Research papers
← vista completaPublished on August 27, 2021 | http://doi.org/10.5867/medwave.2021.07.8452
Psychometric validation of the Peruvian version of a short scale to assess psychological violence in health professionals: A cross-sectional study
Validación psicométrica de la versión peruana de la escala breve para evaluar violencia psicológica en profesionales sanitarios: estudio transversal
Abstract
Objective This study aimed to adapt a Peruvian version of the brief scale to assess psychological violence in health professionals (EVP-salud), exploring its validity and reliability properties.
Methods We made a cross-sectional study of psychometric evaluation conducted between January 2019 and February 2020. It involved the voluntary and anonymous participation of 316 health professionals and administrative workers from 17 health centers in Peru, who were administered the 22-item psychological violence scale. In addition, three other instruments were used to assess convergent and discriminative validity.
Results In contrast to other findings using similar instruments, the item composition of the abbreviated psychological violence scale converges on three components that assess isolation, intimidation, and belittling violence. This validation provides evidence of good fit in criterion and construct, explaining 66.7% of the accumulated variance and up to 54.3% when the final version is reduced to 13 items and three factors. The data reflect a high inverse association between psychological violence and intrinsic job satisfaction.
Conclusions The empirical results indicate psychometric properties of the instrument, with strong support in the validity and appropriate reliability according to the internal consistency indexes.
|
Main messages
|
Introduction
The workplace psychological violence is unknown due to the lack of standardization based on empirical evidence of those involved [1].
According to the International Labor Organization, the International Council of Nurses, the World Health Organization [2], and according to Li and collaborators [3], psychological violence in the workplace is an intentional action in which workers or their collectives are verbally assaulted, threatened and/or humiliated during their professional practice. This situation is exacerbated in healthcare due to the precarity of working conditions. The common denominator is psychosocial risk factors [4], with no differences between healthcare groups or between developed and underdeveloped countries [5],[6],[7].
Even though the recording of violent acts is suboptimal [8], it is known that one in 10 healthcare professionals is a victim of psychological violence. This situation harms mental health, including increased stress, insecurity, and exhaustion [9].
A virtual survey of 19 967 physicians, dentists, and nurses in Latin America (56.3% in Argentina, 15.8% in Mexico, 5% in Ecuador, 4% in Peru, and the rest in 18 other countries) showed that 66.7% (13,318/19,967) of the professionals were victims of violence [10]. In Peru, violence reached 36.2% (79/219), and conscious aggressions even came from the patients themselves [11].
The type of psychological violence (e.g., harassment, intimidation, and discrediting) has been studied in several work sectors in Mexico [12] and Spain [13]. In the latter, mental health and emergency units were the most exposed hospital areas to external and psychological violence. It was also found that violence decreases as work experience increases [13].
In Peru, violence at work has been evaluated with interpersonal conflicts and motivational demands in healthcare personnel [14]. A study indicates that stress and mobbing in the workplace have an economic impact that can reach 30% of the total costs of diseases and accidents, which is equivalent to 3.5% of the gross domestic product [15]. External workplace violence and mobbing were studied in Huaraz and Tacna hospitals, where 72% (23/32) of the physicians had suffered some type of aggression [16],[17]. In three hospitals in Arequipa, 84% (168/200) of the physicians had suffered external violence at some time during their working life [18]. In two hospitals in Trujillo, psychological and physical violence was found to occur in outpatient clinics and predominantly in women [11].
Overall, studies assessing workplace violence among physicians and nurses in Peru are mainly oriented towards external violence in specific geographic areas (Lima and four other cities in the country). Studies on psychological violence at work among health professionals at a national level are scarce.
In the last four years, external violence and its associated factors have been oriented towards patient care quality and professional satisfaction [19]. These studies have used Likert self-report questionnaires and multiple-choice or dichotomous questionnaires [10].
One helpful tool to assess verbal and physical violence at work is the aggressive behavior scale for healthcare workers made by Waschgler et al. [20]. This instrument consists of 10 items organized into two factors (psychological violence: 7 and physical violence: 3), with six-point Likert-type graduation. The minimum value (1) corresponds to "never in the last year" and the maximum value (6) to "daily"; this data explained 57.3% of the total variance with an α coefficient of 0.84.
