Research papers
← vista completaPublished on May 27, 2022 | http://doi.org/10.5867/medwave.2022.04.002551
Functional Classification Spaces according to walking speed in self-sufficient Chilean older adults: A complement to the Periodic Physical Examination
Espacios de Clasificación Funcional según velocidad de marcha aplicada a adultos mayores autovalentes chilenos: Un complemento al Examen de Medicina Preventiva
Abstract
Introduction Walking speed is related to functionality in daily activities. Preventive Medicine Examination of the Chilean older adults is a vital prevention program for Chilean community- dwelling older adults. However, this evaluation does not include speed in its battery of tests.
Objective To evaluate the functional classification spaces for threshold, reference, and categorization val-ues of self- selected and maximum walking speed applied to self- sufficient older adults.
Methods Seventy- two self- sufficient older adults participated in this observational, exploratory, and cross- sectional study. Each participant was asked to walk naturally and then at full speed for three minutes. Through a dispersion graph between self- selected walking speed (axis "x") and maximum walking speed (axis "y"), functional classification spaces were constructed according to documented values for i) thresholds of basic functionality, ii) referential for the instrumental spectrum and iii) functional categorization for "household walker" (< 0.4 meters per second, m/s), "limited community ambulator" (0.40 to 0.80 m/s), "community ambulator" (0.81 to 1.3 m/s), and "cross street safely" (> 1.3 m/s). The relative frequency (%) of older adults who meet each established quadrant was determined.
Results The threshold was reached by 100% of the participants (basic daily activities). About 80% of the older adults have a functional classification space below the reference limit (instrumental and advanced daily activities). It was also found that 81% of women and 69% of men are "efficient in the community", and 31% of men and 14% of women reach the minimum value for "effec-tive street crossing" (advanced daily activities).
Conclusions The exploration of functional classification spaces according to self- selected walking speed and maximum walking speed applied to a group of self- sufficient older adults reveals that this pop-ulation is at risk of deteriorating instrumental and advanced activities of daily living.
|
Main messages
|
Introduction
The increase in life expectancy is an evident fact worldwide. In Europe, North America, and Oceania, life expectancy is around 80 years, while in Latin America and the Caribbean, it is close to 75 years. The projections for the population aged 65 years or over indicate that by 2025 most South American countries will surpass 10%, and even in Uruguay and Chile, it will exceed 15% [1]. These demographic changes should be followed by policies and mechanisms attentive to improving the quality of life of older adults in the region [2].
Aging is complex and multifactorial, involving progressive and irreversible changes [3]. This physiological process decreases functional capacity, resulting in physical, social, and psychological frailty [4], dependency, and death [3],[4]. Frailty resides in the dynamic interaction of sarcopenia and low activity, leading to a progressive decrease in maximum oxygen consumption, total energy expenditure, basal metabolic rate, muscle strength, power, and gait parameters' alteration [5]. Many instruments have been proposed to measure functionality in older adults – especially in basic dependency [6] – and classify levels of independence and autonomy [7],[8]. However, diagnostic approaches are generic, raising doubts about the presence of heterogeneous movement profiles and functionality within a stratified group.
Bipedal locomotion is fundamental for efficiently developing basic, instrumental, and advanced daily activities [6],[8]. Speed is its primary indicator due to its reliability, validity, and sensitivity to evaluating and monitoring functionality in various populations [9],[10],[11],[12]. These characteristics establish speed as the "sixth vital sign" in older adults to predict functionality [12] and detect systemic risks while assessing cardiopulmonary [13], neuromotor [14], cognitive [9], and nutritional [15] areas. Population reference values according to sex and age [16] and thresholds required for minimum functionality have been reported [11],[12],[17],[18].
