Epistemonikos summaries
← vista completaPublished on May 10, 2019 | http://doi.org/10.5867/medwave.2019.04.7623
Weight loss exclusively through diet for knee osteoarthritis
Baja de peso exclusivamente a través de dieta para el tratamiento de la artrosis de rodilla
Abstract
INTRODUCTION Knee osteoarthritis is a highly prevalent chronic disease, associated with various risk factors and with multiple treatment options. Overweight is among the main risk factors and also constitutes an aggravating factor of the symptoms. It has been suggested that weight loss would be able to improve symptoms and to stop the progression. It can be achieved by several methods: exercise, diet, drugs, surgery, or a combination of them. Apparently, diet is a reasonable option given its availability, low technical complexity and greater acceptability, especially in the population susceptible to developing knee osteoarthritis, but it is not clear whether the benefit of diet as the only intervention leads to symptomatic improvement.
METHODS We searched in Epistemonikos, the largest database of systematic reviews in health, which is maintained by screening multiple information sources, including MEDLINE, EMBASE, Cochrane, among others. We extracted data from the systematic reviews, reanalyzed data of primary studies, conducted a meta-analysis and generated a summary of findings table using the GRADE approach.
RESULTS AND CONCLUSIONS We identified seven systematic reviews including six primary studies overall, all corresponding to randomized trials. We concluded diet may improve functionality and quality of life, with probably minimal or no adverse effects. However, we are uncertain whether diet reduces pain as the certainty of the evidence has been assessed as very low.
Problem
Knee osteoarthritis is a highly prevalent condition produced by degeneration of the articular cartilage. It is a chronic and multifactorial disease that leads to pain, substantive functional disability and quality of life deterioration.
Among the modifiable risk factors are overweight and obesity, which, in addition to being associated with greater symptoms, contribute to progression into more severe stages. Because of the role in severity and progression of the symptoms, weight loss is recommended as a fundamental part of the treatment.
The reduction of weight would cause an improvement of the symptoms through the reduction of the mechanical stress on the joint. Additionally, it would decrease the intra-articular and serum levels of mediators such as interleukin-6 and leptin, which would be involved in the pathogenesis of the damage present in this condition.
There are different ways to achieve weight loss; currently the most recommended are diet and exercise, over drugs and surgery, mainly for its ease of implementation and lower rate of adverse effects. Exercise would also have a beneficial effect on functionality of the osteoarthritic knee, independently of the weight loss, but it presents difficulties when implemented in older patients or with clear functional limitation, so weight loss exclusively through diet could be a good alternative. Currently, there is no clarity regarding the benefit of diet as an exclusive measure to achieve symptomatic improvement in knee osteoarthritis.
Methods
We searched in Epistemonikos, the largest database of systematic reviews in health, which is maintained by screening multiple information sources, including MEDLINE, EMBASE, Cochrane, among others, to identify systematic reviews and their included primary studies. We extracted data from the identified reviews and reanalyzed data from primary studies included in those reviews. With this information, we generated a structured summary denominated FRISBEE (Friendly Summary of Body of Evidence using Epistemonikos) using a pre-established format, which includes key messages, a summary of the body of evidence (presented as an evidence matrix in Epistemonikos), meta-analysis of the total of studies when it is possible, a summary of findings table following the GRADE approach and a table of other considerations for decision-making.
|
Key messages
|
About the body of evidence for this question
|
What is the evidence. |
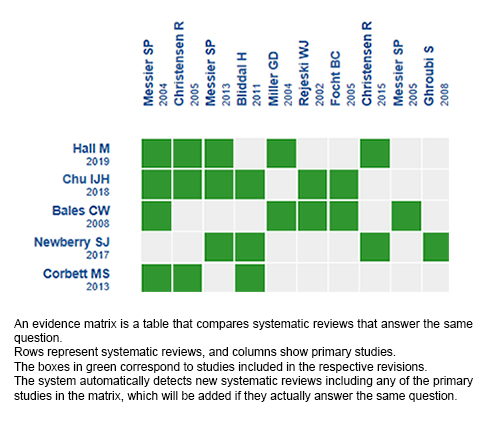
We found seven systematic reviews [1], [2], [3], [4], [5], [6], [7] including six primary studies reported in 14 references [8], [9] , [10], [11], [12], [13], [14], [15], [16], [17], [18], [19], [20], [21], of which all corresponded to randomized trials. |
|
What types of patients were included* |
All trials included adults older than 18 years with a clinical and/or radiological diagnosis of symptomatic unilateral or bilateral knee osteoarthritis, mainly due to pain and functional limitation. All trials included patients who presented some degree of overweight or obesity, with BMI values greater than 28. Two of the trials [10], [21] recruited patients with a BMI greater than 27. Three trials included patients with sedentary lifestyle [8], [9], [10], while the remaining trials did not provide this information [16], [20], [31]. |
|
What types of interventions were included* |
All trials evaluated weight loss exclusively through diet, compared mainly against placebo, exercise, other less intensive diets and healthy lifestyle education sessions. One trial [8] evaluated a diet divided into three phases (intensive phase, transition and maintenance), each with specific goals in addition to educational sessions on healthy lifestyles. One trial [9] evaluated a diet that included the consumption of nutritional powder and weekly dietary educational sessions, compared to another diet with a higher energy content and education on a healthy diet. One trial [20] evaluated a program that consisted of nutritional education and a very low energy diet (485 kcal/ day), compared to a low energy diet (810 kcal/day). In one trial [10], the diet consisted of replacing regular meals of the day with meals adjusted in calories for the weight loss rate, with a goal of 10% reduction in the initial weight, compared against exercise. One trial [16] evaluated a diet based on a reduction of 25% to 30% of the previous caloric level compared against placebo (they received neither diet nor exercise program). In one trial [21] the diet consisted of a nutritional program for weight control, which included weekly diet diaries and information on fat intake and adequate proportions of vegetables, compared with standard care and non-specific health information. |
|
What types of outcomes |
The trials evaluated multiple outcomes, which were grouped by the systematic reviews as follows:
The average follow-up of the trials was 60 weeks with a range between 8 weeks and 18 months. |
* The information was extracted directly from primary studies.