The latter behavior scale has been used in the Spanish mental health field (n = 518 nurses), and its reliability by internal consistency has been determined by Llor and collaborators [13]. Another tool to assess violence at work is the inventory of violence and psychological harassment at work for 24 business lines made by Pando and collaborators [21]. These authors evaluated the internal consistency, concurrent validity, and construct validity of the 21-item instrument in Mexican workers (n = 307); and applied exploratory factor analysis to define its dimensions.
Acosta and colleagues [22] studied psychosocial conditions, violence, and mental health among Colombian doctors and nurses (n = 111) through the 22-item inventory of violence and psychological harassment at work [23]. This instrument was validated by applying exploratory factor analysis in 359 workers in the economic sector. Pando et al. [24] also applied exploratory and confirmatory factor analysis to determine the construct of the IVAPT-Pando instrument on violence and psychological harassment in service and industry sectors in Bolivia (n = 311 workers) and Ecuador (n = 309 workers).
Similarly, Diaz et al. (2015) [25] validated and standardized the inventory of violence and psychological harassment at work for the Chilean working population in the commerce, health, and education sectors, after semantic adaptation and content and construct validity analysis. This adaptation used data from 700 workers and applied exploratory factor analysis for 25 items in four components (isolation, intimidation, discrediting, and external violence). The authors also performed a convergent validation with the 12-item General Health Questionnaire and determined scales to diagnose violence and psychological harassment.
Perez [11] studied workplace violence in 219 health professionals in Peru, using a structured self-administered survey questionnaire with seven items. This survey describes the type of violence (physical and psychological), the triggering context, and the sequelae. Although neither its validity nor reliability has been reported, this questionnaire has been used in several Latin American countries [10].
Various techniques and instruments are used to assess and monitor the prevalence of psychological violence, including costs and impact [1]. Despite this, there is limited information regarding psychological violence in Peruvian health professionals; and this may be because:
1) Several structured and self-administered formats [10],[11] or the aggressive behavior scale of Llor et al. [13] have been validated for Spain, Mexico, Colombia, Ecuador, Chile, and Bolivia, but not for the Peruvian population.
2) These tools contain mostly items referring to external violence and few items related to psychological violence.
3) These instruments are oriented to the construction, education, commerce, industry, or security sectors.
4) These scales are oriented to determine the frequency of physical or psychological violence in doctors and nurses of particular hospital centers.
Therefore, the instruments used in Peru to assess psychological violence in all professional and occupational health groups at different levels of health care present limitations that do not allow reaching the standards of use of psychological tests (such as those of the American Educational Research Association, AERA; American Psychological Association, APAM; and the National Council on Measurement in Education, NCME) [26].
Due to the instrumental limitations described in the previous paragraphs, it is necessary to have an instrument that allows developing valid and reliable assessments on psychological violence and standardizing criteria for the application and interpretation of results. Our objective is to identify, evaluate and compare prevalences, verify corrective actions, and establish baselines in the field of mental health at work.
This study aims to determine the validity and reliability of the Peruvian version of the brief scale to evaluate psychological violence in health professionals (EVP-salud).
Methods
Study design
A cross-sectional psychometric evaluation design was applied to determine the validity and reliability properties of the brief scale to assess psychological violence in health professionals (EVP-salud). The study was conducted between January 2019 and February 2020. First, 30 healthcare workers participated voluntarily and anonymously to develop the semantic adaptation. In the second stage, 316 healthcare professionals and administrative workers from 17 healthcare centers in Peur were included; and the reliability test was developed according to internal consistency and the exploratory factor analysis. From this group, three subsamples were organized that included:
a) 27 participants for reliability analysis according to response stability.
b) 52 participants to evaluate convergent validity.
c) 42 participants to determine discriminative validity.
Participants
We included both health care professionals and administrative staff from different services of the country's health care centers that agreed to participate voluntarily and anonymously in the study. Following Nowrouzi and collaborators [27], the required work relationship length was two or more years, and the number of participants had to be proportional between males and females. Those returning from a period of leave or vacation during the last six months and those who did not complete or dropped out of the total number of psychometric tests requested were excluded.
As noted in the "study design" section, the first sample was organized for semantic adaptation. The psychological violence at work scale was applied to determine the reliability by internal consistency and exploratory factor analysis and to evaluate the complementary validity and reliability in the three samples.
To calculate sample size, we considered the criteria indicated by Lloret et al. [28]. We needed a minimum of 10 individuals for each of the 22 items of the ‘EVP-salud’ scale, so a minimum sample size of 220 participants was needed. Therefore, it was unnecessary to calculate the sample size since only health professionals eligible according to the criteria previously described were included.
