Epistemonikos summaries
← vista completaPublished on June 26, 2019 | http://doi.org/10.5867/medwave.2019.05.7643
Interventions to reduce the impact of dual practice in the public health sector
Intervenciones para reducir el impacto de la práctica dual en el sector público de salud
Abstract
INTRODUCTION Dual practice (i.e. workers who work in the public and private sector) has an impact on health services in terms of quality and costs. However, the effectiveness of regulatory policies has not been proven.
METHODS We searched in Epistemonikos, the largest database of systematic reviews in health, which is maintained by screening multiple information sources, including MEDLINE, EMBASE, Cochrane, among others. We extracted data from the systematic reviews, reanalyzed data of primary studies, conducted a meta-analysis and generated a summary of findings table using the GRADE approach.
RESULTS AND CONCLUSIONS We identified three systematic reviews that included 23 primary studies overall, of which all correspond to observational studies. We concluded it is not clear whether the interventions to reduce the negative consequences of dual practice in the health system are effective because the certainty of the available evidence is very low.
Problem
Dual practice is a common phenomenon in mixed health systems with the participation of public and private actors. The definition most frequently used is ‘to carry out more than one job’ [1]. In low- and middle-income countries, it has negative effects on the public sector, leading to a deficit of human resources, low salaries and poor working conditions secondary to the growth of the private sector [1].
Although the impact of these practices depends on the context of each country, the negative effects on the public system seem to prevail. This translates, for example, into conflicts of interest where professionals provide suboptimal care, in terms of quality or timeliness, in order to transfer them to the private system [1]. Likewise, dual practice would cause difficulties for the public sector to retain the necessary human resources to satisfy the demand of the population [2]. Despite the observation of the potential negative effects of dual practice on health systems, there is still controversy about the effectiveness of regulatory alternatives to avoid these consequences.
Methods
We searched in Epistemonikos, the largest database of systematic reviews in health, which is maintained by screening multiple information sources, including MEDLINE, EMBASE, Cochrane, among others, to identify systematic reviews and their included primary studies. We extracted data from the identified reviews and reanalyzed data from primary studies included in those reviews. With this information, we generated a structured summary denominated FRISBEE (Friendly Summary of Body of Evidence using Epistemonikos) using a pre-established format, which includes key messages, a summary of the body of evidence (presented as an evidence matrix in Epistemonikos), meta-analysis of the total of studies when it is possible, a summary of findings table following the GRADE approach and a table of other considerations for decision-making.
|
Key messages
|
About the body of evidence for this question
|
What is the evidence. |
We found three systematic reviews [1], [3], [4] that included 23 primary studies [5], [6], [7], [8], [9], [10], [11], [12], [13], [14], [15], [16], [17], [18], [19], [20], [21], [22], [23], [24], [25], [26], [27], [28] of which, all correspond to observational studies. |
|
What kind of countries were included* |
The 23 studies were carried out in countries from different income levels, analyzing physicians or heterogeneous groups that included all types of health professionals. |
|
What types of interventions were included* |
All the studies evaluated the effect on the public sector of regulatory policies at a national level. |
|
What types of outcomes |
The outcomes, as grouped by the systematic reviews, were the following: migration of professionals to the private sector, quality of care and migration of patients to the private sector. |
* The information about primary studies is extracted from the systematic reviews identified, unless otherwise specified.
