Research papers
← vista completaPublished on March 24, 2022 | http://doi.org/10.5867/medwave.2022.02.002513
Perception of risk to COVID-19 and mental health indicators in workers of a Peruvian hospital: An analytical cross-sectional study
Percepción de riesgo a COVID-19 e indicadores de salud mental en trabajadores de un hospital peruano: estudio transversal analítico
Abstract
Introduction COVID-19 has caused great fear on health professionals and could affect their mental health, therefore it is important to determine the association between the perception of risk to COVID-19 and mental health in workers of a Peruvian hospital.
Methods Analytical cross-sectional study, through virtual survey. The dependent variables were: depression, anxiety and stress; The independent variable was perception of risk to COVID-19 and the covariates: sociodemographic, family, work and clinical data. Crude and adjusted prevalence ratios were found with a 95% confidence interval and a significance level of 5%.
Results There was no association between risk perception and depression (adjusted prevalence ratio: 0.98 95% confidence interval: 0.89 to 1.08), anxiety (adjusted prevalence ratio: 0.94 95% confidence interval: 0.89 to 1.00), stress (adjusted prevalence ratio: 0.89 95% confidence interval 0.76 to 1.04). In the multivariate analysis, an association was found between depression with direct contact with the COVID-19 patient (adjusted prevalence ratio: 2.06, 95% confidence interval: 1.14 to 3.70) and with having a comorbidity (adjusted prevalence ratio: 2.56 95% confidence interval: 1.52 to 4.30); likewise, between anxiety with number of children (adjusted prevalence ratio: 1.09 95% confidence interval: 1.00 to 1.18), with direct contact with COVID-19 patient (adjusted prevalence ratio: 2.67 95% confidence interval 1.46 to 4.85) and having comorbidity (adjusted prevalence ratio: 2.00 95% confidence interval: 1.40 to 2.86); finally, between stress with direct contact with the COVID-19 patient (adjusted prevalence ratio: 2.86, 95% confidence interval: 1.20 to 6.83).
Conclusions No statistically significant association was found between risk perception and depression, anxiety, or stress. However, there was an association between depression, anxiety, and stress, each with direct contact with COVID-19 patients; between anxiety and depression, each with having comorbidities and, finally, anxiety with the number of children.
|
Key messages
|
Introduction
In March 2020, the World Health Organization (WHO) declared the COVID-19 pandemic [1]. By the end of June 2020, 2 033 606 people were infected, and 190 906 died in Peru [2], causing a significant social impact and a health care collapse. As new COVID-19 waves appeared, infection rates increased again in many world regions, including Latin America, with Peru being one of the most affected countries worldwide [3].
Hospital personnel has a higher risk of infection due to con stant contact with COVID-19 patients, and their protection is fundamental since infection in health care workers decreases the response capacity. This risk is particularly elevated in Peru, where appropriate personal protection elements are scarce [4]. A study in the United States found that most personal protec tive equipment availability is below 50% [5], and a study of 521 health professionals in Colombia revealed that 47.9% had not received training on personal protective equipment during the pandemic [6]. Moreover, a study of 5210 Paraguayan residents found a greater perception of risk of infection when they had a family member or friend suspected or exposed to COVID-19 [7].
Health personnel finds themselves in an unprecedented sani tary situation. Amidst the uncertainty, health personnel work under extreme pressure, are subject to a high risk of COVID-19 infection due to inadequate protection and must deliberate tough decisions such as allocating limited resources to equally needy patients.
All these circumstances can cause mental health problems in these workers. These problems include stress, depression, or anxiety [8],[9]. Despite the great vulnerability of health person nel, mental health status has not been explored in the Peruvian context. Therefore, this study explores the association between the perception of risk to COVID-19 and indicators of depres sion, anxiety, and stress among workers of a Peruvian hospital.
