aspects. They do not consider the evaluation of socioeconomic factors, or other potentially important factors such as ethnicity for the identification of the population with increased risk of incidence, transmission, severity, or mortality from COVID-19[5]. In a country with marked inequalities such as Peru, the study of these factors is relevant during this pandemic.
In 2016, Peru implemented the National Death Information System (SINADEF in Spanish), a national system of electronic web registration of deaths, which currently records the majority of fatalities in Metropolitan Lima, the capital of Peru[6]. This information allows the evaluation of mortality figures by economic and sociodemographic characteristics at the district-level in Metropolitan Lima. The purpose of this study was to compare excess mortality by district quintiles according to the Human Development Index (HDI) in Metropolitan Lima and explore the socioeconomic factors associated with excess mortality within the context of COVID-19 in the districts of Metropolitan Lima.
Methods
Study design and data source
We performed a retrospective analysis of the mortality data registered in the districts of the province of Lima (n = 43) and the Constitutional Province of Callao (n = 7), which are a part of Metropolitan Lima with a population of more than 9 million inhabitants in 2017. Districts are the smallest political-administrative units of territorial organization. The records of 49 855 deaths from the 50 districts of Metropolitan Lima due to non-violent causes occurring in the first 24 weeks of 2019 and 2020 were included. A total of 43 753 of the total death records are from the province of Lima and the rest from the Constitutional Province of Callao. For this study, data was collected from various sources of information: deaths were taken from the SINADEF [VCB1] and MINSA through the National Open Data Platform. In turn, the socioeconomic characteristics by district were taken from the National Census 2017 through REDATAM and the National Center for the Strategic Plan (CEPLAN in Spanish). Finally, data related to access to public services and mobility were extracted from the National Census of Supply Markets and the official web pages of Line 1 of the Lima Metro and the Metropolitan Rapid Transit Bus System.
The excess of non-violent deaths in each district was obtained from the difference in total deaths from non-violent causes in the first 24 weeks of the year 2020 and the same period in 2019. The excess of deaths was expressed for every million inhabitants taking into account the population of each district in the 2017 National Census.
The following socioeconomic variables were considered as possible explanatory factors for excess mortality: the HDI, population density, percentage of the population in poverty and extreme poverty, inhabitants over 60 years of age, the self-identified Afro-Peruvian population, the population working in the same district, and houses with access to water from the public network with a computer and internet access. The availability of services was represented by the number of supply markets, health facilities, Metropolitan stations, and the number of metro Line 1 stations in each district. Control variables considered in each district were population size, area (in kilometers squared), and the number of days since the first death from COVID-19 in the district.
Data analysis
A descriptive analysis of excess of mortality was performed using contingency tables and time series graphs to explore the behavior of this variable by sex (male and female), age group (0 to 11, 12 to 17, 18 to 29, 30 to 59, 60 and over), and quintile of the district of residence according to the HDI (Q1 [districts with the lowest HDI], Q2, Q3, Q4 and Q5 [districts with the highest HDI]), as well as their weekly evolution during the study period. In addition, the presence of trends in the time series of excess mortality was evaluated using the Kwiatkowski-Phillips-Schmidt-Shin test (KPSS).
Then, to determine the variables that influence the excess of mortality at the district level, those with collinearity were discarded by evaluating the variance inflation factor. Next, counting data models were run, such as Poisson and negative binomial, in which the population was introduced as an offset, and a logarithmic link function was used. All the predictor variables were quantitative, and none presented records of missing values.
In both models, the independence of errors was evaluated, and the Akaike information criterion and Bayesian information criterion values were reported. Over-dispersion was explored using Pearson's Chi-square residual test, the Bohning test, and the Vuong test to assess the suitability of the Poisson model. In the inferential analysis, a significance level of 0.05 was used, and the results were generated using the R 4.0 and RStudio 1.2 Tools.
Ethics
Since this was an ecological study of aggregated secondary data that is in the public domain and that does not allow identifying individuals who participated in the census or the deceased, the approval of an ethics committee was not requested.