Summary of findings
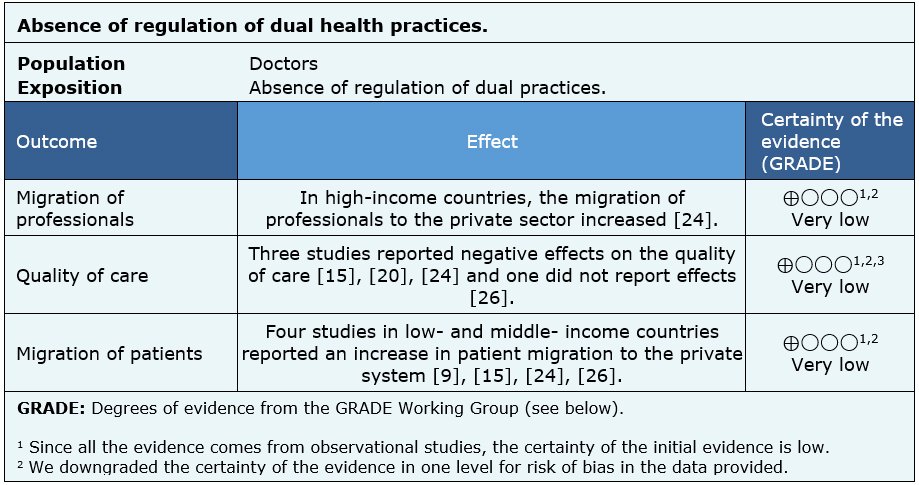
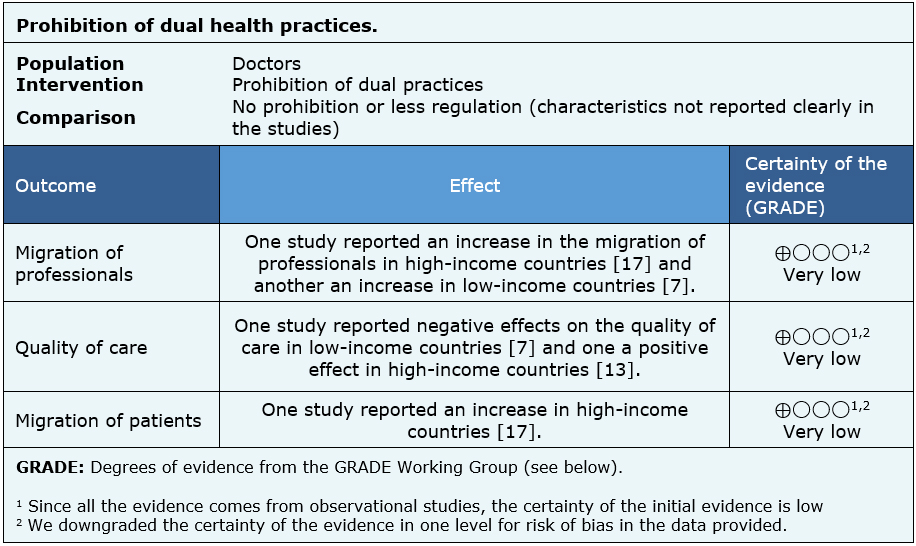
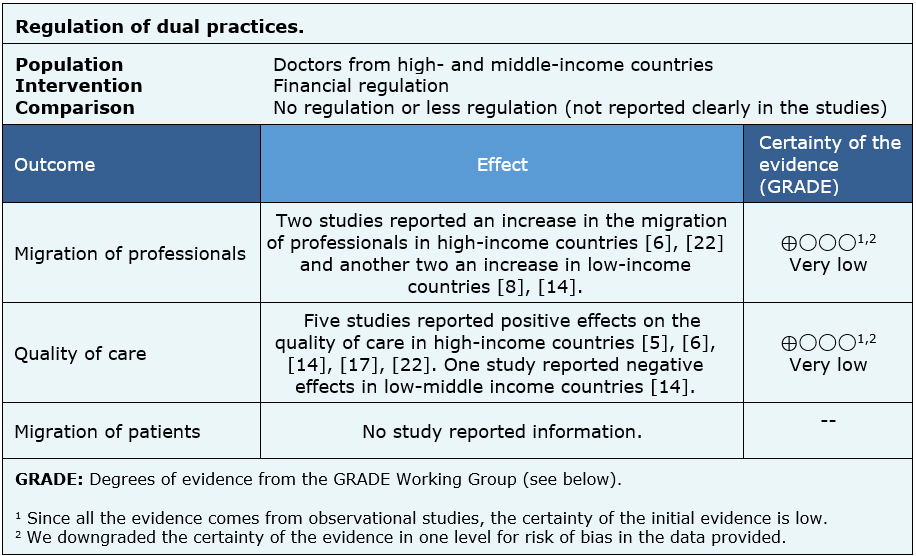
The information on the effects of regulation of dual practices in the public system is based on 21 of the 23 studies identified [5], [6], [7], [8], [9], [10], [11], [12], [13], [14], [15], [17], [18], [20], [21], [22], [23], [24], [25], [26], [27], since two studies did not report any of the outcomes of interest [16], [19]. Twelve studies reported migration of professionals to the private system [6], [7], [8], [9], [10], [11], [12], [13], [22], [24], [17], [14], fourteen reported quality of care [5], [6], [9], [10], [11], [12], [13] [14], [15], [18], [20], [22], [24], [27] and nine migration of patients to the private system [9], [11], [12], [15], [17], [18], [20], [24], [26].
