Research papers
← vista completaPublished on July 30, 2019 | http://doi.org/10.5867/medwave.2019.06.7670
Factors associated with the use of nonprescription psychotropic drugs in Chile: A descriptive study using a nationwide drug consumption survey
Factores asociados al consumo de psicofármacos sin receta en Chile: estudio descriptivo basado en la Encuesta Nacional de Consumo de Drogas en Población General
Abstract
Background The consumption of psychotropic drugs without a medical prescription is a growing public health problem worldwide. Misuse or indiscriminate use involves several risks.
Objective To determine sociodemographic factors and behaviors associated with the consumption of psychotropic drugs without prescription in Chile.
Methods This is a descriptive study based on the data of the XI National Study of Drugs in the General Population in Chile, carried out in the population between 12 and 64 years old (n = 19 512) during 2014. Prevalence was estimated, and a multivariate logistic regression model was adjusted. Also, a multiple correspondence analysis was performed.
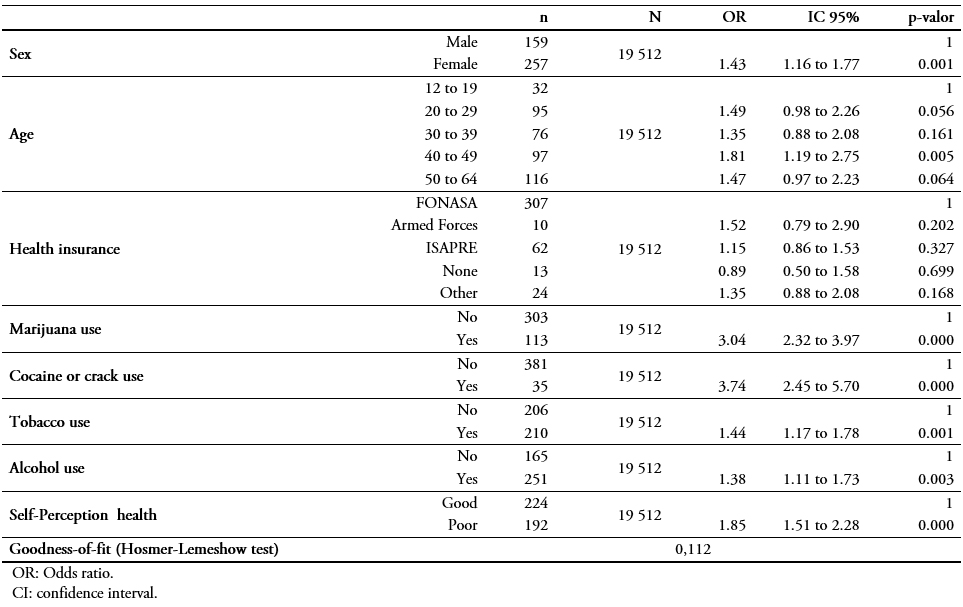
Results The prevalence of psychotropic drug use was 2.3%. In the studied population, associated risk factors are female sex (odds ratio: 1.4; 95% confidence interval: 1.16 to 1.77); ages between 20-29 (odds ratio: 1.4; 95% confidence interval: 0.98 to 2.26) and 40-49 (odds ratio: 1.8; 95% confidence interval: 1.19 to 2.75); consumption of marijuana (odds ratio: 3.0; 95% confidence interval: 3.32 to 3.97), cocaine or crack (odds ratio: 3.7; 95% confidence interval: 2.45 to 5.70); tobacco (odds ratio: 1.4; 95% confidence interval: 1.17 to 1.78); alcohol (odds ratio: 1.3; 95% confidence interval: 1.11 to 1.73); and poor health perception (odds ratio: 1.8; 95% confidence interval: 1.51 to 2.28). Military personnel used more pain and cough medication; young women between 19 to 25 years old used stimulants; the population between 45 to 64 years had a bad perception of health associated with the use of tranquilizers; and men between 12 and 18 years used illicit drugs.
Conclusions The prevalence found in the different groups is consistent with data reported in Latin America, showing the relationship between the use of non-prescription psychotropic drugs with sociodemographic factors, risk behaviors, and the identification of consumption profiles.