Methods
Study design and setting
A cross-sectional, analytical study was conducted on the work ers of the Chancay Hospital, located in Lima. A survey was conducted between July and August 2020 to 588 health care workers.
Population and sample
The population consisted of health care workers of the referred hospital during the study period. The sample size was based on the prevalence of stress, anxiety, and depression among the dif ferent categories of risk perception to the COVID-19 virus or the pandemic in general [10],[11],[12]. These three estimates were found using the EPIDAT 4.2 program, considering a power of 80% and a confidence level of 95%, and we chose the one that gave us the highest prevalence [12]. We expected to find a prev alence ratio of anxiety/depression in health care workers of 1.6 according to the fear of feeling unprotected against COVID-19. Given these factors, a minimum sample size of 228 health care workers was considered.
All workers who answered the questionnaire and gave informed consent were included. Workers who suffered from depression or any psychiatric pathology before or during the study period, those who did not fill out the data collection instrument cor rectly, and those who had difficulty reading the survey were excluded.
Although the planned sample was 228, we reached a sample of 191 participants. According to previous studies, this sample size had a statistical power of 98%, 99%, and 73% of finding the association between perception of risk to COVID-19 with stress, anxiety, and anxiety/depression, respectively.
Variables and instruments
The survey included sociodemographic, health status, work and family situation, and contact with COVID-19 patients’ data. Likewise, for the perception of risk to COVID-19, a previously validated scale named 'Perception of safety regarding COVID-19 protection measures in Peruvian resident physi cians' [13] was used. This scale was validated through the judg ment of 12 experts, who analyzed the items' relevance, representativeness, and clarity. Regarding reliability, the scale has a Cronbach’s α of 0.8. Four Likert-scaled questions with five response categories measure perceptions about safety mea sures and contagion risk. Moreover, this scale evaluates individual and environmental aspects, including colleagues and working conditions.
The Depression, Anxiety, and Stress Scale (DASS-21) [14] addressed participants' mental health. The depression subscale assesses dysphoria, hopelessness, sadness, and anhedonia. The anxiety subscale evaluates aspects related to psychophysiologi cal activation or autonomic arousal (hand sweating, trembling, among others) and subjective experiences of anxiety. Furthermore, the stress subscale evaluates the difficulty in relaxing, nervous arousal, agitation, irritability, and impatience.
The instrument used is a package of three four-point severity/ frequency Likert scales (seven items each) to measure how much the statement applied over the past week. The rating scale is as follows:
0: 'Did not apply to me at all'.
1: 'Applied to me to some degree, or some of the time'.
2: 'Applied to me to a considerable degree, or a good part of the time'.
3: 'Applied to me very much, or most of the time'.
Then we sum up what is obtained from subscales items to assess the presence and degree of depression, anxiety, and stress:
Depression:
Mild: 5 to 6.
Moderate: 7 to 10.
Severe: 11 to 13.
Extremely severe: 14 or more.
Anxiety:
Mild: 4.
Moderate: 5 to 7.
Severe: 8 to 9.
Extremely severe: 10 or more.
Stress:
Mild: 8 to 9.
Moderate: 10 to 12.
Severe: 13 to 16.
Extremely severe: 17 or more [15].
The depression, anxiety, and stress subscales presented an α of 0.85, 0.73, and 0.83, respectively. Overall, the DASS-21 presented an α of 0.91 [15].
Procedures
The institution requested the required premises, and the data were collected only after approval by an ethics committee through a virtual survey sent via e-mail to the workers from a list provided and authorized by the hospital. The survey was applied according to the selection criteria and was filled out anonymously by the participants.
Once data collection was completed, an educational interven tion was conducted through an informative video on mental health and specific strategies for coping with the current pandemic.
