Research papers
← vista completaPublished on March 26, 2018 | http://doi.org/10.5867/medwave.2018.02.7184
Frequency and characteristics of gallbladder cancer at a referral hospital in southern Peru, 2009-2014: a descriptive study
Frecuencia y características del cáncer de vesícula biliar en un hospital de referencia al sur del Perú, 2009-2014: estudio descriptivo
Abstract
INTRODUCTION Gallbladder cancer is a rare neoplasm, its frequency is variable in the regions of Peru.
OBJECTIVE To determine the frequency and describe the clinical characteristics of gallbladder cancer in southern Peru.
METHODS The reports of the anatomopathological department of the Honorio Delgado Regional Hospital were selected from all samples of cholecystectomies performed between 2009 and 2014 and those that had some result compatible with gallbladder cancer were looked for. Subsequently, the clinical histories were searched to obtain the characteristics of these patients.
RESULTS Of 2991 cholecystectomies, 75 (2.5%) had gall bladder cancer. The most frequent symptom in both groups was pain (96.7%), followed by nausea (87.5%) and vomiting (65.0%). The majority of patients were women (83.3%) older than 60 years (65.0%). The most frequent histological type was the adenocarcinoma (80.0%).
CONCLUSION The frequency of gallbladder cancer in a reference hospital in southern Peru is 2.51%, higher than that reported in other studies in the central and northern regions of Peru.
Introduction
Gallbladder cancer is the most common malignancy of the biliary tract [1]. Its prevalence is extremely variable according the geographical regions. In some studies, it is the fifth cancer among digestive neoplasms [1]. A 2014 review of the global epidemiology of this disease, reported that indigenous populations, especially the Mapuche, and some Asian populations are often more affected by gallbladder cancer [2]. According to the IX report of cancer incidence worldwide, in America, the highest frequency of gallbladder cancer has been observed in Chile [3]. Other reports also find a high incidence of this disease in Peruvian inhabitants [2],[4].
Due to its clinical presentation, gallbladder cancer is usually confused with benign diseases of the gallbladder [5]; therefore, the identification of its characteristics is fundamental to apply primary care strategies [1].
There are studies at Peru about gallbladder cancer, with variable prevalence between the northern and southern regions [6],[7],[8],[9]. In a city in northern Peru, between 2011 and 2015, 1.0% of vesicle samples sent to the pathology service had gallbladder cancer. In southern Peru, Manrique R et al found a proportion of 0.64% patients with gallbladder cancer among the total number of patients treated in a hospital in the region [7]. Both proportions were calculated differently: in the first study the proportion was based on the samples analyzed by the pathology department; while in the second, it was based on the number of patients seen in the hospital. Therefore, it is not possible to establish a comparison between both frequencies or to know if there is a difference in the prevalence of this disease according to geographical location
The southern region of Peru limits geographically with Chile, a country with a high incidence of gallbladder cancer [3]. Considering this, it could be expected that this region has a higher rate of gallbladder cancer than the rest of the country. It is important to know if this difference in the geographical distribution of the disease exists, in order to be able to plan interventions to improve the early diagnosis and timely treatment of this disease in different regions, as well as to deepen the investigation of the possible causes of this phenomenon.
Therefore, the objective of this study was to determine the hospital prevalence of gallbladder cancer in a referring center in southern Peru between 2009 and 2014. We aimed to estimate the socio-demographic and clinical-pathological characteristics of this disease, in this region of the country.
Methods
A descriptive, observational and retrospective study was carried out in the Honorio Delgado Regional Hospital, a tertiary referral center (level III), and the hospital with the highest level of the health ministry, located in Arequipa, the second most populated city in Peru, as well as the most populated in the southern region of this country.
Population: Patients with gallbladder cancer diagnosed from January 2009 to December 2014, with due histopathological confirmation performed at the hospital. The diagnosis was made based on microscopic analysis of surgical samples of cholecystectomies sent to the service of pathological anatomy. Immunohistochemistry studies were not performed.
Data collection: We recovered data concerning: age, sex, origin, body mass index, and symptoms upon admission, from the medical records of patients with gallbladder cancer.
From the pathological anatomy reports, we obtained the diagnosis, histological type, presence of stones, gallbladder wall thickness, and larger diameter length of the gallbladder. For the staging of the disease, we used the proposal of the American Joint Committee on Cancer (JCC-2017) [10]. An increased vesicle length was considered when it was more than 10 cm [11]. To this end, a pre-designed data collection card was used for this purpose.