Background
The use of drugs without a medical prescription has become a global public health problem. Consumption of one pharmacological class of drugs—psychotropics—has recently increased among the general population[1]. These drugs are characterized as chemical substances that act on the central nervous system and produce temporary changes in a person’s perception, mood, state of consciousness, and behavior[2] and are generally used to treat mental health disturbances and related problems[3].
There is a wide variety of psychotropics, including opioid analgesics, anxiolytics and sedatives, general anesthetics, antiepileptics and anticonvulsants, antipsychotics, antidepressants, and mood stabilizers, among others[4]. Among these drugs the following categories stand out due to a higher rate of consumption: tranquilizers, which are mainly central nervous system depressants; stimulants, which are often indicated for the treatment of attention-deficit/hyperactivity disorder, and narcolepsy[5]; antidepressants, which are used clinically to treat multiple psychiatric disorders, and depression[5]; opioid analgesics, which mainly affect the central nervous system[6]; and opioid antitussives, like codeine, which have a moderate analgesic effect (depression of the central nervous system) and suppress the cough reflex[6].
Consumption of these drugs without medical supervision exposes people to a wide range of potential adverse reactions, including sleep disorders, irritability, panic attacks, depression, and motor and memory alterations[3]. Long-term use has been linked to brain damage; disorders of the central nervous system such as psychosis and various personality and mood disorders; and an increased risk of suicide[7]. Risk of these effects is exacerbated when psychotropic drugs are consumed with alcohol and/or other drugs such as marijuana. Psychotropics have a high capacity to create tolerance in the body, leading to dependence or addiction in some cases. Psychotropic drugs commonly associated with dependence or addiction include opioids, barbiturates, benzodiazepines, amphetamines, and anorectics[8].
According to data from the Chile’s Tenth National Study on Drugs in the General Population (2014), the most common way of obtaining psychotropics without a prescription (mainly tranquilizers) in the Chilean population 15 to 64 years old was through third parties without payment (45.4%), followed by “Other” (not specified in the survey), or through the Internet (20.2%), purchased at open-air markets (15.2%), and purchase at pharmacies (8.8%)[9]. A study conducted in Argentina in 2017 showed the main way to obtain nonprescription psychotropics in that country was through a friend (44%), on the street (23.8%), and at a pharmacy (22.4%)[5]. The same study indicated 49% of the Argentine population 12 to 65 years old tended to consume nonprescription psychotropics occasionally, whereas 44.2% consumed them several times per week, with average consumption estimated at 6 days per month[5].
In the United States, the 2014 National Survey on Drug Use and Health collected data on nonprescription use of tranquilizers, stimulants, and sedatives, and results indicated that among Americans 12 years or older (2.5% of the population) 6.5 million likely used a psychotropic drug during 2014[9],[10]. In Latin America, Haiti reported the highest prevalence of nonprescription tranquilizer consumption (lifetime, and in the last year and month during 2011) (6%)and nonprescription stimulant consumption (3.5%) among high school students[7]. In Argentina, reported prevalence for 2017 was 0.7% for nonprescription tranquilizers and 0.09% for nonprescription stimulants[5]. According to statistics from Chile’s National Service for the Prevention and Rehabilitation of Drug and Alcohol Use (SENDA), 191 000 people used psychotropic drugs without a prescription in 2014. Also, 56.3% of students reported using tranquilizers without a prescription for the first time before the age of 15[3]. Another study conducted in Santiago more than 20 years earlier (1991) found a prevalence of 28.9% for self-administered nonprescription psychotropics[11].
Several studies have suggested a relationship between the consumption of nonprescription drugs and various socio-demographic factors[12],[13], including age, sex, education level, and socioeconomic level[12]. These studies also describe a relationship between nonprescription drug use and alcohol and tobacco consumption[14]. Other investigations have described correlations between nonprescription psychotropic use and factors such as the absence of chronic illness, high education level, and female sex, all of which were associated with an increase in the consumption of these types of drugs[13].