Results
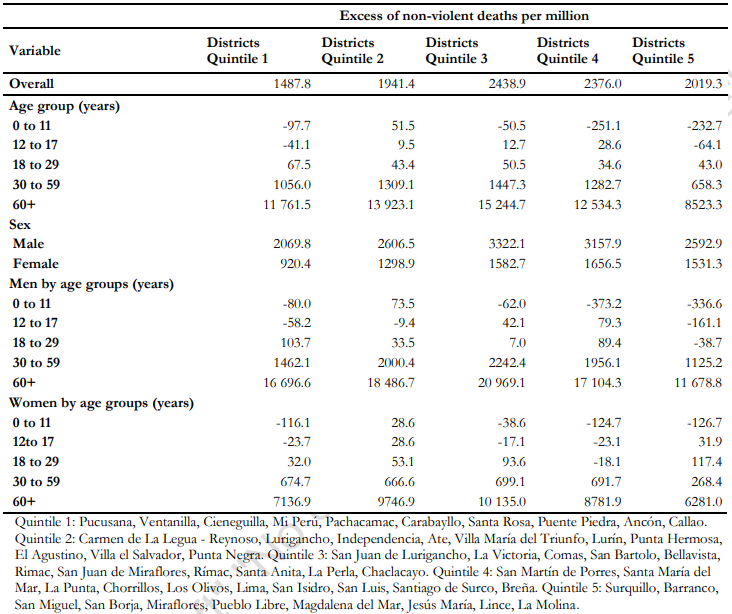
In the first 24 weeks of 2020, an excess of 20 093 non-violent deaths and 2979 confirmed deaths from COVID-19 were registered in Metropolitan Lima when compared to the same period in 2019. Of the non-violent deaths, 34% (6831) were in the two quintiles of districts with the lowest HDI and 65% (13 154) in males. The age group from 0 to 11 years did not present excess of mortality, except in the districts belonging to the second quintile according to the HDI, while age groups from 18 or more years registered excess deaths in all district quintiles according to the HDI. The most affected group was that of men aged 60 and over residing in the districts of the third quintile according to the HDI, with 20 969 excess deaths per million inhabitants. In contrast, males from 0 to 11 years of age residing in the districts of the fourth quintile, according to the HDI, had a deficit of -373.2 deaths per million inhabitants (Table 1).
 Full size
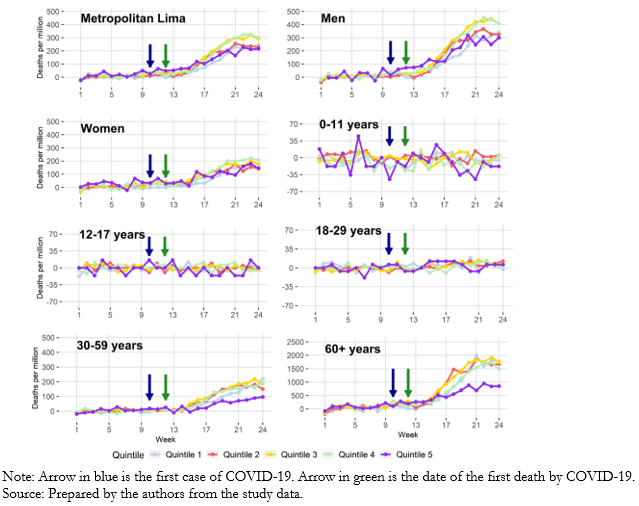
Full size Figure 1 shows the evolution of excess mortality per million inhabitants according to the characteristics of interest. An increase was observed toward the final weeks of the study period for 2020 when compared to that same period in 2019, especially in men and adults aged 60 and over. However, the slope showed a change taking the series to a high, albeit stable, level.