Statistical analysis
The Stata v14 program was used for the analysis. Categorical variables were expressed as absolute and relative frequencies (percentages), and numerical variables were expressed as mea sures of central tendency and dispersion, according to their dis tribution. When the distribution was non-normal, median and interquartile ranges were used. If the distribution was normal, mean and standard deviation were used. Eight participants did not answer the question regarding emergency rotations. The analysis of living with a partner and children variable was per formed only on those who referred having a partner or chil dren, respectively.
Poisson regression with robust variances was used for the infer ential analysis to find crude and adjusted prevalence ratios with their respective 95% confidence intervals. The main indepen dent variable – i.e., the perception of risk to COVID-19 – and the other independent variables that had a significant associa tion in the bivariate analysis entered the multivariate model. A p< 0.05 was considered statistically significant for all cases.
Ethics
All the information was used exclusively for scientific purposes and was handled anonymously (the authors did not have access to the workers' identities). The research project was approved by the ethics committee of the Universidad Ricardo Palma with the official letter-number PG-022-2020, following the Declaration of Helsinki principles. The study’s objectives were explained to the occupational health area of the hospital where the research was conducted. Before each electronic survey, an informed consent form was demanded, explaining the scientific purpose of the research, the scope, and expected results. In this instance, the importance of identifying the perception of expo sure to COVID-19 risk, assessing mental health, and recogniz ing the benefits obtained from participating in this study was also explained. It was also identified as a benefit to provide bet ter attention to health workers for timely diagnosis and treatment.
Once the survey ended, an informative intervention was con ducted using virtual resources to promote good mental health, prepared specifically for this population. The information was based on two basic psychosocial skills guides for front-line staff of COVID-19 response prepared by the WHO: the 'Addressing the mental health and psychosocial aspects of the outbreak of COVID-19' guideline [16] and the 'mhGAP intervention guide for mental, neurological and substance use disorders in non specialized health settings: mental health Gap Action Programme (mhGAP)' [17]. The audiovisual material was reviewed by hospital leadership, which gave its approval and facilitated its broadcast to all hospital staff.
Results
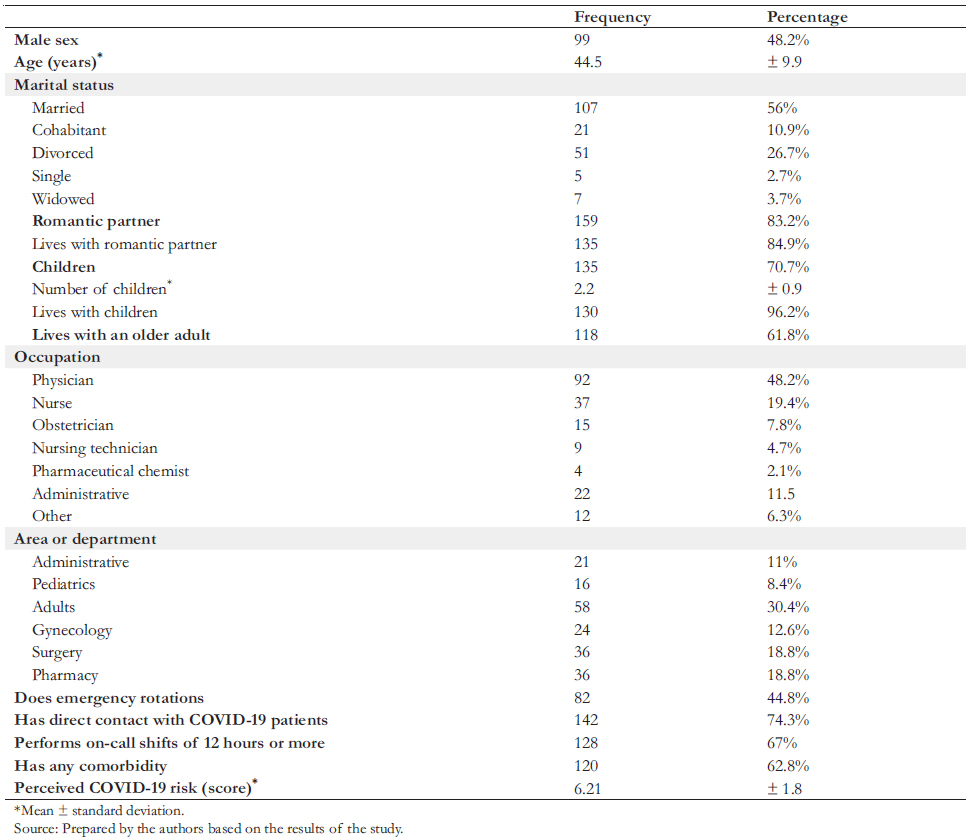
Of the 191 health care workers evaluated, 48.2% were male, and the mean age was 44.5 years. The majority were physicians (48.2%), followed by nurses (19.4%) and obstetrics profession als (7.8%). Regarding work, 44.8% had emergency rotations, and 74.3% had direct contact with COVID-19 patients (Table 1). We also found that 46.6% were suffering from depression, 60.7% from anxiety, and 27.8% from stress, at dif ferent levels (Table 2).