In Chile, consumption of psychotropics without a prescription, especially tranquilizers, increased from 3.9% in 2014 to 4.2% in 2016[15]. A comparison of this increase to figures from the Toxicological Information Center of the Pontifical Catholic University (Santiago) suggests most cases of intoxication (57.1%) involved this class of drugs, especially those that act on the central nervous system, which was associated with 50.9% of all cases of drug intoxication in 2007[16].
The objective of this study was to determine the factors associated with the consumption of nonprescription psychotropic drugs in the general Chilean population using data from SENDA’s 2014 survey.
Methods
Data source and study population
A descriptive study was performed using data from the Tenth National Study on Drugs in the General Population (2014), conducted by SENDA to describe the magnitude of licit and illicit drug consumption in Chile, including consumption trends at the national and regional level[9]. The study was carried out between October 2014 and January 2015 and included an in-person survey of a total of 19 512 people 12 to 64 years old of both sexes and different socioeconomic levels. The sample was nationally representative. The coverage of the study (108 urban communities with a population of more than 30 000 inhabitants) corresponds to approximately 70% of the national population. The sample was provided by Chile’s National Statistics Institute based on random selection of blocks and residences followed by random selection of inhabitants of the selected residences. Individuals living on the streets or in institutions such as prisons and hospitals were excluded. The survey response rate was 69.6%, and the cooperation rate was 88.1%, while the rejection rate was 7.8%[9].
Ethics
This study used a publicly available database obtained from a division of the Government of Chile (SENDA). The data used were confidential and anonymous in accordance with the provisions of Law No. 17-374, Article 29[17], on statistical confidentiality. Therefore, no ethics committee approval or informed consent of participants was required to conduct this study.
Study variables
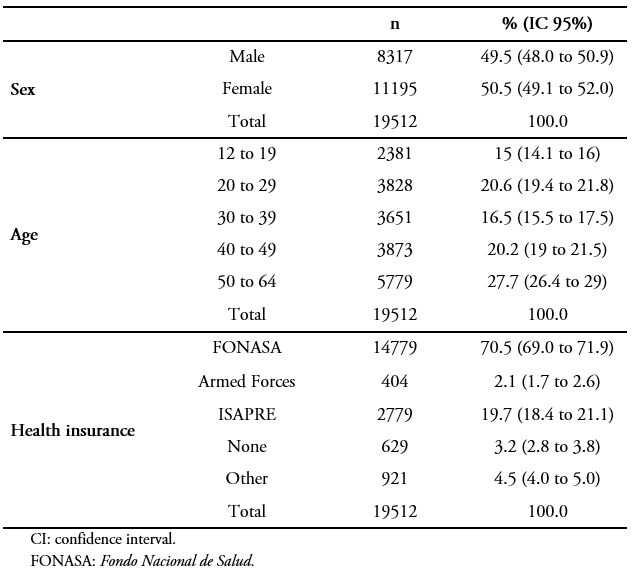
The following socio-demographic variables were considered: sex, age group (12 to 19, 20 to 29, 30 to 39, 40 to 49, and 50 to 64 years); type of health insurance (National Health Fund or FONASA, the public agency that administers government health care funding in Chile to cover beneficiaries directly[18]; Instituciones de Salud Previsional (ISAPRE), a group of private insurers that provide health care coverage through individual contracts[19]; Fuerzas Armadas y de Orden, which covers the health needs of Chile’s military personnel and law enforcement, and their dependents; “Other,” and “None,” for those with no health insurance). Health behavior variables were also incorporated, including the consumption of illicit drugs (marijuana, cocaine, and crack during the last year); alcohol (during the last month); and tobacco (at least one cigarette in 20 or more days during the last month). General self-perceived health was also included and this was based on a person’s description of their overall health status during the last 12 months, categorized for this study as “good” or “poor.”
Consumption of nonprescription psychotropics in the last year was used as the dependent variable and defined as the use of tranquilizers, stimulants, opioid analgesics, antidepressants, and opioid antitussives without a medical prescription (see Annex).
