Research papers
← vista completaPublished on June 30, 2021 | http://doi.org/10.5867/medwave.2021.05.8221
Clinical and tomographic characterization of patients with interstitial lung disease at the Trujillo Regional Teaching Hospital, Peru
Caracterización clínica y tomográfica de pacientes con enfermedad pulmonar intersticial del Hospital Regional Docente de Trujillo, Perú
Abstract
Objective To determine the main clinical and tomographic characteristics of patients with diffuse interstitial lung disease at Trujillo Regional Teaching Hospital.
Methods Case series. Tomographic examinations and clinical data were obtained from patients with interstitial pulmonary disease who attended the pulmonology service of Trujillo Regional Teaching Hospital. The information collected was recorded and systematized in Excel. For the statistical analysis, SPSS 23.0 program was used.
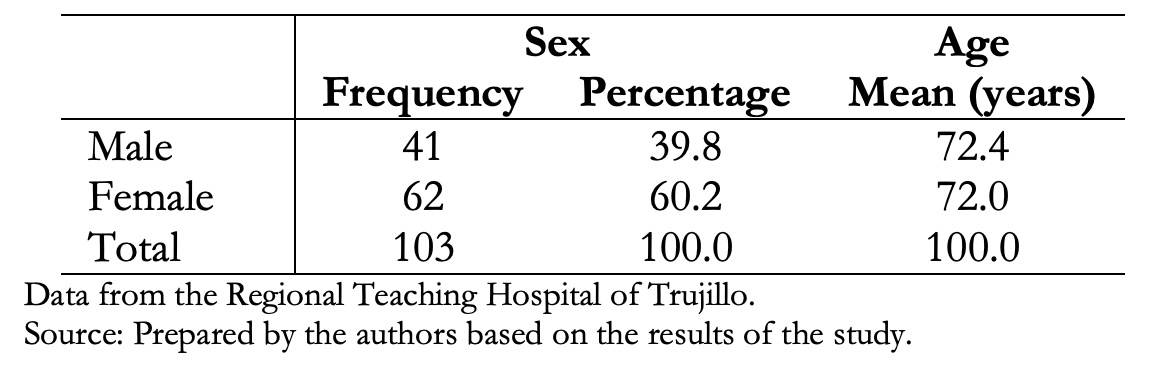
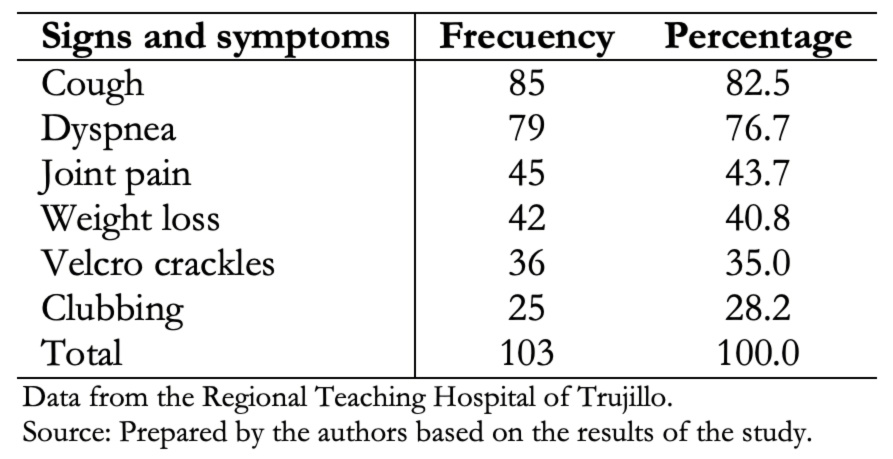
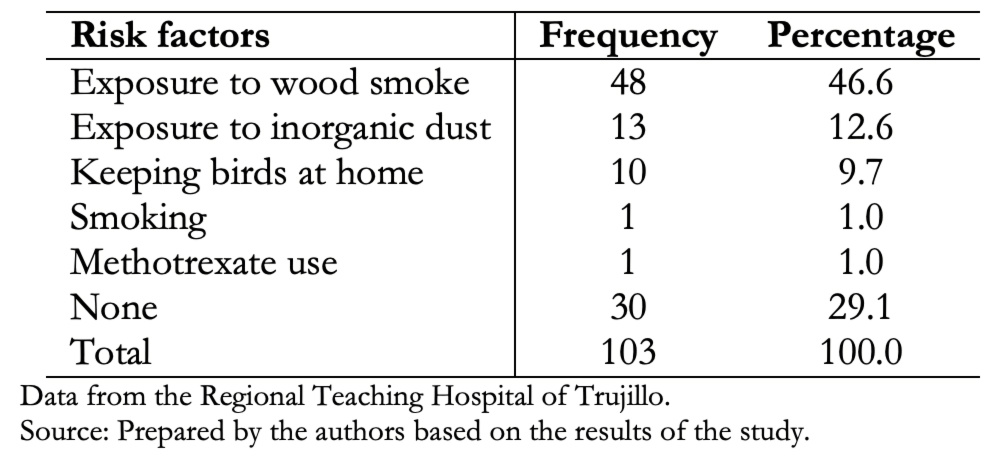
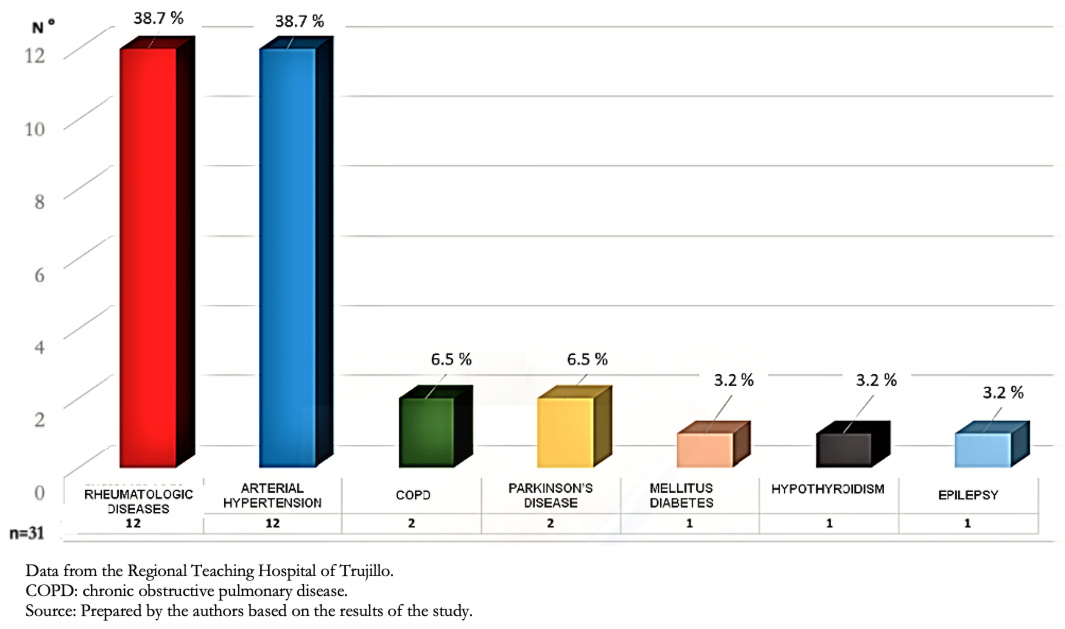
Results Data from 103 patients were obtained, of which 60.2% were female, and 39.8% were male. The average age was 72 years for both groups. Main clinical manifestations were cough (82.5%), dyspnea (76.7%), joint pain (43.7%), weight loss (40.8%), velcro crackles (35%) and digital clubbing (28.2%). Exposure to wood smoke was present in 46.6%, exposure to inorganic dust in 12.6% and fowl ownership in 9.7% of cases. Thirty-one (30.1%) patients presented comorbidities. Among these, rheumatic diseases and arterial hypertension were the most frequent. Non-specific interstitial pneumonia pattern was present in 26.2% of the cases; probable usual interstitial pneumonia in 16.5%; organized type in 12.6%; usual interstitial in 10.7%; acute interstitial in 2.9% and 27.1% had no defined tomographic pattern.
Conclusions In the studied population, clinical and tomographic characteristics of interstitial lung parenchymal diseases are variable in magnitude and forms of presentation. Female sex and exposure to fuels were the most frequent associated factors. Connective tissue diseases could also explain study findings.