The World Health Organization defines health in older adults not in terms of its deficit but as preservation of functional capacity [2]. In Chile, the periodic functional assessment of older adults (Evaluación Funcional del Adulto Mayor; EFAM) is a predictive instrument of functionality loss designed to timely detect risk factors in community- dwelling older adults [19]. Its application in Chilean Primary Health Care has allowed older adults to be classified as: i) self- sufficient without risk in 70%, ii) self- sufficient with risk in 17%, and iii) dependent with risk in 13% [20]. In this regard, it is inferred that one- third of older adults are at least in a pre- frailty state. Hence, these statistics generate concerns about whether all self- supporting older adults have a safe and efficient gait, directly impacting the risk of trips, falls [21], and advanced activities in the community [8],[12].
The Preventive Medical Examination of Older Adults (Examen de Medicina Preventiva del adulto mayor; EMPAM) (7) includes peri-odic functional and emotional assessments, abuse screening, and risk of falls evaluation. Regarding the risk of falls, it is essential to assess mobility and balance through reproducible tests such as the unipodal station and the timed up and go test [22]. However, these tests have narrow margins of normality, making it challenging to discriminate between measurements [23]. Moreover, they do not incorporate an added value to speed to predict health and functionality states [24]. Speed is the indicator that best represents the global motor ability of fragile older adults [10]. Analyzing self- selected walking speed and maximal walking speed is helpful due to its measurement properties [25], its predictive value [26], and the possibility of establishing functional reserve indicators [27],[28].
Concerning the periodic functional assessment of older adults, it is hypothesized that not all older adults classified as "self- sufficient" have the minimum walking speed needed to be fully functional in daily activities. Thus, it is interesting to know the percentage distribution within functional classification spaces. This research aims to evaluate in self- sufficient Chilean older adults a functional classification spaces proposal, added to peri-odic physical examinations, according to threshold [17],[18], referential [16], and functional categorization [12] indicators of self- selected walking speed and maximal walking speed.
Methods
Participants
Seventy- two self- sufficient older adults (age: 70 ± 5.1 years; periodic functional assessment of older adults- A: 51 ± 3 points) participated in this observational, exploratory, and cross- sectional study, selected by a non- probabilistic convenience sampling. The older adults came from four clubs in Talca, Chile. Recruitment took place in January 2015 through the presentation of the project and an interview between the researcher and interested participants.
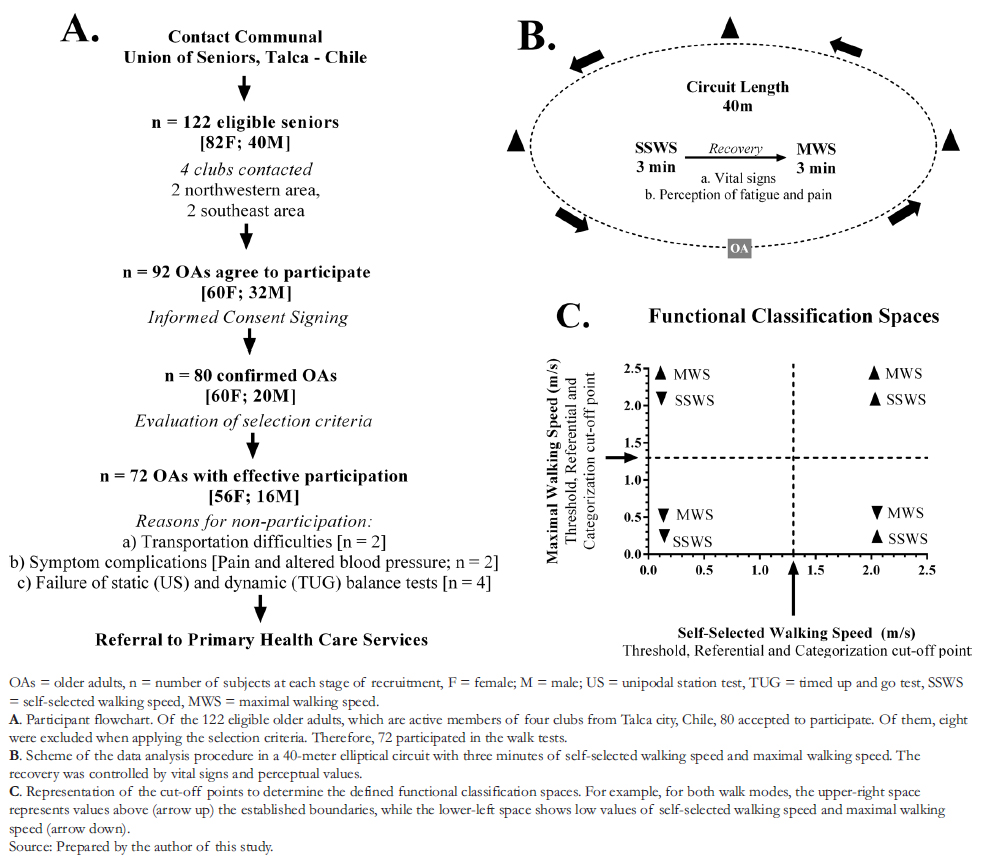
Each older adult signed an informed consent approved by the Scientific Ethics Committee of the Universidad Católica del Maule, Talca, Chile (No. 002/2014). The inclusion criteria were age between 60 to 75 years, self- sufficiency (periodic functional assessment of older adults-Chile, part A > 42 points), normal weight or overweight (according to body mass index), no risk of falls (negative timed up and go and unipodal station tests), normal cognitive level (abbreviated Mini- Mental State Examination > 13 points) and no established depression (Yessavage Scale < 5 points) [7]. Older adults with sequelae of diseases and decompensation of vital signs or pain were excluded (Figure 1A).