 Full size
Full size 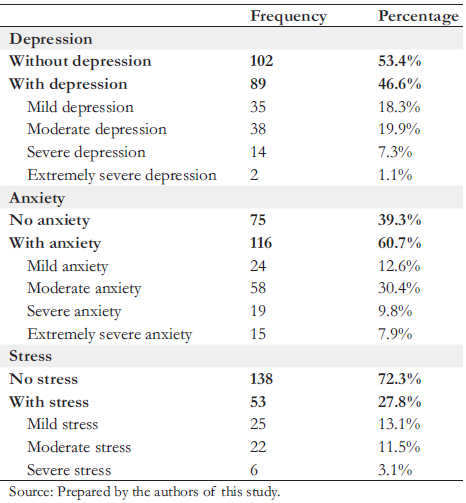 Full size
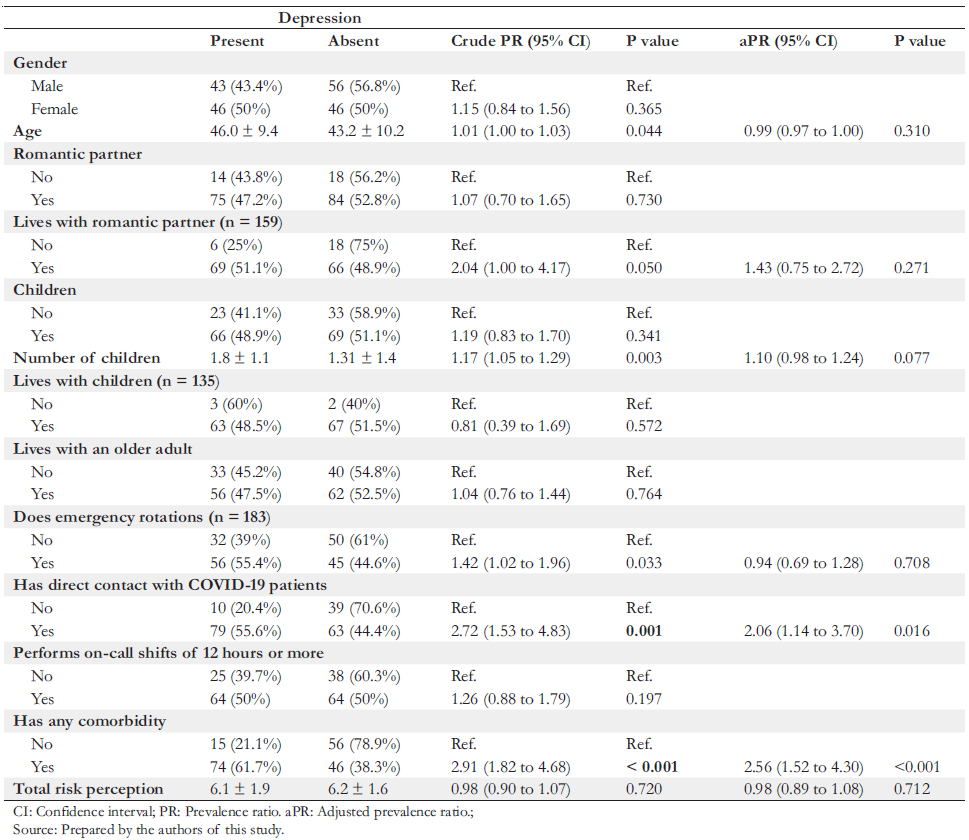
Full size Concerning depression, no association was found with the per ception of risk to COVID-19. However, in the multivariate analysis, an association was found between depression and direct contact with COVID-19 patients (crude prevalence ratio:
2.72 and 95% confidence interval: 1.53 to 4.83; adjusted prevalence ratio: 2.06 and 95% confidence interval: 1.14 to 3.70), as well as the presence of any comorbidity (crude preva lence ratio: 0.98 and 95% confidence interval: 0.90 to 1.07; adjusted prevalence ratio: 0.98 and 95% confidence interval:
0.89 to 1.08) (Table 3).
Concerning anxiety, no association was found with the percep tion of risk to COVID-19. However, in the multivariate analy sis, an association was found between anxiety and the number of children (crude