Variables and data sources
The psychological violence at work generated by internal agents (which excludes physical violence) [1],[2],[3] – and subject to psychometric evaluation in this study – was determined through the ‘EVP-salud’ scale. The data collection procedure was carried out simultaneously in the 17 health centers previously mentioned, with the support of a person (for every health center) responsible for coordination and guidance. The scale was completed in an average of nine minutes. In addition to the socio-labor data indicated for the sample, information on job satisfaction and depression were recorded in the three subsamples and evaluated using three additional psychological tests, which are described below.
Instruments
Brief scale to evaluate psychological violence in health professionals
The ‘EVP-salud’ consists of 22 items that refer to three types of violence in the country's health centers:
a) Intimidation violence, composed by eight items (1, 2, 4, 8, 12, 15, 17, 21).
b) Isolation violence, composed of seven items (3, 5, 6, 7, 9, 10, 18).
c) Belittling violence, composed of seven items (11, 13, 14, 16, 19, 20, 22).
The overall reliability according to the internal consistency of the instrument was α 0.930 [25]. Seventy-seven percent (17/22) of the items were adapted from Díaz et al. study [25], and the rest were incorporated during the study. Each item corresponds to a four-point Likert-type scale, where one corresponds to "never" and four to "always" (in the last six months).
Overall job satisfaction scale
The Overall job satisfaction scale (OJS) consists of 15 items grouped into two subscales: intrinsic satisfaction (seven items) and extrinsic satisfaction (eight items). Each item corresponds to a seven-point Likert-type scale, where one corresponds to "very dissatisfied" and seven to "very satisfied". The scale's total score is the sum of the set of items, which ranges from 15 to 105 base points. However, it is advisable to use separately the subscales whose scores vary between 7 and 49 for intrinsic satisfaction and between 8 and 56 for extrinsic satisfaction. The scale presented good reliability and validity in 518 Spanish nurses [13]. In our study, we obtained α values of 0.75 for the total scale.
Beck depression inventory
The Beck depression inventory (Beck depression inventory, BDI-II) is widely used in psychological research. It consists of 21 items covering affective, cognitive, motivational, psychomotor, and vegetative components of depression. Each item consists of four statements, which are scored from zero to three. The BDI-II presented good internal consistency and validity in a sample of 797 Dominican participants [29]. In this study, the α coefficient was 0.91 for the global dimension.
Zung self-rating depression scale
The Zung self-rating depression scale (Zung SDS) comprises 20 items that involve affective, physiological, and psychological aspects of depression. Each item corresponds to a four-point Likert-type scale where one corresponds to "never" and four to "always" in the last week. Ten of these items are written using negative statements; therefore, as the score increases, mental health levels decrease. The scale has obtained good reliability and validity in a sample of 3614 people between 15 and 56 years of age [30]. In this study, the α coefficient was 0.93 for the total scale.
Statistical analysis
For the psychometric evaluation of the quantitative variables, exploratory factor analysis was developed using the Kaiser-Meyer-Olkin and Bartlett's sphericity tests. The principal components technique was then applied using a triple criterion:
a) Extraction of components with eigenvalues greater than unity, whose factor weights were equal to or greater than 0.5 for less than four components [31].
b) That the components appear in a factor whose total variance is greater than or equal to 50% and are contained in the correlation matrix of items analyzed [32].
c) Interpretation of the correlation matrix applying the orthogonal rotation method.
The information was processed using the InfoStat/E v.2017® software.
Ethics
Participants were informed of the research objectives, and their voluntary participation was recorded in a letter of consent, guaranteeing the anonymity and confidentiality of the data provided. The research was approved by the ethics committees of the Research Unit of the Universidad Nacional Agraria de la Selva and the Faculty of Medical Technology of the Universidad Nacional Federico Villareal.