Procedures
The data collection was carried out in a university setting during February and March 2015. Participants were required to attend with comfortable clothing and regular footwear and were evaluated in morning sessions (09:00 to 11:30 a.m.). Two physical therapists with gerontological experience measured the variables of interest.
Participants were asked to perform three minutes of "usual walk" (self- selected walking speed). Then, after verifying recovery in a sitting position (3 ± 3 minutes), patients performed a "demanding walk" (maximal walking speed) in a 40 meters elliptical circuit on a homogeneous surface (Figure 1B), recording the total walking distance to calculate the average speed (meters traveled/180 seconds). The time and distance of the walking test have been previously established to extrapolate the results to daily activities [29],[30],[31].
Definition of functional classification spaces
Each functional classification space was determined by a crossing line between the speed value of self- selected ("x" axis) and maximal ("y" axis) performance. The results were represented by a scatter plot of self- selected walking speed versus maximal walking speed points, incorporating the cut- off point’s criteria according to the established limits (Figure 1C).
The "threshold" is defined as the boundary of self- selected walking speed [17],[18] and maximal walking speed [17] for the development of basic daily activities. The "reference" is the normative speed for a self- selected and maximal walk speed [16], representing instrumental and community contexts. The “functional categorization” according to speed was determined for: i) household walker (< 0.4 meters per second, m/s), ii) limited community ambulator (0.40 to 0.80 m/s), iii) community ambulator (0.81 to 1.3 m/s) and iv) cross street safely (> 1.3 m/s) [12].
Data analysis
The data were described by mean ± standard deviation. Through a scatter plot, each older adult is represented by a point which is obtained between self- selected walking speed ("x" axis) and maximum walking speed ("y" axis), Figure 1C. The results of the location and distribution of older adults (i.e., graph points) were presented in percentage according to coordinates on the graph (i.e., Functional Classification Spaces). The graphs were developed using the GraphPad Prism 6.0 pro-gram (San Diego, CA, USA).
 Full size
Full size Results
The general characteristics of participants are presented in Table 1. The age is around 70 years for both sexes, and most are overweight. In the periodic functional assessment of older adults, section A presents an average of 51 out of 54 possible points.
All older adults exceeded the barrier of 1 m/s, and the increase from self- selected walking speed to maximal walking speed was ≈0.2 m/s in women and ≈0.3 m/s in men. The relationship between the study results and the "threshold" values was almost three times higher for self- selected walking speed and two times higher for maximal walking speed. Compared with the "refer-ence" values, women reach 90% and men between 70 to 80% (Table 2).