Main messages
|
Introduction
Patients with interstitial lung disease usually present respiratory distress due to decreased distensibility, increased interstitium stiffness and alveoli obliteration. These scenarios come with generalized inflammation, fibrosis of alveolar walls, pulmonary vasculature, and interstitium, altering diffusion and decreasing ventilation/perfusion ratio [1].
The main clinical manifestations of interstitial lung disease are cough, dyspnea, joint pain, weight loss, velcro crackles, and clubbing. These occur in varying magnitude and frequency, depending on the underlying type of interstitial lung pathology [2],[3],[4]. There are more than 300 conditions associated with the different causes of interstitial lung diseases [1]. These include connective tissue disease [5],[6],[7], hypersensitivity pneumonitis, pneumoconiosis, sarcoidosis, organizing pneumonia, interstitial lung disease associated with occupational exposures, and unclassifiable interstitial lung disease. The most common interstitial diseases are idiopathic interstitial pneumonia, sarcoidosis, and extrinsic allergic alveolitis [8],[9]. Idiopathic pulmonary fibrosis is the most common subtype of idiopathic interstitial pneumonia with severe and progressive presentation [10],[11].
Epidemiological data on interstitial lung disease vary widely due to differences in data collection methods and classifications. The estimated incidence of interstitial lung disease is 31.5 cases per 100 000 males and 26.1 cases per 100 000 females [12]. On the other hand, throughout Europe and North America, the estimated incidence of idiopathic pulmonary fibrosis varies between 2.8 and 19 cases per 100 000 persons per year [13],[14]. In Peru and Latin America, we do not have epidemiological information that allows us to estimate the full magnitude of the problem. In the region, information is being collected through the Idiopathic Pulmonary Fibrosis Registry, sponsored by the Latin American Thoracic Association (ALAT).
Multiple exposures, such as environmental pollution, accelerates lung function decline. However, there is scarce information on its role in the development and progression of early stages of interstitial lung disease [15]. Exposure to elemental carbon may increase the risk of progressive interstitial lung disease [16]. Associations with other forms of environmental pollution, such as particulate matter and ozone, are not yet clearly defined [15],[16]. On the other hand, hypersensitivity pneumonitis (a type of interstitial lung disease) is most frequently caused by exposure to avian proteins (bird fancier’s lung), fungi and other microorganisms. Among the latter, thermophilic actinomycetes species (farmer's lung) stand out [17].
To unify the nomenclature and definition criteria used and to favor research, in 2015, the American Thoracic Society and the European Respiratory Society formed the ERS/ATS Task Force on Undifferentiated Forms of Connective Tissue Disease-associated Interstitial Lung Disease. This team proposed the terminology for the Interstitial Pneumonia with Autoimmune Features, IPAF [2],[3],[4].
High-resolution computed axial tomography is the standard imaging method used [18] for lung and small airway diseases [19]. Current technical advances in new computed tomography equipment allow simultaneous acquisition of slice data from multiple detector rows. High-resolution imaging for complete chest study during a single apnea phase, volumetric acquisition, and the use of multiplanar reconstructions provide additional information to conventional studies [20],[21]. For the interpretation and determination of tomographic patterns and different types of pneumonia, a multidisciplinary consensus is recommended for a better approach to diagnose interstitial pneumonia [4],[22].
In Peru, the prevalence of interstitial lung disease, the most affected groups and its epidemiological characteristics are unknown. For this reason, this study aimed to determine tomographic patterns, main clinical manifestations, risk factors and comorbidities of patients with interstitial lung disease, treated at the Trujillo Regional Teaching Hospital. This is a third-level hospital center belonging to the Ministry of Health, and attends to a large proportion of public health patients. In addition, it trains undergraduate and graduate students. This information is necessary for proper diagnosis, specific therapeutic management – and most importantly – preventive measures.
Methods
Data sources
We analyzed the clinical history and tomographic information of patients with a diagnostic hypothesis of interstitial lung disease seen in the pulmonology service of the Trujillo Regional Teaching Hospital. Data was obtained between 2 January 2 and 30 December 2019.
Methods and techniques
We did a case series. Patients with clinical history and chest tomographic studies who attended the pulmonology service were selected. We also included patients referred from lower complexity health facilities and patients referred from other hospital services that needed diagnosis and management referring to respiratory symptomatology. Tomographic studies were reviewed in those who had them requested and those who did not.