Results
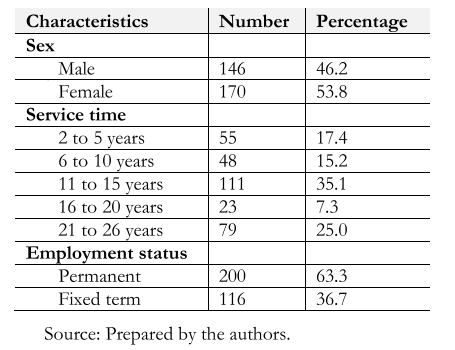
The initial sample was 367 workers, but 51 of them (16.1%) did not respond to the ‘EVP-salud’ items. Therefore, we had a final sample of 316 participants from different health centers in the country. Of these centers, 41.2% (7/17) are based outside of Lima. From the total number of participants, 63.6% (201/316) are healthcare professionals, of which 48.4% (122/122), 7.6% (19/122), and 23.7% (60/122) are nurses, physicians, and from other professions, respectively. The period of employment ranged from two to 26 years, with a predominance of 11 to 15 years (35.1%; 111/316 of the total). The percentages of participants from emergency services and outpatient and ambulatory clinics were similar (16.8% (53/316) versus 16.1% (51/316), respectively). The percentage of participants in the outpatient setting was 63.6% (201/316). The total number of male and female participants are not statistically different (X2 = 2139; p < 0.144) (Table 1).
In our study, the calculated sample size required a minimum of n = 220 subjects (22 items times 10), which was surpassed, and equivalent to a higher percentage variance of 43.6% (316/220 subjects). All healthcare and administrative personnel who agreed to participate voluntarily in the semantic validation, respond voluntarily and fill out both the psychological violence assessment scale and the other three psychological instruments applied in the discriminative and convergent validation were included (Figure 1).
 Full size
Full size 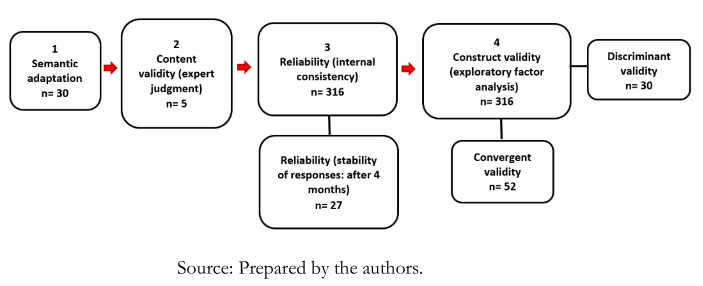 Full size
Full size Semantic adaptation
As a starting point for this evaluation stage, the theoretical foundation on the psychological violence at work domain was considered and organized into 22 indicators. These indicators are distributed in three theoretical factors, of which the intimidation is made up of eight items. The isolation and belittling factors have seven items each (Annex 1).
The semantic adaptation was conducted through two expert panel sessions, comprising 30 healthcare and administrative workers from the admission and emergency departments (first stage, Figure 1). We found the average comprehension difficulty index had 0.20 as the lowest value (for the first item, "18AI") and 0.80 as the highest one (for the last item, "10AI").
These results allowed us to fix the order of presentation of the items in the scale, to incorporate our modifications for 17 of the 22 items (excluding three items related to physical and external violence), and to reduce from five to four gradings, based on the proposal of a set of 22 Likert-type response items by Díaz and collaborators [25].
Content validity
In the second stage of psychometric evaluation (Figure 1), content validity was determined by the judgment of five experts (physicians, nurses, and educational psychologists), who independently rated each of the 22 items of the scale based on seven criteria. In this rating analysis, an item with a score of 1 to 4 was considered deficient, and a score of 9 to 10 was considered very good. According to the Kendall rank concordance coefficient assigned by the experts (W = 0.509; p < 0.026), the minimum conditions indicated by Aravena et al. [33] were exceeded. The best-rated criteria were related to the number and consistency of items per dimension and the feasibility of describing behaviors.
Reliability
The reliability of the ‘EVP-salud’ psychological violence scale was carried out in the third stage of the psychometric evaluation (Figure 1), applying the 22-item scale to 316 workers.
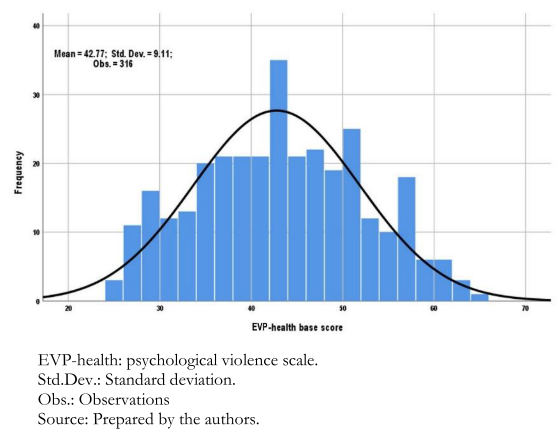
Previously, a symmetry analysis of the data distribution was performed. For this purpose, these base data were transformed into Fisher's standardized "Z" scores. The distribution was homogeneous, according to the Kolmogorov-Smirnov test (K-S= 0.46), with the p-value < 0.200 (Figure 2) exceeding the minimum p-value of p > 0.05. The total base score for the set of 22 ‘EVP-salud’ reagents ranged from 22 to 88 points. Likewise, this distribution homogeneity was corroborated by asymmetry statistics (As = 0.069), which indicates adequate data distribution by the standard error of the mean (EEm = 0.513), which shows good reliability of the ‘EVP-salud’, considering that the maximum limit is EEm = 2.00 for instruments with fewer than 24 items.