Data analysis
This study described the characteristics of the sample population (people 12 to 64 years old of both sexes and different socioeconomic levels) and estimated the general prevalence of consumption of psychotropic drugs without prescription and by pharmacological group by applying expansionist factors due to the complex sample design. Hypothesis tests were used to analyze the association of self-perceived health with consumption of nonprescription psychotropics. To analyze the association between variables a multivariate logistic regression model was conducted to determine 1) the probability of consuming psychotropics without a medical prescription during the last year and 2) the effect of explanatory variables such as socio-demographic characteristics and health behaviors. The odds ratios (ORs), with 95% confidence intervals (CIs), were calculated. The Hosmer–Lemeshow test was used to determine goodness-of-fit20. Finally, to identify consumption profiles, a homogeneity analysis was performed on the subgroup that reported having used psychotropics without a medical prescription during the last year.
Results
As shown in Table 1, of the 19 512 people included in the study, 50.5% were women (average age: 38.6 years; 95% CI: 38.0 to 39.2) and 49.5% were men (average age: 36.8 years; 95% CI: 36.1 to 37.59). Use of marijuana, cocaine, or crack (past year), tobacco (20 or more days in past month), and alcohol (past month) is shown in Figure 1. As shown, alcohol consumption was highest at 48.9%. Of all illicit drug use, marijuana consumption was highest at 11.5% (95% CI: 10.6 to 12.65).
 Full size
Full size 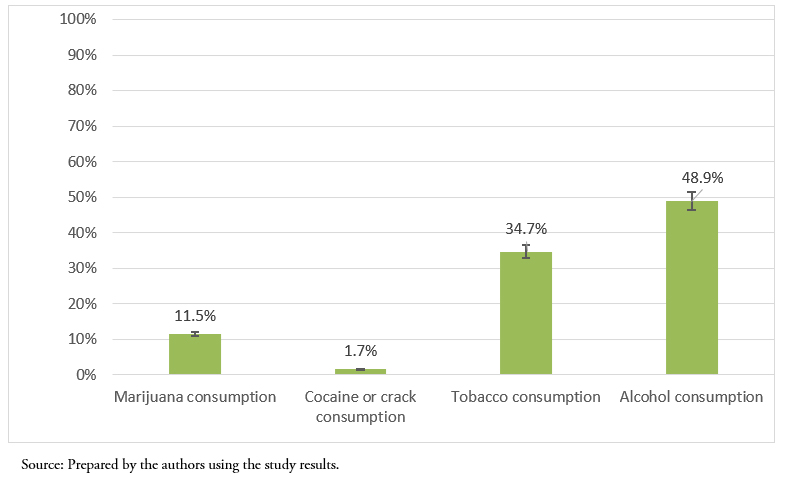 Full size
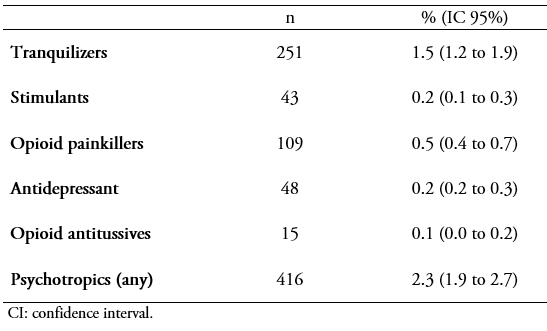
Full size The prevalence of consumption of any nonprescription psychotropic in the last year was 2.3% (95% CI: 1.9 to 2.7) (Table 2). Broken down by pharmacological group, consumption of nonprescription tranquilizers was highest at 1.5% (95% CI: 1.2 to 1.9). As shown in Figure 2, 56% (95% CI: 46.8 to 64.7) of those who consumed nonprescription psychotropics had a “good” positive self-perception health, a lower proportion compared to those who did not report consuming this class of drug.
