Short communications
← vista completaPublished on November 25, 2019 | http://doi.org/10.5867/medwave.2019.10.7734
An assessment of school kiosks in Chimbote (Peru) to curb obesity
Evaluación de kioscos escolares en Chimbote (Perú) en el control de obesidad en la edad escolar
Abstract
School kiosks are spaces where food is provided to preschool and school-age students. Sanitary control of products can help curb and reduce obesity in this study population. We determined compliance and regularity of the evaluation of school kiosks in general and by Regular Elementary Education Institutions in an area of Peru. We performed a secondary cross-sectional analysis of the database of biannual evaluations of school kiosks conducted by the North Pacific Health Network. The main response variables were (a) level of compliance, categorized in Initial (I), In-Process (P), Healthy Kiosk (KS), and Outstanding Healthy Kiosk (KSD). We assigned values from 1 = I to 4 = KSD and assessed the regularity of assessment (schools visited in either semester 1 or 2 or visited in both semesters). The study population consisted of 31 (47.7%) schools out of a total of 65. KS level was reached by 29.1% of the preschool facilities, while 40% of kindergarten/elementary kiosks reached the KS level. Regarding regularity of assessments, 54.8% of kiosks were evaluated in both semesters. All strategic actors of the Ministry of Health and Education must become involved in promoting and facilitating the attainment of the health goals by increasing the number of healthy or featured school kiosks.
|
Key ideas
|
• This is the first study to report an assessment of progress toward achieving the Ministry of Health directive goals by school food kiosks in Peru.
• Schools are effective environments for dietary interventions in children, and the type of food sold by school kiosks can modify eating behavior in students.
• One limitation of this study was the small number of kiosks that were evaluated.
Introduction
Globally, the prevalence of overweight and obesity among children and adolescents 5 to 19 years old increased by 14% between 1975 and 2016[1]. In Peru, the prevalence of obesity increased by 7.5% and 2.6% in children 5 to 9 years old and adolescents, respectively, from 2007 to 2014[2]. Obesity is mainly related to unhealthy eating behaviors, easy access to fast foods, and a sedentary lifestyle. Obesity at an early age represents a risk factor for chronic conditions including high blood pressure, diabetes mellitus, and cardiovascular diseases[3]. Therefore, prevention and awareness activities in school environments are essential.
School kiosks sell food and drinks to students at Regular Basic Education Institutions (Instituciones regulares de educación básica, IEBRs). The food products they sell are heavily processed and include soda and other sugary drinks[4], and the students, who spend nine hours per day at school[5], have no access to healthier options. The increased consumption of processed food and drinks by children and adolescents is strongly associated with the increase in average body weight for this age group[6]. Adequate disease prevention and control, including the promotion of good eating habits, and the implementation of guidelines for the sale of food to children and adolescents recommended by the Ministry of Health (MINSA), can help reduce the risk of overweight and obesity in this population[7].
In 2013, Law No. 30021 on the promotion of good eating habits for children and adolescents was enacted in Peru. This legislation was designed to promote better nutrition in children and adolescents through the sale of healthier food and drinks by IEBR kiosks. In 2015, as part of this campaign, MINSA created a health directive for IEBR food kiosks (Health Directive N° 063-MINSA)[8]. Peruvian health care personnel are responsible for evaluating school kiosks’ progress in achieving the goals set by this directive, which include the sale of healthier foods recommended by MINSA (R.M. No. 908-2012/MINSA)[9], and strategies for promoting healthier eating habits and lifestyles among students. Before this study, the level of achievement of these goals by food kiosks at IEBRs in Chimbote district was unknown. This study was carried out to supply that information by analyzing data from monitoring and evaluation teams at the North Pacific Health Network for 2017 and MINSA goals outlined in annexes 1 and 2 of Health Directive N° 063-MINSA[8]. The study reports Chimbote district school kiosks’ compliance with the health directive by specific evaluation periods, overall, and by type of IEBR (early education, elementary school, high school), categorized as one of four levels of achievement (“Start,” “Process”, “Healthy” and “Outstanding healthy”).
Methods
Study design
This study was a descriptive, cross-sectional, secondary analysis of data from the North Pacific Health Network’s 2017 study of school kiosk compliance with MINSA health directive goals (Monitoring of the Advancement of the Levels of Achievement in School Kiosks of the North Pacific Health Network for 2017). The North Pacific Health Network comprises six micro-networks, including three in the city of Chimbote (El Progreso, Magdalena Nueva, and Miraflores). To meet the requirements of Health Directive N° 063-MINSA, these micro-networks conduct semi-annual evaluations of IEBR food kiosks’ progress in achieving the health directive goals[8].