The reliability of the ‘EVP-salud’ psychological violence scale, according to internal consistency evaluated by Cronbach's α coefficient, was developed in two stages. The first had the 22-item scale from which the item "01I" was eliminated since it had a lower relationship with the scale and decreased the α value (Appendix 2). At the second stage, the 21-item scale had an α coefficient adequate globally (α = 0.803) and individually for each item (α = 0.800). This quantification is based on the covariance between the established items (Appendix 2), considering that the items are positively correlated with each other and that a Cronbach's α value between 0.70 and 0.80 is acceptable [34].
According to the response stability test, there were significant differences between the first and second application (after four months) of the psychological violence scale in 27 individuals (t = -2.855; p < 0.008), considering that a p < 0.05 is the minimum acceptable. For this purpose, the following selection criteria were used:
a) Voluntary but not anonymous participation.
b) Work experience of two or more years.
c) A work position, shift, and health center permanence (declared in the first application).
 Full size
Full size Construct validity
Construct validity was determined by exploratory factor analysis, based on information from 316 subjects and five methodological considerations [33],[34],[35]:
a) Theoretical basis organized into three factors or dimensions and 22 indicators [1],[2],[3],[12],[13],[25] (Annex 1).
b) Between five or ten individuals per item (in this case, it was 15 per item).
c) Preliminary reliability analysis to determine whether the correlations are low (≤ 0.70) or high (> 0.70) and to define the rotation method (orthogonal or oblique) and eliminate item(s) to increase the α value.
d) A minimum explained variance of 50%.
e) A minimum of three items per factor.
We performed the factor analysis using principal components with orthogonal rotation since the correlations between the 21 items were below or close to 0.700 (Annex 2). Then we eliminated items that were not grouped with factor loadings higher than 0.400, grouped in a theoretical factor different from the one proposed (Annex 2), or not grouped in a factor with at least three items.
In the final solution, the eigenvalues higher than 1.00 showed the existence of three factors.
This solution converged in seven iterations explaining 54.3% of the variance. This rate exceeds the minimum of 50% recommended by Lloret et al. [28] and others [35]. The items present factor loadings greater than 0.50 and communalities greater than 0.34. The varimax rotation has converged in 11 iterations, and the item with the lowest factor loadings (0.546) exceeds the 0.40 minimum recommended by Streiner et al. [32] and Lloret et al. [28].
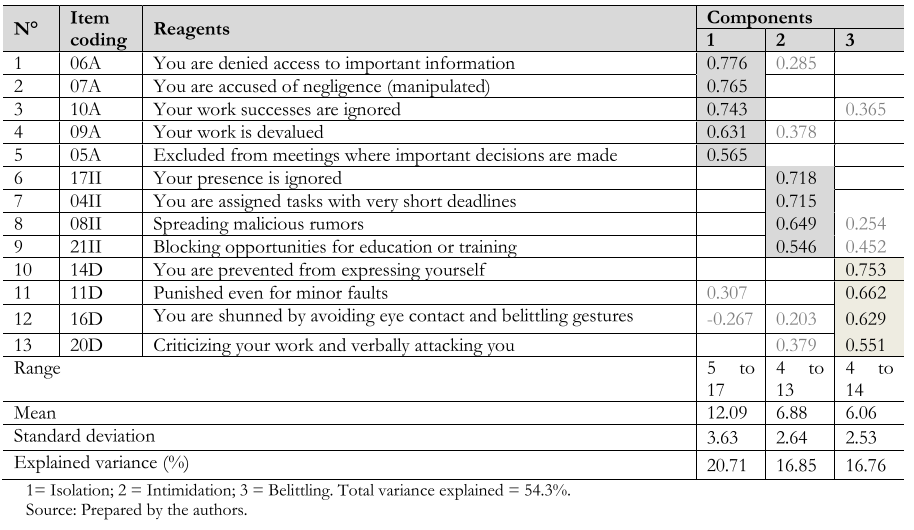
The final instrument consisted of 13 items presented in Table 2. Bartlett's sphericity test was significant (1078.56; gl = 78; p < 0.001), and the Kaiser-Meyer-Olkin sample size indicator was adequate (0.731), indicating that the construct validity summarized in the data matrix is adequate. The total α coefficient for the final version of the instrument was 0.759 and for the standardized items was 0.758.