prevalence ratio: 1.13 and 95% confidence interval: 1.05 to 1.22; adjusted prevalence ratio: 1.09 and 95% confidence interval: 1.00 to 1.18), as well as direct contact with COVID-19 patients (crude prevalence ratio: 2.99 and 95% con fidence interval: 1.80 to 4.94; adjusted prevalence ratio: 2.67 and 95% confidence interval: 1.46 to 4.85), and having any comorbidity (crude prevalence ratio: 2.04 and 95% confidence interval: 1.48 to 2.83; adjusted prevalence ratio: 2.00 and 95%
confidence interval: 1.40 to 2.86) (Table 4).
Ultimately, the stress showed no association with the percep tion of risk of COVID-19. However, in the multivariate analy sis, an association was found with having direct contact with a COVID-19 patient (prevalence ratio: 3.31 and 95% confidence interval: 1.39 to 7.86; adjusted prevalence ratio: 2.86 and 95%
confidence interval: 1.20 to 6.83) (Table 5).
 Full size
Full size 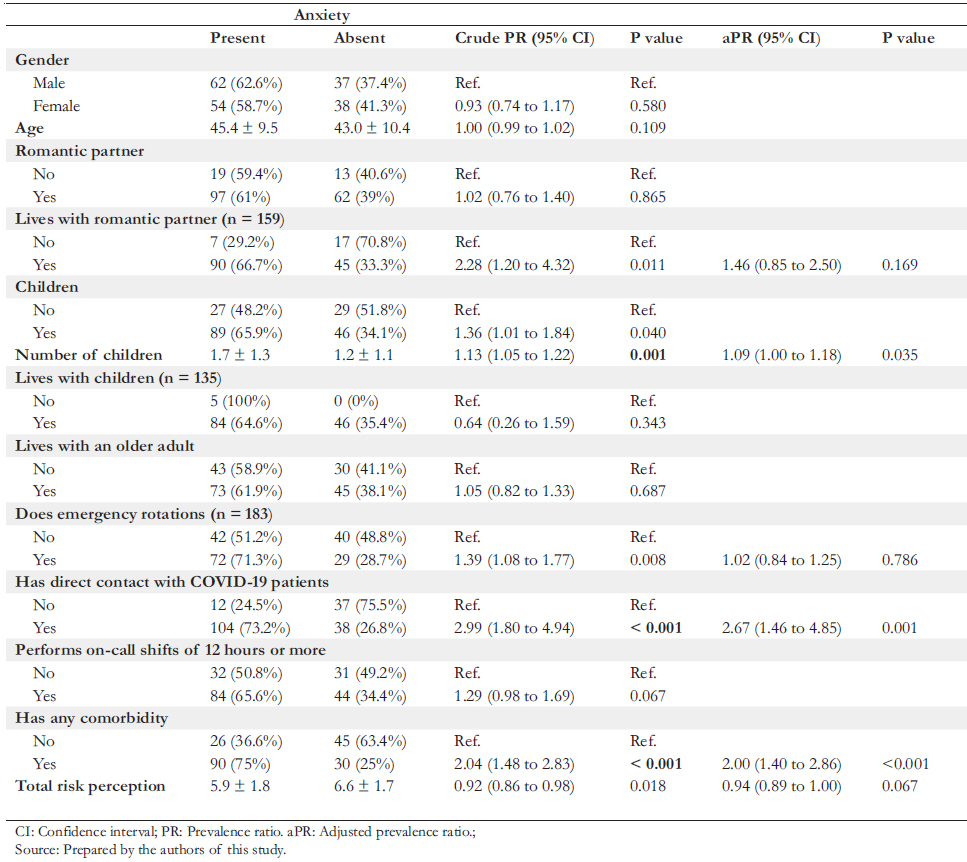 Full size
Full size 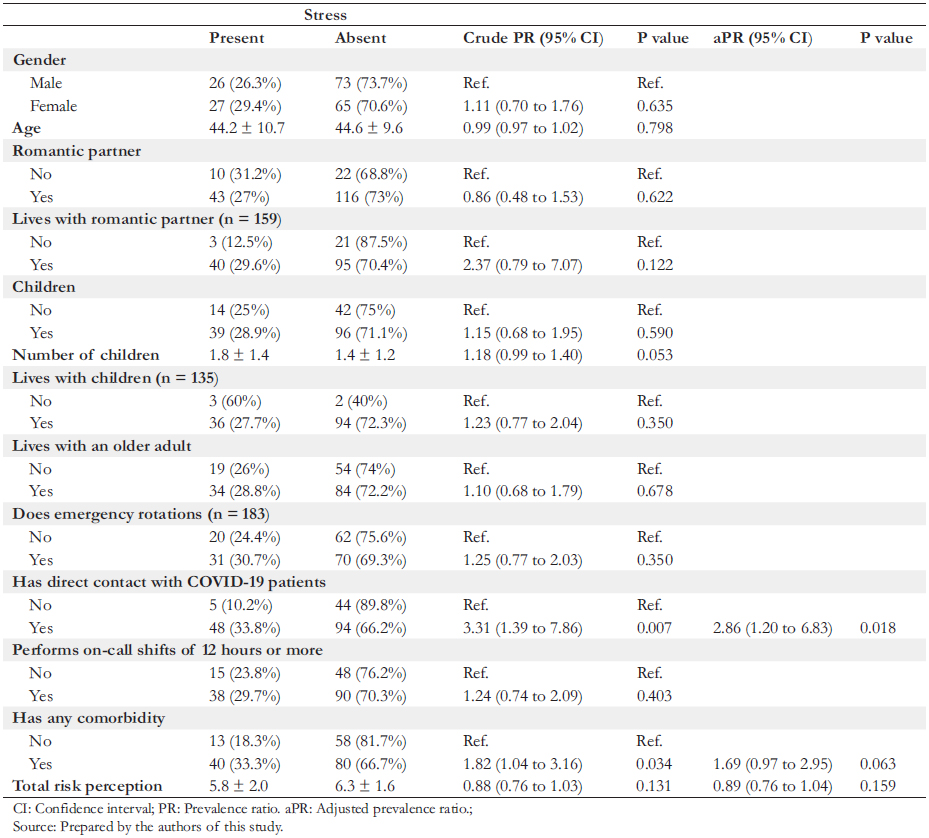 Full size
Full size Discussion
The COVID-19 pandemic has committed health care person nel to an unprecedented sanitary confrontation that involves a high emotional impact due to frustrations, helplessness, adapta tion problems, and fear of discrimination [9],[18]. The present study reports a high percentage of anxiety, depression, stress, and associated factors. Therefore, the evidence of these symp toms suggests that, in addition to confronting COVID-19 daily, health care workers must strive to maintain adequate mental health. As this study included workers of a level two hospital that cares for COVID-19 patients, the results could be extrapo lated to other hospitals with similar characteristics in Peru – considering the non-probabilistic nature of this sampling.