Population
The study’s target population was food kiosks at the 112 IEBRs in Chimbote city that provide various levels of education (early, elementary, and/or high school). The IEBRs that provide only early education (n = 47) were excluded from the study because they do not have food kiosks.
Variables
The 65 IEBRs included in the study were categorized into five groups by the level(s) of education they provide (“NP”, “NS”, “NIP”, “NPS”, and NIPS”)[5]. There were 16 IEBRs with only elementary school programs (“NP”), 10 with only high school programs (“NS”), 14 with both early education and elementary school programs (“NIP”), 16 with both elementary school and high school programs (“NPS”), and 9 with all three (early education, elementary school, and high school programs) (“NIPS”).
The response variable was the level of achievement of MINSA health directive goals by the school kiosks. Four different levels of achievement were defined (“Start,” “Process,” “Healthy,” and “Outstanding healthy”), based on the following criteria:
- “Start”: kiosk food handlers received training, and kiosk has health checks related to the prevention of foodborne illness.
- “Process”: kiosk meets “Start”-level criteria described above and has health-promoting infrastructure and healthy sanitation practices and/or sells healthy food.
- “Healthy”: kiosk meets “Start”- and “Process”-level criteria described above and conducts the healthy practices for the sale of food recommended by MINSA.
- “Outstanding healthy”: kiosk meets “Start”-, “Process”-, and “Healthy”-level criteria described above and collaborates with IEBR personnel in management and environmental projects for the promotion of healthy eating.
The four levels of achievement were assigned a value of 1 (for “Start”) to 4 (for “Outstanding healthy”).
The evaluations were carried out twice per school year (at the end of the first semester and the end of the third semester). In this study, the frequency of evaluations was categorized as “Semesters 1 or 2” (“S1 or S2”) (January to June or July to December) or “Semesters 1 and 2” (“S1 and S2”) (January to June and July to December).
Analysis
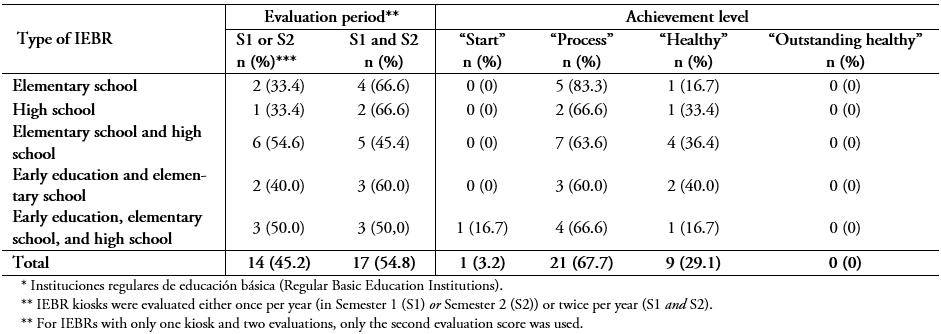
A contingency table was made to show Chimbote district school kiosk progress in meeting the MINSA health directive by type of IEBR and evaluation period (Table 1).
For the IEBRs with only one kiosk that was evaluated in both semesters (S1 and S2), the achievement score for the second evaluation (S2) was used. IEBRs with only one kiosk and evaluated in only one semester (S1 or S2) were rated based on that single score. For IEBRs with more than one kiosk, the average score for all kiosks, from the most recent evaluation, was used. Scores with decimals were rounded up. The analyses were carried out with Microsoft Excel 2016 software.
Results
Of the 65 IEBRs included in the study, kiosks at 47.7% of them were supervised and evaluated by the North Pacific Health Network in 2017, and at almost one-third (29.1%) of them, the kiosks earned a “Healthy” achievement score. No IEBR kiosks included in the study attained an “Outstanding healthy” achievement score. At 54.8% of all IEBRs included in the study, kiosks were supervised and evaluated in both Semesters 1 and 2. At 40% of the IEBRs with both early education and elementary school programs, the kiosks earned a “Healthy” achievement score. No IEBRs with all three programs (early education, elementary school, and high school) had kiosks that attained a “Healthy” achievement level, and only 16% of them had kiosks that attained a “Start” achievement level.