 Full size
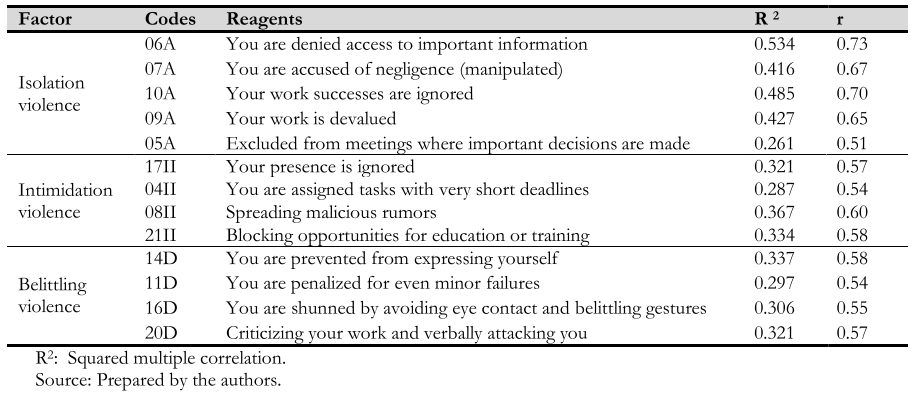
Full size Based on the final item composition and their respective factor loadings according to dimensions, adequacy cut points were defined as follows:
a) The isolation dimension was considered adequate with a factor loading between 0.565 and 0.776.
b) The intimidation dimension was considered adequate with factor loadings between 0.546 and 0.718.
c) The belittling dimension was considered adequate with factor loadings between 0.551 and 0.753 (Table 2).
On the other hand, the item of the first factor (F1) that is best associated with the overall score of psychological violence (square root result of R2), corresponding to the item "6A", describes isolation through attitudes that hinder access to basic information (r = 0.73) (Table 3). The isolation was present in 61.7% (195/316) of participants, compared to more than a quarter of those evaluated (26.3%: 83/316) who did not experience such violence.
Regarding the second factor (F2), the item "8II" has the highest correlation with the overall score and reflects the attitudes of colleagues for spreading malicious rumors (r = 0.60) (Table 3). This violence occurs in more than one-fifth (24.4%: 77/316) of those evaluated, and in opposition, it never happened for 69.3% (219/316) of respondents.
In the third factor (F3), the item "14D" has the highest correlation with the overall score and reflects the attitudes of colleagues who prevent the worker from expressing himself, interrupting continuously, or addressing only third parties (r = 0.58) (Table 3). In this indicator, 35.8% (113/316) of those evaluated experienced "always" or "almost always" this kind of violence, compared with 53.5% (169/316) who did not.
 Full size
Full size Finally, Pearson's correlation coefficients were calculated to determine whether factors or dimensions maintained a theoretical relationship. This coefficient indicated that the correlation is significant for p < 0.01 between the factor isolation and intimidation (r = 0.305), and with belittling (r = 0.186).
Convergent and discriminant validity
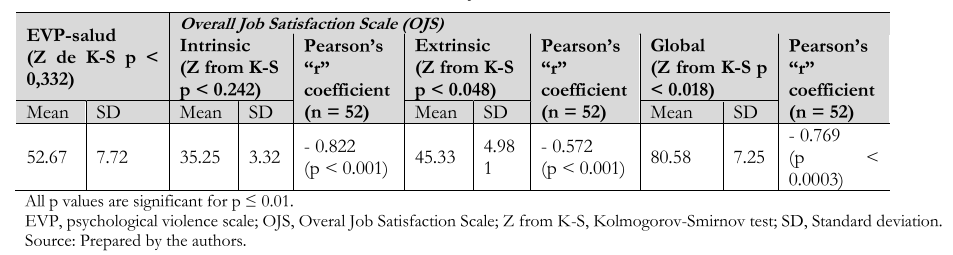
In the fourth stage of the psychometric evaluation (Figure 1), the OJS or general job satisfaction scale was used to evaluate convergent validity. This scale organizes job satisfaction constructs that reflect the work experience and collects emotional responses related to job content. The scale consists of two subscales:
a) Intrinsic factors (recognition, responsibility, promotion, and other factors related to the content of the task).
b) Extrinsic factors (related to satisfaction with the organization, schedules, remuneration and physical conditions of the job) [13].