 Full size
Full size 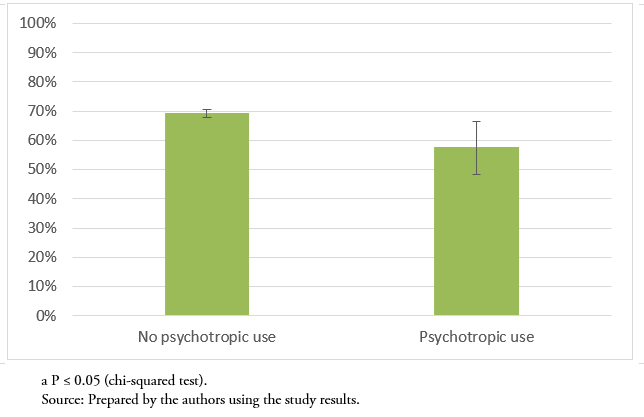 Full size
Full size The logistic regression analysis (shown in Table 3) reveals a greater probability of psychotropic use without a medical prescription among marijuana users (OR: 3.04; 95% CI: 2.32 to 3.97) and users of cocaine or crack (OR: 3.74; 95% CI: 2.45 to 5.70) compared to those who do not use any of the three latter substances. A smaller association with use of nonprescription psychotropics was found for age, with women in two age groups more likely than those in other age groups to use these drugs: 20 to 29 years (OR: 1.49; 95% CI: 0.98 to 2.26) and 40 to 49 years (OR: 1.81; 95% CI: 1.19 to 2.75). When the older age group was compared to the younger age group, nonprescription psychotropic drug use was higher for those who 1) consumed tobacco (20+ days in last month) and/or alcohol (last month) and 2) reported a “poor” self-perception health.
 Full size
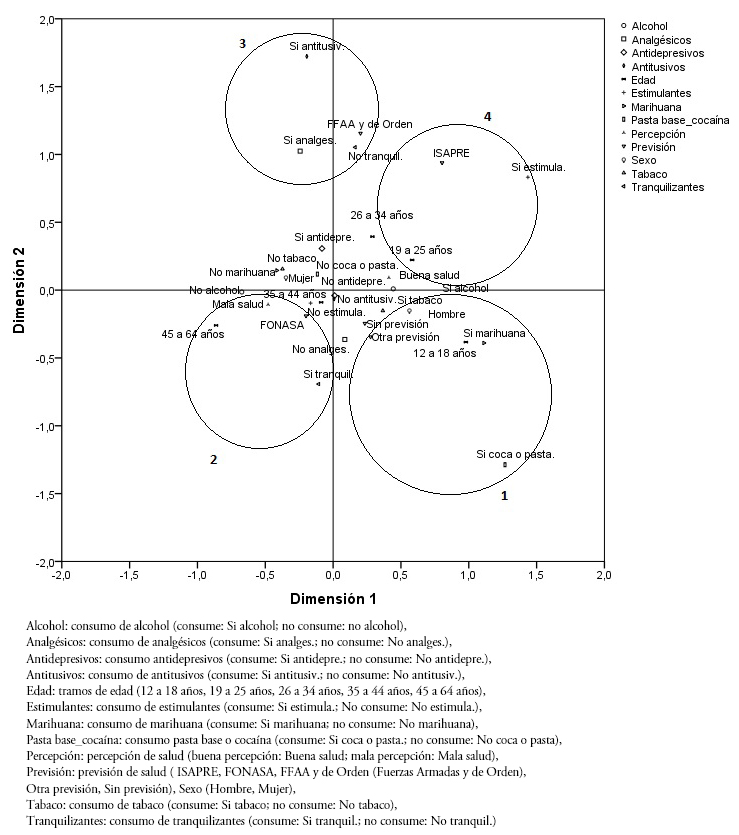
Full size In the homogeneity analysis, four groups or profiles of consumers of nonprescription psychotropic drugs were identified (Figure 3). The first group, male adolescents 12 to 18 years old, was correlated with the use of marijuana, cocaine, or crack. The second group, the male and female population 45 to 64 years with poor self-perceived health, was correlated with the use of tranquilizers. The third group, the population assigned to the Armed Forces and law enforcement pension and benefits system, was correlated with the consumption of analgesics and antitussives. The fourth group, 19 to 25-year-old women that belonged to the ISAPRE insurance system, was correlated with the consumption of stimulants.