We found no association between mental health and COVID-19 risk perception in health care workers. This finding differs from studies among university students, where the perception of risk and impact of COVID-19 was significantly associated with anxiety [10]. This disparity may lie in the knowledge that health care personnel have over personal protective protocols and equipment that confers a greater sense of security, as noted by Kasun et al. [19], and supported by a study conducted on nurses in the United States [20]. The question that revealed the highest risk perception was related to the perceived risk of working in the hospital ("I consider that I am exposed to a higher risk of contagion in my workplace due to my working conditions"). However, the perception of risk increases when the worker is in direct contact with COVID-19 patients. This variable was sig nificantly associated with various mental health indicators.
The present study found an association between anxiety and direct contact with COVID-19 patients. This finding aligns with Jiambo et al. [9], who found that nurses treating COVID-19 patients presented more severe anxiety symptoms. This anxiety could be aggravated by working longer hours than usual and exposure to patients at potential risk of contagion. Likewise, Zhang et al. [21] mentioned that contact with COVID-19 patients was a risk factor for anxiety among physicians. This factor may be particularly relevant in rural areas where working conditions are precarious and personal protective equipment is scarce. This association could be explained by the fear of infecting family members that long working shifts generate, in addition to the incapacity when facing critical patients. In these cases, it is recommended to promote psychotherapeutic inter ventions through a mental health team, including relaxation techniques, social network support, providing a space for rest, and access of health personnel to a comprehensive psycholog ical consultation to manage anxiety.
This study also found an association between having any comorbidity with depression and anxiety. This finding is in line with Sayedd et al. [19], who found in the general population in Bangladesh that the prevalence of anxiety, depression, and stress symptoms was higher in those who had pre-existing comorbidities. This linkage could also be true in health care workers due to their heightened awareness of their vulnerability to COVID-19. It is recommended that mental health resources be made available for health personnel – especially those with a chronic illness – as the perceived risk of contagion impacts mental health.
A significant association was observed between the number of children and anxiety. A similar finding was seen in Poland’s gen eral population [22], where having children was associated with anxiety during the COVID-19 pandemic. Likewise, another study found family size as an important factor linked to anxiety during the COVID-19 pandemic [23]. This phenomenon is probably due to increased concern about family members becoming ill and increased financial responsibility for those health care workers who are the main family providers.
Another finding is the relationship between depression and direct contact with COVID-19 patients. This aligns with Di Tella et al. [24], who identified that front-line health profession als working in COVID-19 wards had higher levels of depression probably because they were involved in the morbidity and mortality process, which in turn carries a high emotional bur den. The exposure to a higher risk of contagion, little rest time, shortage of personal protective equipment, among other aspects, can greatly affect staff. Likewise, Xu et al. [25] reported that during the first wave of the pandemic, surgical medical personnel manifested symptoms of depression, probably due to the perceived risk of self-infection. This exacerbation of symptoms among surgeons could be explained by the uncer tainty about the contagious potential of operated patients since it was challenging to determine previous exposure to COVID-19. This situation is also aggravated among physicians treating patients needing emergency surgical treatment, intuba tions, or other interventions that require close contact.