The OJS scale was applied with the ‘EVP-salud’ to 52 workers in two health facilities (one in Lima and the other outside of the capital (n = 26 in each center). The results showed a high negative correlation. The convergence of scores between the ‘EVP-salud’ and the OJS scale was highly significant (r = -0.769; p < 0.0003). These data indicate that the higher the score on psychological violence at work, the lower the score on job satisfaction (Table 4).
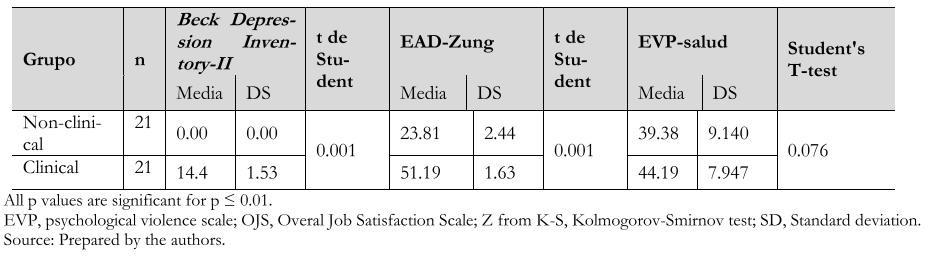
To further assess the discriminative validity (fourth stage, Figure 1), the ‘EVP-salud’ was administered to 42 individuals divided into two groups (non-clinical versus clinical) of the same sample size (n = 21). Participants in these two groups were previously diagnosed using two confirmatory instruments on depressive reactions (BDI-I and Zung's EAD).
 Full size
Full size The mean score of the non-clinical group was 39.38 ± 9.14 and that of the clinical group 44.19 ± 7.95, with 24 to 96 being the theoretical base score range. The results of the Student's t-test confirmed the absence of significant differences in the range of scores between the two samples (p < 0.076) (95% confidence interval: -10.15, 0.53), supporting the good discriminative ability of ‘EVP-salud’ in each of the comparison groups (Table 5).
 Full size
Full size Discussion
This study aimed to determine the validity and reliability of the Peruvian version of the brief scale to assess psychological violence in health professionals (Psychological Violence Scale, EVP-salud). We found that the solid psychometric properties within the scale are the following:
a) Good content validity.
b) Appropriate construct validity.
c) Adequate convergent and discriminant validity.
d) Significant reliability according to internal consistency.
Concerning the second property (appropriate construct validity, b), the first factor within internal psychological violence explains the most significant variance of psychological violence by few components (54.3% cumulative variance) and organizes the greatest number of items (38.5%; 5/13). This first factor describes the isolation and is complemented by intimidation and belittling.
In this work, we confirmed the existence of the principle of simple structuring of the ‘EVP-salud’. This principle is considered as an appropriate psychometric property by Lloret et al. [28], Coulacoglou & Saklafske [35], and by three institutions [26] when a set of items with the highest factorial weights are primarily organized in a main factor. In this case, it is within a total of three components.
Our analysis of the ‘EVP-salud’ instrument differs from the Chilean workplace violence and psychological harassment inventory [25]. This difference may be because the latter is based on four modalities of violence – including physical violence generated by external agents – and because it is validated for a broader context and work settings that are different from the health sector. The ‘EVP-salud’ presents three modalities of psychological violence (generated by internal agents) and excludes physical violence, as described by several scholars [1],[3]. Secondly, (in addition to the remaining eight indicators of the abbreviated scale not included in the final version) ‘EVP-salud’ highlights one indicator that describes belittling violence through nonverbal language (e.g., avoiding eye contact and gestures of ignoring the colleague's presence) and another indicator that highlights slander and public defamation. Thirdly, in our scale, there is an indicator of psychological violence, which underlies the restraint of the individual to express themself and blocking the work performance of a colleague. Finally, in the ‘EVP-salud’, the total variance explaining the overall psychological violence (cumulative variance: 63.8% versus 54.3%) is lower by up to 14.9% of the variance. Despite these differences, according to cluster analysis, the ‘EVP-salud’ scale converges with Diaz and collaborator's study [25] in the conformation of items by components of up to 55.6% (5 versus 9 items) in the first component and 57.1% (4 versus 7 items) in the second one.