Summary of findings
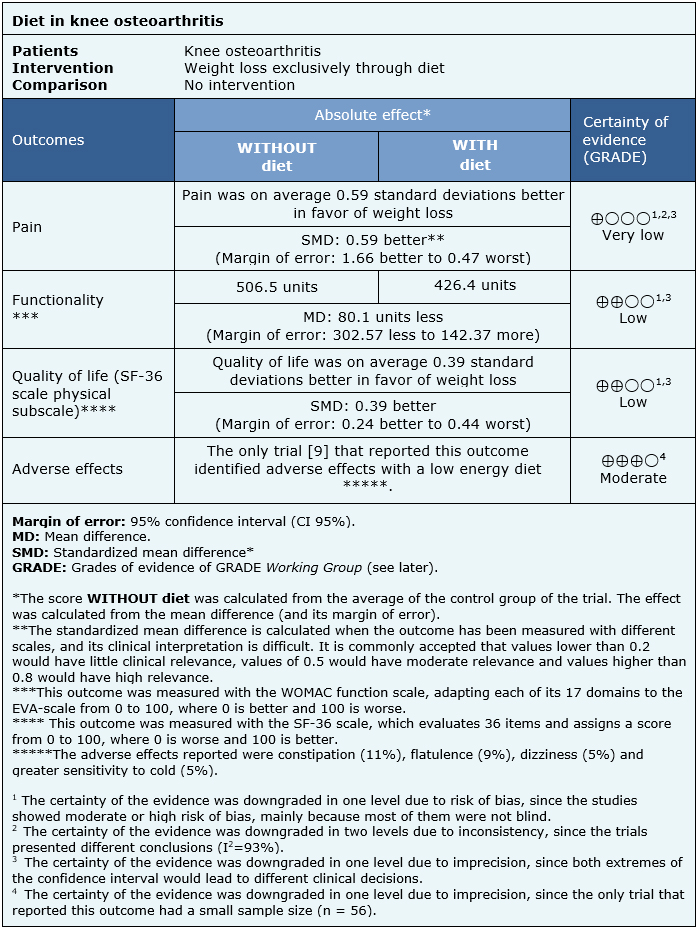
The information on the effects of weight loss exclusively through diet in the treatment of knee osteoarthritis is based on three randomized trials [8], [9], [10] that included 540 patients. The remaining trials did not provide the necessary information to be included in a meta-analysis.
Two trials measured pain (240 patients) [8], [9] using the WOMAC pain scale and Visual Analogue Scale (VAS). One trial measured functionality (80 patients) [9] using the WOMAC function scale. Two trials measured quality of life (693 patients) [8], [10] through the composite SF-36 scale functional subscale. Only one trial [9] reported adverse effects secondary to the intervention (89 patients).
The summary of findings is as follows:
- We are uncertain whether weight loss exclusively through diet reduces pain, as the certainty of the evidence has been assessed as very low.
- Weight loss exclusively through diet may improve functionality (low certainty evidence).
- Weight loss exclusively through diet may improve the quality of life (low certainty evidence).
- Weight loss exclusively through diet probably makes little or no difference to the appearance of adverse effects (moderate certainty evidence).
| Follow the link to access the interactive version of this table (Interactive Summary of Findings – iSoF) |

Other considerations for decision-making
|
To whom this evidence does and does not apply |
|
| About the outcomes included in this summary |
|
| Balance between benefits and risks, and certainty of the evidence |
|
| Resource considerations |
|
| What would patients and their doctors think about this intervention |
|
|
Differences between this summary and other sources |
|
| Could this evidence change in the future? |
|
How we conducted this summary
Using automated and collaborative means, we compiled all the relevant evidence for the question of interest and we present it as a matrix of evidence.
Follow the link to access the interactive version: Weight loss through diet only in knee osteoarthritis treatment.
Notes
The upper portion of the matrix of evidence will display a warning of “new evidence” if new systematic reviews are published after the publication of this summary. Even though the project considers the periodical update of these summaries, users are invited to comment in Medwave or to contact the authors through email if they find new evidence and the summary should be updated earlier.
After creating an account in Epistemonikos, users will be able to save the matrixes and to receive automated notifications any time new evidence potentially relevant for the question appears.
This article is part of the Epistemonikos Evidence Synthesis project. It is elaborated with a pre-established methodology, following rigorous methodological standards and internal peer review process. Each of these articles corresponds to a summary, denominated FRISBEE (Friendly Summary of Body of Evidence using Epistemonikos), whose main objective is to synthesize the body of evidence for a specific question, with a friendly format to clinical professionals. Its main resources are based on the evidence matrix of Epistemonikos and analysis of results using GRADE methodology. Further details of the methods for developing this FRISBEE are described here (http://dx.doi.org/10.5867/medwave.2014.06.5997)
Epistemonikos foundation is a non-for-profit organization aiming to bring information closer to health decision-makers with technology. Its main development is Epistemonikos database (www.epistemonikos.org).
Potential conflicts of interest
The authors do not have relevant interests to declare.