 Full size
Full size Discussion
The prevalence of consumption of any nonprescription psychotropic in Chile was 2.3%, similar to what has been reported elsewhere in Latin America (e.g., in Costa Rica, which had a prevalence of 2.8%)[7]. Some countries in the region have a lower rate of consumption prevalence than Chile’s, however, including Argentina 1.5%[21], as well as the Dominican Republic (0.03%) and Mexico (0.4%)[7]. Consumption prevalence in the United States is 0.5%)[7]. The higher consumption prevalence for these drugs found in people 50 to 64 years old in this study (27.7%) is similar to what has been reported previously in the literature[11]. According to one study, there is a higher prevalence of self-medication in people 40 to 60 years old versus other age groups (38.8%)[11]. Higher consumption of psychotropics in this age range is likely related to the fact that this group is a key part of the working population and thus has a greater tendency to experience stress from work-related pressure[22],[23].
The pharmacological groups with the highest prevalence were tranquilizers, with a prevalence of consumption of 1.5%, and opioid analgesics, with a consumption prevalence of 0.5%. The values for tranquilizers are similar to those previously reported in the literature (0.7% in Argentina[5] and 0.3% in Mexico[7],[5]). The data for opioid analgesics are similar to previously published results that estimated the prevalence of nonprescription consumption for this group of drugs of 0.6% to 0.8% of the global population 15 to 64 years old[24] and 1.7% of Americans over the age of 12[7]. As opioid analgesics are used to treat moderate to severe pain, their misuse has become a major public health problem, due to the risk of coma and cases of fatal respiratory suppression that results from overdoses[25]. Misuse of tranquilizers has also become problematic; recent reports show an exponential increase in their consumption, which could be explained by an increase in psychiatric pathologies[26].
This study also found an increase in the probability of nonprescription psychotropic use in women, and the evidence indicates they have higher rates of consumption than men (OR: 3.44; 95% CI: 1.37 to 8.66)[12],[13],[27],[28],[29]. This behavior may be associated with women presenting more symptoms than men due to their physiological characteristics, their social role, and their greater sensitivity to the symptoms[13]. Other studies show a relationship between the consumption of psychotropic drugs and long-term unemployment, indicating a greater tendency to experience a deterioration of mental health among those who remain unemployed for an extended period. This situation is likely more common among women because women in Chile generally have a more precarious socio-labor situation than men[2]. This higher rate of psychotropic consumption might also be explained by cultural differences between men and women, with the latter group generally more predisposed to recognize the presence of disease and thus seek medical attention. In addition, it is often seen as more socially acceptable for a woman to see a doctor than a man. As a result, women tend to receive more prescriptions for psychotropics than men, and doctors are more likely to prescribe them for women[30]. It is also important to point out the great addictive power of this class of drug, which has been demonstrated in several studies in European countries that found that more than one-third of women who have been prescribed a psychotropic drug at some point time in their lives become regular (monthly) consumers of these drugs[24], which leads to increased overall consumption, often without a prescription.
The data found in this study for the group that consumes licit (alcohol, tobacco) and illicit substances (marijuana, cocaine, and crack) corresponds to findings from past investigations that show that people with this behavior are more likely to use nonprescription psychotropics[28]; these substances generate some degree of dependency, which is associated with an increased risk of substance abuse[29]. Also, epidemiological evidence suggests that tobacco use is a risk factor for chronic pain[14],[31], which encourages the consumption of this type of drug.
The results obtained on the relationship between nonprescription psychotropic use and self-perception health were consistent with data previously reported in the literature (OR: 0.65; 95% CI: 0.42 to 0.99)[13]. Individuals with a “poor” or low self-perception health status are more likely to consume these drugs without a prescription[29]. According to Papakosta et al., this happens because people with a low self-perceptions health often have underlying pathologies and thus tend to use more drugs (both with and without prescriptions) that may in turn negatively affect their health status[13]. However, some studies have found an association between self-medication and an excellent/“good” self-perception health (OR: 2.38; 95% CI: 1.74 to 3.26), especially among those who take analgesics without a prescription, possibly due to the fact that their use of these drugs without a prescription is often a response to mild or sporadic pain[14].