None of the identified reviews managed to extract the data in a way that could be incorporated into a meta-analysis, so the information presented below corresponds to a narrative synthesis of the information obtained from the reviews.
The summary of findings is as follows:
- It is not clear whether interventions to reduce the negative consequences of dual practices in the health system reduces migration of professionals, because the certainty of the available evidence is very low.
- It is not clear whether interventions to reduce the negative consequences of dual practices in the health system improve the quality of care, because the certainty of the available evidence is very low.
- It is not clear whether interventions to reduce the negative consequences of dual practices in the health system reduce patient migration, because the certainty of the available evidence is very low.

Other considerations for decision-making
|
To whom this evidence does and does not apply |
|
| About the outcomes included in this summary |
|
| Balance between benefits and risks, and certainty of the evidence |
|
| Resource considerations |
|
| What would doctors and countries think about this intervention |
|
|
Differences between this summary and other sources |
|
| Could this evidence change in the future? |
|
How we conducted this summary
Using automated and collaborative means, we compiled all the relevant evidence for the question of interest and we present it as a matrix of evidence.
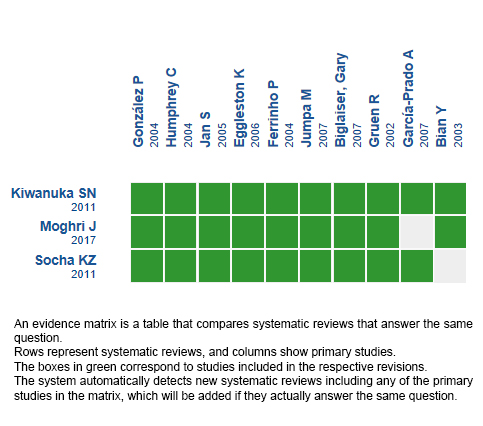
Follow the link to access the interactive version: Regulation of dual practice in the health sector.
Notes
The upper portion of the matrix of evidence will display a warning of “new evidence” if new systematic reviews are published after the publication of this summary. Even though the project considers the periodical update of these summaries, users are invited to comment in Medwave or to contact the authors through email if they find new evidence and the summary should be updated earlier.
After creating an account in Epistemonikos, users will be able to save the matrixes and to receive automated notifications any time new evidence potentially relevant for the question appears.
This article is part of the Epistemonikos Evidence Synthesis project. It is elaborated with a pre-established methodology, following rigorous methodological standards and internal peer review process. Each of these articles corresponds to a summary, denominated FRISBEE (Friendly Summary of Body of Evidence using Epistemonikos), whose main objective is to synthesize the body of evidence for a specific question, with a friendly format to clinical professionals. Its main resources are based on the evidence matrix of Epistemonikos and analysis of results using GRADE methodology. Further details of the methods for developing this FRISBEE are described here (http://dx.doi.org/10.5867/medwave.2014.06.5997)
Epistemonikos foundation is a non-for-profit organization aiming to bring information closer to health decision-makers with technology. Its main development is Epistemonikos database (www.epistemonikos.org).
Potential conflicts of interest
The authors do not have relevant interests to declare.