According to the HDI, residents from districts of quintile 5 presented, in most cases, the lowest rates. When applying the KPSS trend test, an increasing trend was detected in the data in all quintiles, and the same occurred when comparing by sex. Nonetheless, differences between age groups were identified. In the 12 to 17 age group, only those residing in districts of the first quintile, according to the HDI, presented an increasing trend of excess mortality (p = 0.028). This was also observed in the residents of the districts of the second (p < 0.01) and third (p < 0.01) quintiles according to the HDI in the age group of 18 to 29 years. An increasing trend in excess deaths was detected in all quintiles for people aged 30 to 59 and 60 and over.
 Full size
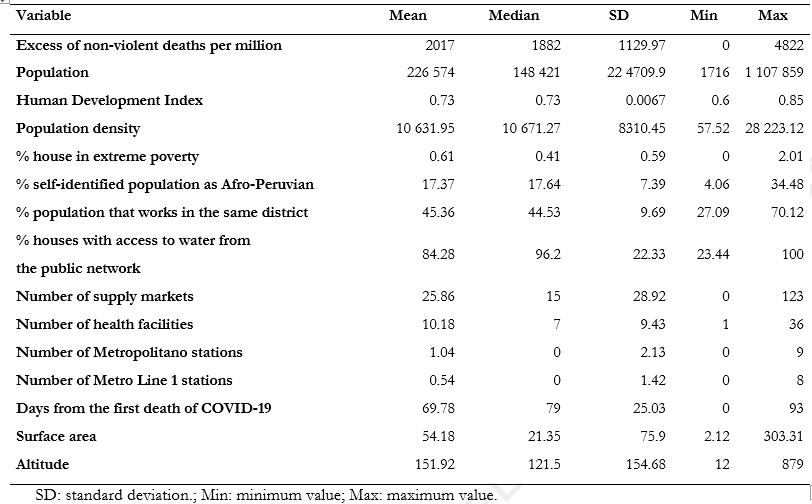
Full size Regarding the socioeconomic characteristics of the districts (see a summary in Table 2), it should be noted that self-identification of the inhabitants as Afro-Peruvian was highest in the districts of East Lima, where 34.48% of the inhabitants of Pachacamac self-identified as Afro-Peruvian, closely followed by 31.26 % of Lurigancho and 30.30% in Cieneguilla and Ate. On the other hand, all districts had at least one health facility. Regarding public transportation services, Line 1 of the Lima Metro supplies nine districts of the city, with the San Juan de Lurigancho district having the most stations, while Metropolitan Rapid Transit Bus System has the highest number of stations in downtown.
 Full size
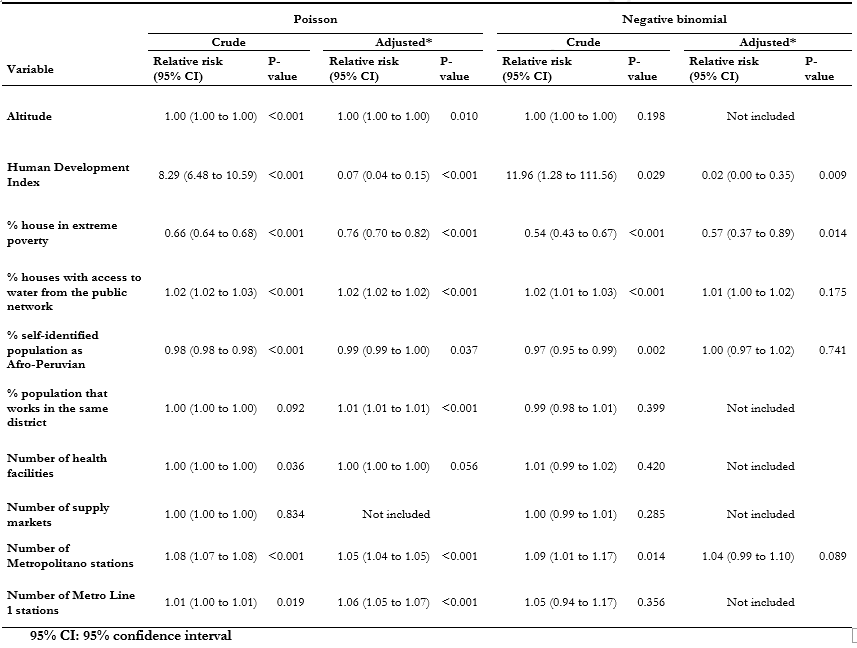
Full size With these variables and the number of excess deaths for each district, bivariate analysis was performed using Poisson regression. However, the results of the Pearson chi-square (p < 0.001) and Bohning tests (p < 0.001) showed over-dispersion in the excess death rate, which is why this model was discarded and the negative binomial model was considered as an alternative. Five explanatory variables with significant individual contribution were selected, of which the multivariate analysis revealed that the HDI (relative risk: 0.02; 95% confidence interval: 0.00 to 0.35; p = 0.009) and the percentage of inhabitants in a situation of extreme poverty (relative risk: 0.57; 95% confidence interval: 0.37 to 0.89; p = 0.014) significantly decreased the rate of excess mortality in Metropolitan Lima (Table 3).