The psychotropic consumption profiles or groups identified through the homogeneity analysis carried out in this study found the use of illicit drugs was associated with adolescent males 12 to 18 years old. Findings from previous studies examining adolescents provide some explanation for this result, pointing to the ease of access to tobacco and alcohol for this age group[32]. Also, adolescents often abuse recreational drugs at a higher rate than adults (for both licit and illicit drugs)[2]. In 2012 the United Nations Office on Drugs and Crime noted that illicit drug use was highest among young men in urban settings[24] and that adolescent males over the age of 12 were more likely to be current users of these substances[7]. A partial explanation for the second consumption profile identified in this study (use of tranquilizers in men and women 45 to 64 years old that reported own health as “poor”) may be found in evidence that suggests the highest consumption of this pharmacologic group of drugs occurs between the ages of 25 and 34[7]. During this period, the consumption of psychotropic is likely triggered by episodes of anxiety resulting from pressure from work, family issues, and the desire to achieve a balance between the two, and this behavior may persist as the users' age. Among the elderly (ages 60 and up), these periods of distress would likely be triggered by certain age-related situations, such as physical and psychological deterioration and loneliness[7]. For the third consumption profile, the literature describes how military personnel/law enforcement who have been repeatedly exposed to stressful situations are at an increased risk of developing drug and substance abuse problems and are more likely to become involved for the first time with alcohol or drug abuse every week. As a result, this group abuses drugs, especially opioid analgesics, at a greater rate compared to the civilian population[33]. Finally, partial explanation for the association with psychotropic use found for the fourth consumption profile or group may be found in past studies have shown that in Latin America—South America, in particular—stimulant use is often associated with efforts to lose weight[24]. In Argentina, more than 37% of young people 18 to 34 years old consume this type of drug without a prescription, with higher use occurring in those 18 and 24 years old[7]. Within this age range the consumption of psychotropics might be justified as a way of maintaining performance in a demanding life context both in study and in work[7].
Conclusion
In Chile, few research studies have examined the consumption of psychotropic drugs among the general population. This study provides an estimate of this consumption, based on data from a population survey with national representation.
One of the main limitations of the study is the source of the data (a survey on the use of drugs and alcohol). The survey data do not include fundamental variables that could be related to the consumption of nonprescription drugs such as the presence of chronic diseases, symptoms, or motives associated with consumption, etc. Due to this limitation, future studies that consider and carefully examine these variables should be conducted to contribute to a better understanding of the consumption of nonprescription drugs in Chile.
The results of this study provide evidence on the relationship between the consumption of psychotropics and certain socio-demographic factors, risk behaviors, and self-perceptions health. They also allowed for the identification of the consumption profiles that are essential in addressing the phenomenon of nonprescription psychotropic use, which has become an important public health problem both nationally and globally in recent years. This problem has also increased due to these drugs’ addictive properties, which are exacerbated when consumption is not controlled by medical personnel. The consequences of such unsupervised use can be severe and can cause premature death. This study identified variables and consumption profiles that can be used to better inform the design of public policies that need to consider the distinct elements of the diverse population groups of both adults and youth that are consuming nonprescription psychotropic drugs in Chile.
Notes
Author roles and contributions
ND: conceptualization, methodology, validation, formal analysis, research, preparation of the manuscript, visualization, and administration of the project.
CV: conceptualization, methodology, validation, formal analysis, writing (review and editing), supervision, and project management.
BM: conceptualization and design.
LH: conceptualization, formal analysis, and writing (review and validation).
Acknowledgments
The authors would like to thank the National Service for the Prevention and Rehabilitation of Drug and Alcohol Consumption (SENDA), which reports administratively to the Ministry of the Interior and Public Security of Chile, for making the database available.
Funding
The authors state that there were no external sources of funding.
Data and material availability
The datasets generated and/or analyzed in this study are available on the SENDA website (http://www.senda.gob.cl/observatorio/estadisticas/?page_id=739).