In contrast, Chen et al. [26] found no association between working on the front-line or working hours per week with depressive symptoms. However, they did observe a link with the workload. These findings could be explained by the double edged sword of the chronic stress and depressive symptoms related to the risk of infection that follows working close to COVID-19 patients and the development of psychological dis tress after keeping affected patients alive. This is especially important with a lack of resources for proper care and is aggra vated even more when working shifts are long. In view of this problem, it is recommended to hire more health personnel to ensure that each worker has adequate hours of rest, administer appropriate personal protective equipment, and ensure psycho logical interventions to timely diagnose and treat symptoms suggestive of depression or other mental health problems.
An association was observed between direct contact with COVID-19 patients and stress. This finding is in line with Boon et al. [27] and Wenshi et al. [28], where it was reported that front-line workers had higher stress levels. This may be due to autonomous system activation by being in the front-line and having a high workload during the pandemic. It is recom mended that institutions take this into account to alleviate the burden by giving better work schedules and allowing social and family support to health care workers. To this end, the collabo ration of society is also necessary.
The present study was limited by using a validated screening survey, which helps detect symptoms, but not for the medical diagnosis of depression, anxiety, and stress. Also, given the lack of knowledge about respondents' anxiety, depression, and stress levels before the outbreak, it is difficult to establish whether these findings can be attributed to work circumstances during the pandemic. On the other hand, the instrument that assessed risk perception to COVID-19 has few items and there fore may not adequately measure risk perception. However, this survey has been previously validated, and there are no other instruments available, so this was the best option available. In addition, the data come from a cross-sectional survey, so causal inferences cannot be made. Furthermore, the data were col lected through a self-report questionnaire, which has a risk of response bias because patients may not answer truthfully. In order to reduce this bias, it was decided that the data collection would be anonymous so that there would be no fear of giving truthful answers for fear of the opinion of superiors or researchers. Also, selection bias was possible given that survey respondents may have lower stress levels and less workload (which could be associated with some independent variables). To reduce selection bias, the survey invitation was repeated at least twice so that those who did not respond in the first e-mail ing could do so in a subsequent invitation. Finally, the initially planned sample size was not reached, which meant a slight decrease in the statistical power to find an association with anx iety/depression. Despite this, we still consider the results valid as the probability of a type two error remains relatively low.
Conclusions
We found no significant association between the perception of risk to COVID-19 and mental health indicators among health care workers. However, there was an association between direct contact with COVID-19 patients and symptoms of depression, anxiety, and stress, and between anxiety symptoms and the number of children and having any comorbidity.
We suggest providing support to improve workers' well-being through consequent reduction of symptoms of mental health affectation among front-line personnel.
Notes
Contributor roles
DMQL: conceptualization, methodology, software, validation, formal analysis, resourcing, writing (original draft preparation), drafting (review and editing), visualization, oversight, project management, and fund acquisition. HGV: conceptualization, validation, research, resources, data curation, writing (original draft preparation, review, and editing), visualization, oversight, project management, and fund acquisition. CBL: validation, resourcing, data curation, writing (original draft preparation, review, and editing), visualization, oversight, project management, and fund acquisition. JCV: methodology, validation, resourcing, writing (review and editing), visualization, oversight, project management, and fund acquisition.
Competing interests
The authors completed the ICMJE conflict of interest statement and declared that they received no funding for the completion of this article; have no financial relationships with organizations that may have an interest in the published article in the past three years; and have no other relationships or activities that may influence the publication of the article. Forms can be requested by contacting the responsible author or the Editorial Board of the Journal.
Funding
The study was self-financed by the authors. The Universidad Ricardo Palma financed the publication costs of this study.
Ethics
The ethics committee project of the Universidad Ricardo Palma approved the research with the official letter-number PG-022-2020. The study was also registered in the national health research registry PRISA with code EI00001396.
Data sharing statement
Supplementary material available at: https://figshare.com/s/c9b365d76d42efdb2bfb
Language of submission
Spanish.