Statistical analysis: the analysis was made with the total number of cases in the study period. Qualitative variables were presented as absolute and percentage frequencies. To compare the frequencies reported in other studies with ours, we used the Chi-square test and we calculated the value of the odds ratio (OR) and 95% confidence intervals. We used the statistical package IBM SPSS Statistics, v 22.0 (IBM inc., Chicago, Illinois).
Ethical considerations: Permission was obtained from the competent hospital authorities and the data from the medical records were used confidentially and only for the purposes of this investigation. The Regional Hospital Honorio Delgado does not have an institutional ethics committee, so there is no approval from the ethics committee.
Results
In Figure 1, we observe the selection of the case studies, based on the total number of pieces analyzed in pathological anatomy.
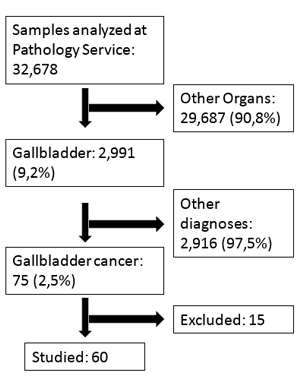 Full size
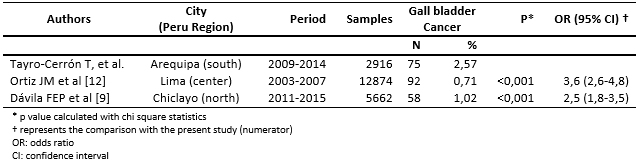
Full size Table 1 shows a comparison made between gallbladder cancer frequencies in three studies conducted in different regions of Peru. The comparisons were made between the studies carried out in the center and the north, with those presented in the southern region (Arequipa).
 Full size
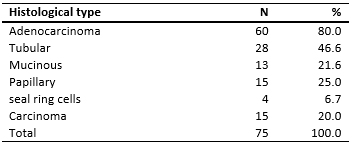
Full size In tables 2 and 3 we analyze the results of pathological anatomy and the progression of the disease respectively.
 Full size
Full size 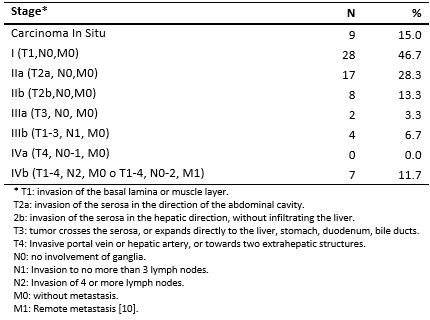 Full size
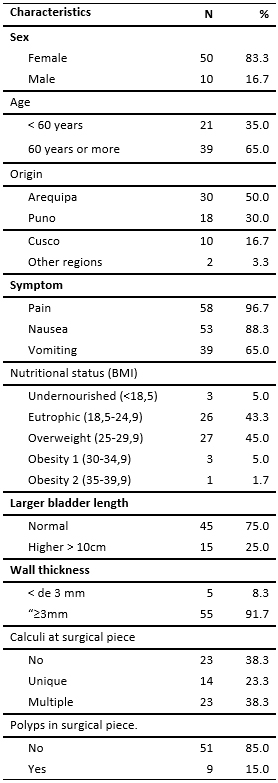
Full size Of the 75 patients with reports of gallbladder cancer in the pathology department, we only retrieved data from 60 medical histories. The characteristics evaluated are presented in Table 4. Table 5 also shows the preoperative diagnoses of the patients.
 Full size
Full size 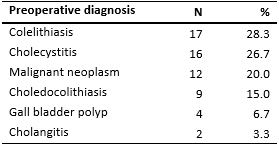 Full size
Full size Discussion
In our study, we found 75 (2.5%) cases of gallbladder cancer. At an international level, a study of a similar design in a Brazilian hospital found a proportion of 1.3% [13], and in Mexico it was reported as 0.26% [5]. Which shows that the values found for our population are high.
The proportion found is higher than that found in other studies conducted in the country (Table 1), despite the fact that the number of cholecystectomies performed was lower compared to the other two studies. This epidemiological situation requires more attention to explain this high frequency in the southern zone of Peru, the associated factors and possible prevention strategies.
It has been proposed that in these regional differences, various factors such as genetic, environmental, and lifestyles such as food and hygiene can influence [14]. A possible explanation related to food, could be related to the fact that in the southern region of Peru, and especially in the city of Arequipa, consumption of the fruit of Capscium pubescens (known as rocoto), is usual and an important part of local gastronomy. This fruit has high levels of aflatoxin and ochratoxin, which have been related to increased risk of gallbladder cancer [15],[16].