The determination, interpretation and qualification of the tomographic patterns of interstitial lung disease were performed by pulmonologist investigators trained in reading chest tomography and correlated with the respective radiological report. If there were disagreements, the tomography was reread and reviewed with the radiologists who had reported the studies, based on the consensus of the American Thorax Society, Europe Respiratory Society, Japan Respiratory Society and ALAT. There was a recollection of study’s predefined clinical characteristics for patients that met inclusion criteria. This included demographic data, clinical data, risk factors, and comorbidities noted in the respective medical records and an ad hoc registry.
The information obtained was recorded and systematized by Microsoft Excel spreadsheets. SPSS 23.0 program (Statistical Package for the Social Sciences 23) was used to analyze age, sex and tomographic patterns of interstitial pneumonia. To these, we added the predefined clinical characteristics for interstitial lung disease (i.e., cough, dyspnea, joint pain, weight loss, auscultation of velcro crackles and clubbing).
Inclusion criteria
- Patients older than 15 years of age.
- Patients with high-resolution tomographic chest studies with or without contrast, printed on plates or CD.
- Medical history with demographic data and clinical characteristics of patients with interstitial lung disease.
Exclusion criteria
- Patients with incomplete data.
- Patients without high-resolution tomographic chest studies.
Results
Data were obtained from 112 patients with a presumed interstitial lung disease diagnosis, of which 103 (92%) had clinical history data and tomographic studies of interstitial lung disease that met the inclusion criteria. The majority were females (60.2%), and there were no age differences, as shown in Table 1.
 Full size
Full size Cough and dyspnea were the most predominant symptoms. Auscultation of velcro crackles was the most frequent clinical sign, as shown in Table 2.
 Full size
Full size Table 3 shows that exposure to wood smoke was the most frequent risk factor (46.6%). However, in 29.1% of patients with interstitial lung disease, no risk factor was obtained.
 Full size
Full size Of the total, 31 patients had comorbidities (30.1%), and 72 had none (69.9%). Figure 1 shows that rheumatologic diseases and arterial hypertension were the most frequent comorbidities.
 Full size
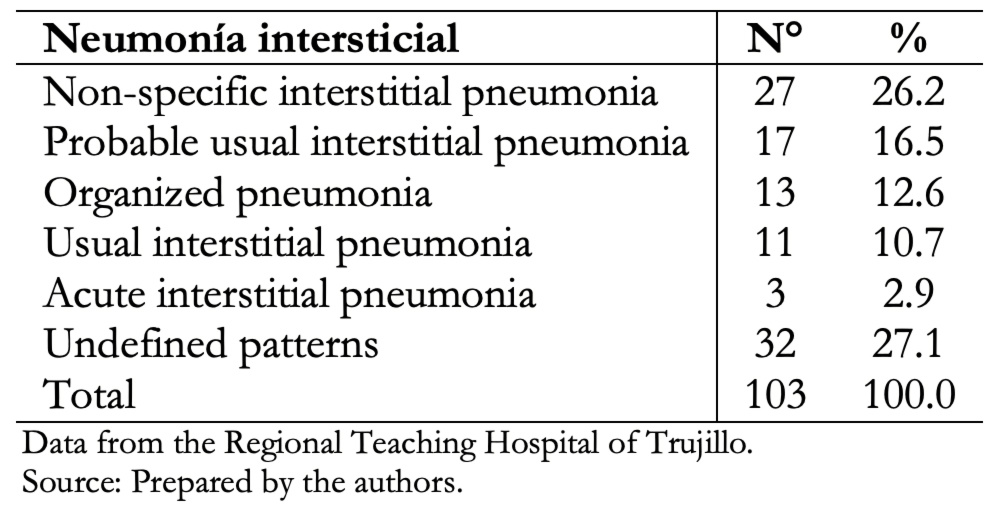
Full size In our study, non-specific interstitial pneumonia tomographic pattern was the most frequent (26.2%), and the usual interstitial pneumonia pattern was 10.7% of the cases, as shown in Table 4.