 Full size
Full size Discussion
We report an excess of 20,093 non-violent deaths during the first 24 weeks of 2020 in the districts of Metropolitan Lima when compared to the same period in 2019. Of the total excess deaths, 2979 deaths were attributed to COVID- 19 according to the records of origin (in 87.3% of cases, the cause was unknown). Likewise, the highest proportion of excess deaths (33.5%) was registered in the quintiles of the districts with the lowest HDI. Similarly, the excess deaths per million inhabitants in the districts of all the quintiles, according to the HDI, were greater in males and the age group of 60 years and older. In the general population and populations of men and women, the fifth quintile, according to the HDI, and the age groups of 35 to 59 and from 60 to more years, was the least affected by excess mortality per million inhabitants. Multivariate analysis showed that the HDI and the percentage of inhabitants in a situation of extreme poverty were the influencing variables on the excess death rate in the population of Metropolitan Lima.
Peru is one of the 15 countries in the world with the highest number of deaths from COVID-19, and, like the United States and several European countries, has recorded a high excess of deaths during the pandemic, compared to mortality records from previous years[1],[2]. Our study reported an excess of 20 093 non-violent deaths, of which at least 2979 (14.8%) were attributed to COVID-19. In this regard, some international reports indicated that Peru would have an excess that surpasses 100% of deaths compared to historical data. Likewise, this proportion of excess deaths is greater than that of countries such as the United Kingdom (62%), Spain (61%), Belgium (58%), and the Netherlands (50%)[2]. Similarly, more than 85% of the total excess deaths were not attributed to COVID-19 in the excess mortality records of Metropolitan Lima. However, it is very likely that many of these deaths were due to the disease, and there has been a delay in registering the specific cause of death. In addition, it must be taken into account that a significant proportion of deaths may be due to indirect consequences of the pandemic, such as difficulties in accessing health services (economic incapacity, lack of access to transportation, or collapse of health services ), and a shortage of human and economic resources[7],[8].
Of the total excess deaths, 33.5% were concentrated in the districts of Metropolitan Lima with the lowest HDI (quintiles 1 and 2). It should be considered that the HDI involves the measurement of aspects of health, education, and wealth in the population of a specific geographic area[9]. In this regard, similar to our results, a study carried out in the five municipalities of New York reported that the highest mortality rate from COVID-19 was in the Bronx (224 per 100 000 inhabitants), which has one of the highest proportions of racial and ethnic minorities, as well as the highest proportion of people living in poverty and with low educational levels. In contrast, in the more affluent municipalities, the rates were lower (Manhattan reached a mortality rate of 112 per 100 000 inhabitants)[10]. Similarly, in our study, we found that the age groups most affected by the pandemic in terms of mortality (35 to 59 years and 60 years and older) had a lower excess mortality per million inhabitants in the fifth quintile, according to the HDI. In this regard, it is necessary to take into account that in a context of social inequality, labor informality, and economic precariousness such as that experienced in our country, compliance with effective measures to prevent the spread of the disease, such as mandatory social isolation, is not very manageable for the working class and much worse for those with informal employment. Indeed, before the pandemic, these latter groups represented 70% of the total Peruvian workers[3],[11],[12]. Their condition has worsened because of the inability to work and to changes in consumer preferences and priorities due to lockdown. This is in line with estimates that at least 49 million people worldwide will fall into extreme poverty in 2020 due to the pandemic[13].