Concurrently with most reports, the most common histological type of gallbladder cancer is adenocarcinoma (Table 2) [5],[7],[9]. About the extent of the disease (table 3). It is important to mention that most were in stage T1, followed by T2a, similar to what was previously reported in other national studies. In a previous study conducted at Honorio Delgado Hospital, the most frequent stage of gallbladder cancer was stage II, in which local infiltration causes changes in the vesicle morphology and lymphatic involvement occurs [7]. It is important to point out that the staging carried out in this study was based on the previous recommendations of the Joint Committee on Cancer.
Patients with gallbladder cancer presented as more frequent symptoms: pain, nausea, and vomiting; which are typical symptoms of cholecystopathies [17]. This is consistent with reports indicating that gallbladder cancer is easily confused with benign gall bladder pathology due to nonspecific symptoms [5], and even make gallbladder cancer an anatomopathological finding in operative parts of patients with preoperative diagnosis of cholelithiasis [18],[19],[20].
In Table 4 we find that the majority of patients are women (83.3%) older than 60 years (65%). The relationship between age and gallbladder cancer has been previously described in other studies, finding that usually the benign pathology usually appears around the fourth decade of life, and gallbladder cancer in the sixth [20],[21].
Having identified a high risk in these patients, it is necessary to conduct further studies on the need to establish screening tests for gallbladder cancer in patients with vesicular clinical picture who are older than 60 years; similarly, we recommend that all gallbladder samples of these patients be analyzed in a prioritized manner in anatomopathological laboratories, especially to look for the disease in the early stages [20].
The percentage distribution of patients according to geographical origin was higher in Arequipa 60.0%, then Puno 21.7%, and Cusco with 11.7%; this is due to the fact that the Regional Hospital Honorio Delgado receives a greater proportion of patients from the city of Arequipa, and also receives cases from other cities in the south of the country. The cities of Puno and Cusco are located in the southern highlands of the country and have a greater proportion of indigenous population, so the risk described for these populations could be important in the frequency of this disease [2].
As we observed in the results, the frequency of gallbladder cancer in southern Peru is high; the reason is not yet clear, it may be due to genetic factors, food habits or environmental contaminants [1].
Although the nutritional status is a proven factor for the development of vesicular pathology, being this more common in patients with obesity or overweight, the majority of our patients (48.3%) were eutrophic or malnourished. A meta-analysis conducted in 2015 found that obesity was a mild risk factor for gallbladder cancer (odds ratio= 1.96, 95% CI: 1.38-2.02) [22] and that overweight was not associated with risk of gallbladder cancer.
The size and thickness of the gallbladder were increased in patients. This has also been reported by other authors. Having a limit of more than 3mm for an increased risk of gallbladder cancer [17].
This study has some limitations. It cannot be established that the characteristics presented frequently in patients with gallbladder cancer are associated with or different from those of other types of diseases. In addition, we cannot extrapolate our results to other hospitals in the southern region. In spite of this, the data presented are important and useful for planning and taking decisions in this regard. A recommendation could be not to ignore the anatomopathological analysis of all samples from cholecystectomy in this region, especially in women over 60 years of age. In the same way, it is important to train personnel for the possibility of detecting neoplasia in situ during the surgical act, because these actions have been shown to improve the survival of these patients [23],[24],[25],[26],[27],[28].
Conclusion
In conclusion, the frequency of gallbladder cancer among the samples sent to pathological anatomy is 2.5%. The most frequent characteristics are female sex, age over 60 years and anatomopathological result of tubular adenocarcinoma.
Notes
From the editor
The authors originally submitted this article in Spanish and subsequently translated it into English. The Journal has not copyedited this version.
Editor's note
The principal or responsible author asserts that this manuscript is an honest, accurate and transparent transcription of the study being reported; that no important aspects of the study have been omitted; and that discrepancies between the study results and those anticipated (if relevant) have been recorded and explained.
Declaration of conflicts of interest
The authors have completed the ICMJE conflict of interest declaration form translated into Spanish by Medwave, and declare that they have not received funding for the report; have no financial relationships with organizations that might have an interest in the published article in the last three years; and have no other relationships or activities that could influence the published article. Forms can be requested by contacting the author responsible or the editorial management of the Journal.
Authorship statement
The authors declare that each meets the four criteria of authorship recommended by ICMJE (International Committee of Medical Journal Editors) and recognize the intellectual contributions and responsibilities in the design, writing and review of the contents of this article.
Financing
The authors state that there were no external sources of funding.