Concerning the percentage of subjects for each functional classification space, participants exceeded the "threshold" in 100% of cases (Figure 2A). The results concerning the "reference" values are distributed in ≈80% for both sexes in the spaces that represent a self- selected walking speed and maximal walking speed below the limit value. In the same way, ≈20% of the participants present a surplus only in the self- selected walking speed (Figure 2C and D).
Figure 2B represents functional classification spaces distribution according to the pre- established "functional categorizations". All self- sufficient older adults exceed the boundary required to develop activities within the home (household walker). In the case of limited community roles (limited com-munity ambulator), the female sex presents three participants in its upper limit (5%). Also, 81% of women and 69% of men are effectively within the established community space (community ambulator). In the space of effective street crossing (cross the street safely), men double the percentage of women (31% versus 14%).
 Full size
Full size  Full size
Full size  Full size
Full size Discussion
This study sought to explore functional classification spaces by walking speed in Chilean self- sufficient older adults, according to threshold values [17],[18], normative references [16], and boundaries of functional categorization [12]. The main findings are that most participants are below the average walking speed according to age range (Figure 2C and D) and below the categorization boundary for efficient street crossing (Figure 2B).
Explanatory factors: anthropometry, environment, and measurement criteria
According to the inverted pendulum model, the length of the lower limbs influences walking speed [32]. Moreover, speed is also related to height, which is highly variable among populations [16],[17],[18],[33],[34]. Height explains 20% of the variation in stride length in community- dwelling older adults, conditioning self- selected walking speed [33]. For maximal walking speed, predictive equations establish height as a factor that significantly explains the distance covered in sub- maximal exercise tolerance tests [34]. For that reason, Bohannon [16] presents height- normalized reference values for self- selected and maxi-mal walking speeds. When applying this methodology in this study, the self- selected walking speed is similar between sexes and reference values, while differences are found for maximal walking speed (Table 2).
Another factor that could have influenced the differences in the results is the measurement procedure of walk speed. Wang et al. established the measurement distance and the acceleration and deceleration phases as the most influential elements [35]. Also, Ng et al. determined that measurement lengths of five, eight, and 10 meters do not affect the self- selected walking speed and maximal walking speed, producing consistent results from a clinical point of view. For applicability reasons, Ng. et al. recommend 5- meter corridors considering two meters for acceleration and deceleration [36]. The study of reference values uses a 7.62- meter corridor length without considering two meters for acceleration and two meters for deceleration [16], so the effective distance was fewer than four meters and, there-fore, less than the validated minimum. Furthermore, from the functional point of view, Salbach et al. establish 10 meters as the limit register to extrapolate the results of the safe street crossing [31].
n the present study, a distance of 40 meters was used in an elliptical circuit while recording temporality in three minutes to reach a "steady state" [30]. These time and distance measurements are relevant to this age group’s functional daily life activities [28],[29],[33]. The lower average walking speed of the present study can be explained by the omission of the acceleration phase for the speed recording (achieving a steady- state), so this value would be the closest to the older adults' community activities.
What are the risks for underdiagnosed older adults?
In the present study, all older adults were classified as "self- sufficient" according to the periodic functional assessment of older adults (Table 1) and exceeded the threshold values of walk speed (Figure 2A). However, Shinkai et al. estimated for community- dwelling Japanese older adults that speed values similar to those obtained in this study are associated with the risk of losing functionality within the next six years – which is ≈two times for self- selected walking speed (risk ratio: 1.76; 95% confidence interval: 1.02 to 3.04) and ≈five times according to maximal walking speed (risk ratio: 5.15; 95% confidence interval: 2.71 to 9.77) (26). Similarly, most participants have a walking speed below the documented reference [16] (Figure 2C and D) and do not achieve the functional classification space boundary for efficient street crossing [12] (Figure 2B). These results border the speed cut- off points for older adults that do not achieve 8000 steps per day for self- selected walking speed (≤ 0.97 m/s) and maximal walking speed (≤ 1.39 m/s) [11]. This threshold of steps per day is considered a protective indicator for cardiovascular risk and moderate to intense levels of physical activity [11], which according to the guidelines of active and autonomous aging, are linked to the quality of life and optimization of opportunities for carrying out daily activities and roles [2].