Our study recorded higher excess mortality in the male population and people over 60 years of age in all the district quintiles according to the HDI. This pattern has also been reported in Italy by Michelozzi et al., who reported higher excess mortality in men compared to women in northern (+ 87% vs. + 17%) and southern (+ 70% vs. + 9%) Italian cities, respectively[14]. Likewise, this study reported an increase in excess mortality according to age (+ 76% in the group of 65 to 74 years old, + 89% in the group of 75 to 84, and + 102% in those over 85 years of age). Similar patterns in excess mortality have been reported by several studies in different countries[15],[16],[17],[18],[19]. With the current absence of drugs or vaccines with proven efficacy and safety for the disease, knowledge of these patterns would allow anticipating excess deaths in groups of greater vulnerability from potential outbreaks of the disease. This knowledge can also be useful for governments to strengthen prevention in these population groups—all the more so considering that the lifting of lockdown measures has been taking place in many countries around the world.
It should be mentioned that the results of the multivariate model showed the effect of the sociodemographic characteristics of the districts on excess deaths due to COVID-19. In the adjusted model, we found that the excess of deaths per million identified to date can be explained by a lower HDI level (p = 0.009) and a lower excess in districts with a higher percentage of inhabitants in situations of extreme poverty (p = 0.014). This is consistent with the results on the proportion of excess deaths in the districts of Metropolitan Lima, where more than 33% are concentrated in quintiles 4 and 5 according to the HDI.
One of the main limitations of our study was the use of secondary data from the different databases used in the analysis, which may present information bias due to the possible poor quality registration of the data of interest. Likewise, even the causes of death are in the process of quality control and standardization by the Peruvian Ministry of Health, which does not allow the causes of death to be individually identified and compared between the years of study.
Similarly, it should be pointed out that some deaths may be pending notification, mainly in those districts with marginal areas with an inadequate provision of health services. On the other hand, a statistical limitation may be the sample size. Regression models require a minimum of 10 to 20 units of analysis per independent variable; in our study, this rule was valid only for the negative binomial model. Consequently, the Poisson model may suffer from overfitting, meaning its results are valid for the sample but may not be reproducible. For this reason, we preferred to consider the regression through the negative binomial distribution. Bottai also suggested using geometric distribution (a particular case of the negative binomial distribution) for one-time event modeling, such as death[20]. Also, since different measures are being implemented to mitigate the impact of the pandemic, there may be a variation in the mortality outcome over time according to the characteristics evaluated. Despite these limitations, our study only used information on deaths that occurred in Metropolitan Lima, which is the region with the highest percentage of digital death registration nationwide.
In conclusion, in Metropolitan Lima, there was an excess of 20 093 non-violent deaths during the first 24 weeks of 2020 compared to the previous year. This excess was greater in the quintiles of districts with the lowest HDI, in men, and people 60 or older. Excess mortality beyond non-violent deaths caused by COVID-19 can be attributed to the catastrophic indirect impact of the disease on health systems, leading to neglect of other life-threatening diseases or conditions, as well as the large socioeconomic differences of the Peruvian population, even within Metropolitan Lima, which leads to a breach of compulsory isolation. The study of social and economic health determinants in Peru is crucial for the design of measures to be taken by the government against the COVID-19 pandemic. The impact of the pandemic on health and the role of the economy in its outcomes should not be underestimated and should lead the government to take specific measures to reduce gaps in social and economic inequality, as well as to push investments to improve the Peruvian health system.