 Full size
Full size Discussion
This study found a low level of compliance with MINSA health directive goals by IEBR school kiosks in Chimbote city, with only one in three establishments attaining a “Healthy” achievement level, based on the scoring criteria. Although no studies methodologically similar to this one was found in the literature, one investigation from Argentina was found that carried out a week-long evaluation of 1) food sold by school kiosks and 2) food wrappers in school garbage cans. That study found high availability and consumption of processed foods in schools[10]. Another study in Guatemala found that students at public schools had no access to drinking water and, in general, school kiosks promoted and sold processed foods[11]. That study concluded that if there is a continuous supply of processed food in school kiosks, students' eating behavior cannot be modified[11]. While schools can be effective environments for implementing diet interventions, this study found that school kiosks in Chimbote city had low compliance with MINSA health directive guidelines[9].
In Peru, supervision and evaluation of school kiosk implementation of MINSA health directive goals are carried out on a semester basis. In this study, more than half of the school kiosks in the sample were supervised and evaluated by the North Pacific Health Network in both Semester 1 and 2. A similar assessment was carried out in Chubut (Argentina) after 2012 when the Ministry of Education required the sale of more nutritious food at school kiosks and provided a list of healthy foods, as well as nutrition advice. Monitoring and evaluation of compliance were carried out by principals and school supervisors[12]. Follow-up monitoring and evaluation by school authorities showed a positive result, including the provision of more nutritious food by school kiosks and, therefore, better eating habits among students[13]. Continuous monitoring of compliance with the health measures to prevent obesity adopted in Peru, including the sale of healthy foods by school kiosks, will help promote the selection and consumption of healthier food by students. The participation of the education and health community is an essential part of this process.
On the other hand, a low level of achievement of the MINSA health directive goals by school kiosks could result in poor nutritional status in students. In this study, just under half of the kiosks at IEBRS with both early education and elementary school programs attained a “Healthy” achievement score. These results are worrisome in terms of public health, given that, according to one study, there are no barriers to students acquiring food from school kiosks[14]. Students attending IEBRs with early education and elementary school programs are between 3 and 11 years old[5]. Exposing students of these ages to kiosks that have not attained a “Healthy” or (best-case scenario) “Outstanding healthy” achievement score for compliance with the MINSA health directive could result in their lifelong consumption of unhealthy food. This could, in turn, result in an unhealthy lifestyle, poor nutritional status, and the development of chronic diseases in adulthood[3]. Therefore, helping school kiosks attain a “Healthy” level of achievement of MINSA health directive goals, with the help of marketing and training strategies, can modify eating behavior in students.
Conclusions and recommendations
In this study, only one-third of the 65 IEBRs in the sample had kiosks that attained a “Healthy” achievement level for compliance with the MINSA health directive to prevent obesity in children and adolescents, and of the IEBRs with the youngest student populations (early education and elementary schools), just under half had kiosks that attained the “Healthy” score. The outcome for the frequency of the compliance evaluation by the North Pacific Health Network was a little better, with kiosks at more than half of the 65 IEBRs supervised and evaluated twice per year (in both Semester 1 and 2).
All participants in the implementation of the MINSA health directive, including MINSA staff and personnel from the Ministry of Education, in collaboration with regional and local governments, must work toward achieving the following objectives:
- Promote effective verification in the performance evaluations carried out by health networks, including micro-networks, to determine the level of achievement of health directive goals by school kiosks.
- Promote awareness of the need for the provision of healthy food and beverages at school kiosks, using IEBR management as strategic allies.
- Publish the results of the evaluations of school kiosk achievements of health directive goals in visible, strategic places, such as the school entrance foyer, classrooms, and the kiosks themselves.
- Train all staff and other representatives of the educational community in health directive goals and promote healthy eating habits in students.
Notes
Roles and authorship contributions
WAI and JBP designed the manuscript and participated in the statistical analysis and the final editing and approval of the study.
Competing interests
The authors declare no competing interests
Funding
This study was funded by Universidad Católica Los Ángeles de Chimbote.
Ethics
This study is a secondary analysis of data from the North Pacific Network of Chimbote; therefore, there was no direct contact between the research team and the study participants. Nonetheless, the study was approved by the Institutional Committee on Research Ethics (CIEI) of the Catholic University Los Angeles of Chimbote (approval #016-2018-CEI-VI-ULADECH-Católica).
From the editor
The original version of this article was submitted in Spanish and was copyedited by the journal.