 Full size
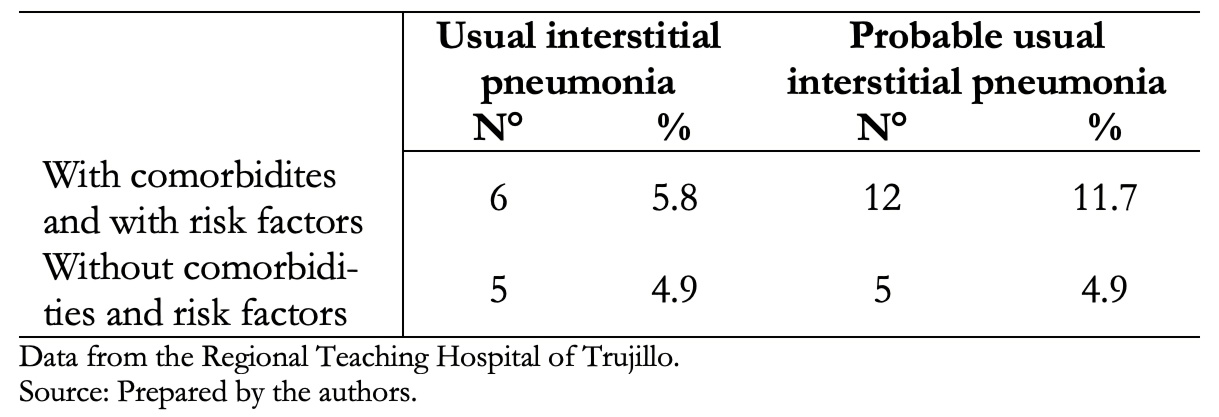
Full size Table 5 shows that 5.8% of patients with usual interstitial pneumonia tomographic pattern and 11.7% with probable usual interstitial pneumonia had comorbidities and risk factors.
 Full size
Full size Discussion
This study aimed to identify the main demographic, clinical, risk factors, comorbidities and tomographic characteristics associated with interstitial lung disease in patients attending the Trujillo Regional Teaching Hospital. This is one of the first descriptive studies at a regional level to assess this issue. Among 103 patients studied, females were more frequent. In addition, the average age was 72 years, with no differences between genders.
The present study is similar in age but different in gender, as reported by Diaz and Miranda in Huancayo, Peru [23]. In contrast, Dueñas and colleagues [24] found dissimilar results in Colombia, in which lower mean age (41.7 years) and males were predominant.
These differences could be explained because the prevalence of certain interstitial pneumonias (related to age and gender onset, which depends on work activity, environmental factors and connective tissue diseases) can appear at any stage of life and without distinction for race, age, education or sex. However, females and older adults seem to be the most affected as a result of the aging process [13],[25],[26],[27],[28].
Dyspnea and cough are the most frequent symptoms in patients with interstitial lung disease, although they may be asymptomatic and discovered by incidental findings [29]. Common signs include velcro crackles and digital clubbing. In the present work, it was also observed that such manifestations were the most prevalent, in addition to joint pain. The magnitude of these clinical manifestations would be associated with work activity, underlying pathology (such as connective tissue diseases) and environmental risk factors related to female predominance, as shown in the present study [14],[23],[30].
We observed that the main associated risk factors were wood smoke and inorganic dust exposure. Diaz and Miranda [23] report similar results. In Colombia, Restrepo and colleagues – based on histological studies in animal experiments and clinical findings and transbronchial lung biopsies in humans – proved that the smoke cooking produced by firewood causes a pneumoconiosis type lung damage [31]. In Costa Rica, it was shown that wood smoke is a major source of contamination, mainly in rural areas where it is used for household combustion. Therefore, this study suggests wood smoke is an important factor in the genesis of interstitial lung disease [32],[33]. In our work, the association of wood smoke with interstitial lung disease could be explained by female sex predominance; and this may be because they are more likely to be exposed to biomass elements due to domestic activities. In Peru, an average of 23% of women prepare their food with biomass fuels [34].
Bird keeping was present in 9.7% of the cases, which is also important to consider because of its relationship with interstitial lung disease. Exposure by direct contact with birds is a frequent and recognized form of hypersensitivity pneumonitis, which is a type of interstitial lung disease. Prolonged exposure to avian proteins, which are the main antigenic sources, causes constant inflammation leading to irreversible pulmonary fibrosis over time [35]. Typical tomographic findings include fibrosis with reticulation, architecture distortion, bronchiectasis and traction bronchiolectasis. The honeycomb pattern has been reported in 16 to 69% of cases of chronic hypersensitivity pneumonitis. In contrast to patients with idiopathic pulmonary fibrosis, the honeycomb pattern rarely has basal predominance [36]. In our study, domestic bird keeping could be related to our tomographic findings [37],[38],[39].