Regarding the number of items of the final version of the brief psychological violence scale (‘EVP-salud’ of 13 items), it also exceeds up to 46.2% (13/7) of the scale of aggressive behavior of health workers by Waschgler and collaborators [20], used in the mental health field where psychological violence is organized by seven items [13],[20]. It also exceeds up to 61.5% (13/5) of items to the structured survey questionnaire of Perez [11], where the latter is composed of five items and used for studies on psychological violence in health professionals in several Latin American countries [10].
Regarding the complementary reliability of the fourth psychometric property (d) of the ‘EVP-salud’ scale, according to the response stability test, we also found that there are differences between the first and second application of the instrument, confirming the report of Díaz et al. [25] where psychological violence at work fluctuates over time.
The internal consistency properties are consistent with Cascaes da Silva et al.'s specifications [34] and have adequate validity. This possible uniformity contrasts with previous studies in our country, which used different techniques and instruments to assess violence focused on specific healthcare establishments and professional groups [15],[16],[17],[18],[19]. In our study, the sample size indicated above was higher than the minimum required of 10 individuals for each item (n = 316 versus n = 220 subjects) [33] and higher than the sample size of studies in Bolivia, Colombia, Ecuador, and Mexico [21],[22],[24].
On the other hand, – just as there is an association between the different modalities of psychological violence and harassment, and other psychosocial variables in the Latin American context (e.g., job satisfaction) [10] – we also verified the negative association between psychological violence and job satisfaction using the ‘EVP-salud’. These results agree with Llor et al. [13] and are highly significant since intrinsic job satisfaction is linked to the presence or absence of psychosocial risk factors in the healthcare facility [4]. Furthermore, the negative consequences of decreased job satisfaction are known to negatively influence organizational commitment [3] and increase stress and burnout levels in healthcare workers [9].
Limitations
The study was conducted with a sample 43.6% (316/220) larger than the minimum required size, according to the number of items in the instrument [28], which is equivalent to 220 subjects (10 x 22 items). Possible limitations of our study are linked to the limited quality control over the pollsters and the small sample size used to assess the complementary validity and reliability associated with job satisfaction and depression. However, as the gender distribution is similar between groups and the length of job services is two to more years [27], the validity and reliability determined in this study are maintained. Moreover, the occurrence of psychological violence at work does not differ between healthcare groups [5],[6],[7].
Thus, the prospects for using the Peruvian version of the abbreviated psychological violence scale ‘EVP-salud’ are:
a) To ensure a valid and reliable assessment of psychological violence in healthcare workers.
b) Since violence generally remain hidden for various reasons (including the need for anonymity on the part of the complainant), the anonymous and voluntary nature of the scale could help capture violence reports [1],[8].
c) Identify intervention topics, together with other instruments, for the evaluation of human behavior in organizations.
Finally, given the prevalence and impact of psychological violence and its corresponding responses in healthcare centers, the use of the ‘EVP-salud’ may promote forming a baseline and monitoring responses based on the framework of organizational psychology [1].
Conclusion
This paper has determined that the Peruvian version of the brief scale to assess psychological violence in health professionals (EVP-salud) has shown good reliability and validity indexes that could be applied to different health centers in the country (Annex 3).
Notes
Contributor roles
LFAT, YJGH: conceptualization, methodology, formal analysis, research, data curation, writing the original draft; preparation, review, editing, and supervision. CKGD, GECG: conceptualization, methodology, research, resources, writing the original draft; preparation, review and editing; supervision, project management, and fund acquisition.
Competing interests
The authors completed the ICMJE conflict of interest statement and declared that they received no funding for the completion of this article; have no financial relationships with organizations that may have an interest in the published article in the past three years; and have no other relationships or activities that may influence the publication of the article. Forms can be requested by contacting the responsible author or the Editorial Committee of the Journal.
Funding
The authors declare no external sources of funding.
Ethics
The study had the approval of the Research Ethics Committees of the Universidad Nacional Agraria de la Selva, and of the Facultad de Tecnología Médica of the Universidad Nacional Federico Villareal.
Data sharing statement
The data used for the study are available upon request to the corresponding author.
Language of submission
Spanish.
Acknowledgments
To Karina V. Diestro C. (Escuela Académica de Psicología, Universidad de Huánuco), and psychologist A. Celia Lino C. (Hospital de Tingo María), for their collaboration in data collection.
Annex 1
