Research papers
← vista completaPublished on August 1, 2015 | http://doi.org/10.5867/medwave.2015.06.6194
Anatomic variations of the branches of the aortic arch in a Peruvian population
Variantes anatómicas de las ramas del arco aórtico en una población peruana
Abstract
PURPOSE Previous publications from two countries in South America found one anatomical variation not previously reported in the rest of the world, which in turn give some clues with regard to a racial difference. The objective of the present study is to describe variations in the anatomical distribution of the branches of the aortic arch in a Peruvian population.
OBJECTIVE To describe variations in the anatomical distribution of the branches of the aortic arch in a Peruvian population
METHODS A descriptive study of patients who underwent a tomography angiography of the aorta was performed. We analyzed the reports that showed the description of the variations of the branches of the aortic arch based on the eight types currently described in the literature.
RESULTS From 361 analyzed reports, 282 patients (78.12%) had a normal aortic arch configuration (type I; aortic arch gives rise to the brachiocephalic trunk, left common carotid and left subclavian arteries); followed by type II (left common carotid artery as a branch of the aorta) with 41 patients (11.36%); and type IX (common ostium for the brachiocephalic trunk and the left common carotid artery) with 25 patients (6.93%). The latter and two other types are new variations.
CONCLUSION Aortic Arch Type I, Type II and Type IX were the most frequent variations in this Peruvian study. Additionally, we also found two more new types that have not been previously described in the literature. Further investigation regarding these variations is needed in order to assess a racial factor in South America and possible relationships with clinical or surgical events.
Introduction
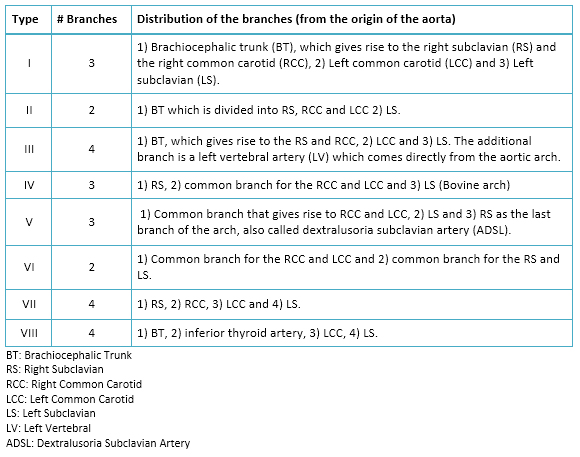
The “normal” configuration of the aortic arch has three branches: A brachiocephalic trunk (BT), which gives rise to the right subclavian (RS) and the right common carotid (RCC), a left common carotid (LCC), and a left subclavian (LS) artery [1]. The variations of the anatomical configuration of the aortic arch are reported from 6 to 49% of the studied population in several countries [1],[2],[3],[4],[5],[6],[7],[8],[9],[10],[11],[12],[13],[14]. However, there is no information regarding the frequency of these variations in Latin American population [1],[2],[3],[4],[5],[6],[7],[8].
Two publications from Colombia and Argentina identified a not previously reported variation, which implies a racial difference in this area of South America when compared to the rest of the published articles regarding this matter [15],[16].
The majority of the aortic arch branches variations are described as asymptomatic, although others have been associated with relevant symptomatology and serious surgical problems, secondary to compression or pressure of the trachea or esophagus [17],[18],[19],[20],[21],[22],[23],[24]. If the physician does not take into consideration the existence of those possibilities, the diagnosis dilates and the costs increase. In our country, unpublished articles related to these variations generate a degree of uncertainty in clinical, radiological and, interventionist practice.
For example, an aberrant vertebral artery as a branch of the aorta is an extremely important variation when cervical vascular surgery is performed, since it will give complications [17],[23]. Apart from that, some authors have suggested that the anomalous origin of the vertebral arteries, coupled with a more extensive vascular path, may cause hemodynamic disturbances that predispose to cerebrovascular diseases [10],[15], whereas others argue that the artery would have a greater flow as it receives the blood directly from the heart; and that the large extension of the artery could affect the hemodynamic resistance of the vessels, thus causing fatigue in the distal portion of the artery [10],[23].