Smoking is a prevalent risk factor for interstitial lung disease, according to Behr J and colleagues [38] and Rodas and Espinoza in Guayaquil, Ecuador [28]. On the other hand, Xaubet A et al. differ from our findings [40]. This difference may be explained for two reasons. Firstly, because smoking prevalence for people over 15 years old in the northern region of Peru (where we conducted the study) is 15% on average, which is low compared to other areas. Secondly, because smoking is more frequent among young men. In women, the prevalence is between 0.6 and 2% in this age group [34]. Our study population was predominantly women over 70 years of age, and we had only one smoking-related event. Also, other studies have found an important association with drugs such as methotrexate [41]. In our study, we had only one patient related to methotrexate use.
Rheumatologic diseases and essential arterial hypertension were the most prevalent comorbidities of our study. These results are similar to Gaudiano J and colleagues in Uruguay. They mention a high frequency of women with rheumatologic diseases, especially connective tissue diseases as the main disease triggers [42],[43]. This is different from Buitrón et al. in Huancayo, where diabetes mellitus was present in most cases [44]; and also different from other studies, where they found other important comorbidities such as gastroesophageal reflux [45], chronic viral infections [46],[47],[48], hepatitis C [49] or family history of interstitial lung disease [51],[52],[53].
In the present study, the non-specific interstitial tomographic pattern was most prevalent among interstitial pneumonia. Imaging manifestations were followed in prevalence as probable usual interstitial pneumonia, organized pneumonia, usual interstitial pneumonia, and acute interstitial pneumonia. In addition, 27.1% of patients did not have a defined tomographic pattern and had variable forms and causes of the interstitial involvement. This last finding is half of what was found by Gaudiano J and colleagues in a tertiary hospital in Uruguay [43]. The prevalence of interstitial pneumonia tomographic patterns will depend on the frequency of underlying pulmonary pathologies. In our study, tomographic pattern results could be related to the high frequency of females and joint pain, which may correspond to a high prevalence of connective tissue diseases [54].
Our imaging findings of usual interstitial pneumonia and probable usual interstitial pneumonia without comorbidities and risk factors, could correspond to cases of idiopathic pulmonary fibrosis. Some reports say that 50% of usual interstitial pneumonia is idiopathic pulmonary fibrosis [55]. The remaining cases of usual and probable usual interstitial pneumonia could correspond to other pathologies associated with interstitial lung involvement, such as connective tissue diseases [55].
Recommendations
As a result of our work, we suggest conducting new regional studies to assess the prevalence of interstitial lung diseases and their respective associations with risk factors, etiologic agents, and underlying comorbidities.
Limitations
It should be mentioned that the study has limitations, which could affect results interpretation. For example, because it was a descriptive observational study, biomarker studies were not performed (such as autoantibodies) so that the prevalence of connective tissue diseases cannot be assessed with great precision. Also, we did not quantify exposures to risk factors such as biomass fuels, and there were no pathological anatomy studies.
Conclusions
In the studied population, clinical and tomographic characteristics of interstitial lung parenchymal diseases are variable in magnitude and forms of presentation.
Female sex and exposure to biomass fuels (wood smoke) were the most frequent factors associated with interstitial lung diseases. These study findings could also explain the high prevalence in women with joint pain and connective tissue disease characteristics.
This is relevant information for decision-making because there are modifiable factors that can curtail the progression of interstitial lung diseases.
Notes
Authorship contributions
LARH: conceptualization, validation, research, original draft writing, editorial review and editing, visualization, oversight, project management, funding acquisition. LACU: research, resourcing, fund acquisition. JSHV: methodology, formal analysis, resources, writing original draft, review and editing, oversight, acquisition of funds. JLCP, ONAH: research and acquisition of funds.
Competing interests
The authors completed the ICMJE conflict of interest statement and declared that they received no funding for the completion of this article; have no financial relationships with organizations that may have an interest in the published article within the past three years; and have no other relationships or activities that may influence the publication of the article. Forms can be requested by contacting the corresponding author or the Editorial Committee of the Journal.
Funding
Funding was provided by the authors; no external funding was received.
Ethics
This study was authorized by the Ethics Committee of Trujillo Regional Teaching Hospital Office N° 203-2019, dated 9 December 2019, both for the management of information from medical records, tomographic studies, and research development.
Language of submission
Spanish.