The objective of our study was to describe variations in the anatomical distribution of the branches of the aortic arch in a Peruvian population.
Methods
Study Design, Population and inclusion criteria
This is a descriptive study involving analysis of a series of cases in a Peruvian population. 361 reports of Multislice CT Spiral Angiography (MSCTA), performed by two experienced radiologists of the imaging center “RESOMASA”, during the period 2004-2009, were reviewed. All the MSCTA reports that described the anatomic distribution of the branches of the aortic arch were included in the study, excluding the reports that could have contradictory or incomplete information. Aside from the origin of the population and the sex of the individual, no other sociodemographic variables were included in the study due to the lack of effect of those variables into the embryologic and anatomic configuration of the aortic arch [4].
Procedures for collecting information
The electronic reports were collected in RESOMASA, assigning a code to each one, and then copied to a Compact Disc - Read-Only Memory (CD-ROM) and kept by the researchers for subsequent discharge in the database.
Center and equipment
RESOMASA is a specialized reference center for imaging diagnosis by magnetic resonance and multislice spiral computer tomography SOMATON SENSATION CARDIAC (Siemens Medical Systems, Erlangen, Germany), is located in the department of Lima, the Peruvian capital. RESOMASA is medical team of specialists recognized for their experience and expertise, as well as the accuracy of their images. Since it is a private center, people pay for the imaging tests. The MSCTA report is filled using a format where all the arteries must be specified, thus avoiding an observer omission.
Classification of types of aortic arches
We used the rating by Natsis et al. in his revision article published in 2009 [3]. See table 1.
The other types of aortic arch found continued this classification, being referred to as Type IX, X and XI. See table 2.
 Full size
Full size 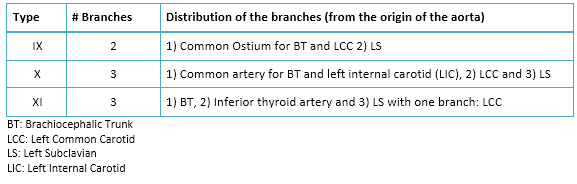 Full size
Full size Statistical analysis
The analysis was performed with STATA statistical software version 10, elaborating frequency tables for the analysis of the qualitative variables.
Ethical issues
The study protocol followed the standards norms of the Helsinki declaration and was approved by the Institutional Ethics Committee of the “Universidad Peruana Cayetano Heredia” and RESOMASA authorities. No names or addresses of the patients were included in the study. The authors signed a letter of commitment to confidentiality of the data.
Results
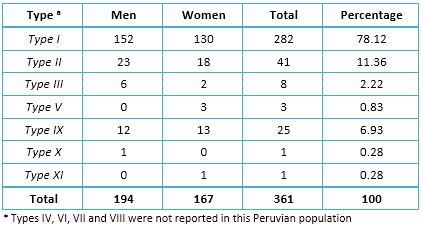
361 reports were included according to our criteria. We found 7 different distributions of the branches of the aortic arch, reporting 3 new types in this population. See table 2. The type I or classic was the most frequent with 275 cases (78.12%), followed by the type II with 41 cases (11.36%), type IX with 25 cases (6.93%), type III with 8 cases (2.22%), type V with 3 cases (0.83%) and type X and XI with 1 case each one. The three new types frequency as well as the frequency of all the other types found are described in table 3. Type IV, VI, VII or VIII variations were not found in our population. The images of the configuration of each aortic arch are shown in Figs. 1 and 2.
 Full size
Full size 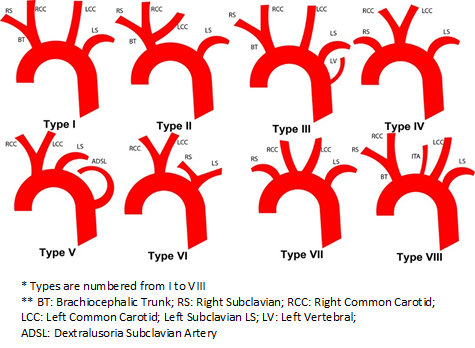 Full size
Full size 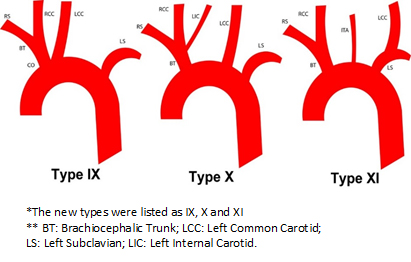 Full size
Full size Discussion
We used the classification of Natsis et al. [3], who made a scientific review of the majority of the published articles on anatomical variations of the aortic arch, categorizing them according to their incidences. In our study, angiography was employed by MSCTA, technique that has shown an excellent correlation with conventional angiography, even in coronary artery atherosclerotic disease [25],[26],[27].
Type I was the most frequent aortic arch configuration reported in our study, which is compatible with other studies worldwide (64.9 - 94.3%) [4],[5],[11]. The second one was type II, whose incidence is also within the range reported in the literature (11-27%) [1],[3],[4]. However, there are two reports with a lover incidence in American-Japanese men (1.03%) [5] and in Polish population (0.9%) [6]. This variation has been rarely associated with clinical symptoms, which were attributed to an expansion of the superior mediastinum [28].
Type III had an incidence of 2.22%. For most authors, this would be the third in terms of incidence (2.5 - 8%) and second to Nelson and Sparks (3.1%) [5]. However, Natsis et al. and Nizankowski et al. reported low frequencies (0.79% and 1.3% respectively) [3],[6]. This variation is very important in neurosurgical and neurovascular interventions because an injury of the vertebral artery is a complication during surgery of the anterior cervical spine, which can cause exsanguination and thus provoke permanent neurological deficits [23]. Furthermore, the vertebral artery can be wrongly considered occluded or diseased when not found by conventional angiography [13]. This variation has only been correlated with clinical symptoms when associated with an intracranial aneurysm [7],[17],[18].
The results of type V are within the described range (0.13% - 25%) with an incidence of 0.83%. Its importance lies in being considered as the cause of "dysphagia lusoria", condition that, despite being asymptomatic in the majority of the cases, could provoke difficult in swallowing and, in some cases, pain due to the pressure exerted by the aberrant artery over the wall of the esophagus, which in turn may need surgical management [29]. It has also been described to cause shortness of breath when the right subclavian meets the trachea. Complications may arise during the tracheostomy if it was found in front of the trachea [30].
We described a variation of the aortic arch that has only been reported in two small series of cases in south-American countries (Colombia and Argentina) [15],[16]. In one article, the authors merely described it as an isolated finding in the part of results [16], whereas the second tried to establish a possible relationship between some variations and the distribution plates of atheroma [15], neither of them highlighting the finding. We called it variation IX, continuing with Natsis classification. Of note, it was the third most common in our series of cases (6.93%) and it is not among the 8 most frequent variations in the literature. Unlike type II, this variation has a common ostium for BT and the LCC. We think that it would be very important to conduct further studies to find out if a relationship with clinical or surgical events exists, as the hemodynamics in a common ostium should be different.
Two more variations of the aortic arch were also found, which have not been reported within the eight most common types described in the literature. Nonetheless, their incidence was less than 1% of the population studied. The main limitations of this study is that it is a series of cases and thus the found frequencies cannot be extrapolated to the rest of the Peruvian population, also, since the MSCTA were performed in a private center, patients pay for their imaging study, which means that most of the patients are middle-class or upper-class Peruvians, so there might be a higher prevalence of some variations in the poorest regions in Peru that are underestimated. However, we believe that an epidemiological study of different populations of our country and from other countries should be performed.
We conclude that in our Peruvian series of cases, the distribution of the branches of the aortic arch of types I, II and IX were the most frequent, the latter being a possible genuine type in south-Americans. In addition, two new not previously described variations were reported. Further investigation regarding this variations is needed in order to assess a racial factor in south-America and possible relationships with clinical or surgical events.
Notes
From the editor
This article was originally submitted in Spanish and was translated into English by the authors. The Journal has not copyedited this version.
Acknowledgments
The authors are grateful to Dr. Pedro Tapia Puente-Arnao and the institution RESOMASA for their selfless support to research, provide all facilities and assistance relating to access its database.
Conflicts of interests
The authors have completed the ICMJE Conflict of Interest form and have no relevant interests to declare.