The classification of self- sufficient older adults also includes an essential group who present risks of i) functional dependence in the medium term and ii) walking limitations in community contexts (instrumental and advanced activities) [8], which are currently not investigated and intervened.
Complementary proposal for the periodic physical examination
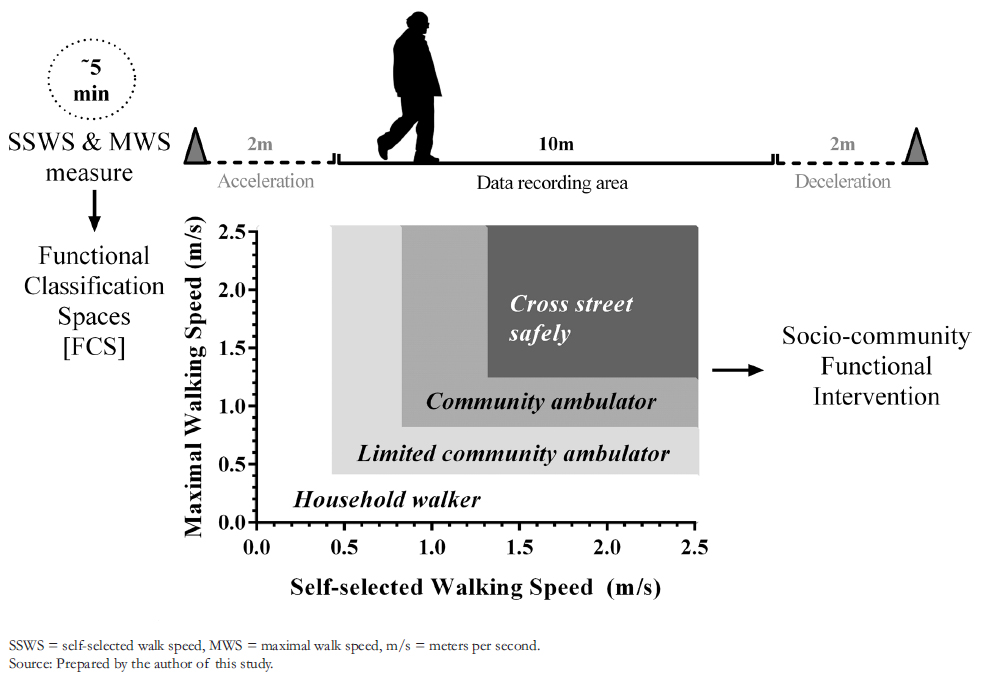
According to the health objectives of the decade 2011- 2020, older adults' central purpose is to improve functional health status [37]. We need to perform comprehensive gerontological evaluations [2], including self- selected and maximal walking speed indicators. By this, we may specify the functional prediction of periodic physical examination (i.e., preventive medicine exam of the elderly) and assess capacity and functional reserve in community- dwelling older adults.
Figure 3 represents the proposal to incorporate walk speed into the functional prediction tools. A 10 meters flat registration surface free of obstacles and 4 meters of non- registration is required. This configuration guarantees a speed with the most negligible incidence of acceleration and deceleration [38], an automated motor gesture [39], and that it is capable of being functionally extrapolated [31].
Among the limitations of this study is the difficulty of fully extrapolating these results to Latin American primary health care services (sampling and recruitment reasons), the necessity to use references from other regions of the world, and the impossibility of analyzing the effects of demographic [16],[22],[25], socioeconomic [29],[40] and health [9],[13],[14],[15] variables. It is projected to have "threshold", "reference", and "functional categorization" values validated according to the characteristics of the Latin American older adults' environment, in addition to incorporating the type of stimulus in the maximal walking speed characterization [41]. It will be relevant to establish the mini-mum speed requirements according to geographical and climatic factors, the surfaces' characteristics, and the dynamics of pedestrian traffic used in the urban systems.
 Full size
Full size Conclusion
The exploration of functional classification spaces according to self- selected walking speed and maximal walking speed applied to a group of self- sufficient older adults results in individuals at risk of deteriorating instrumental and advanced activities of daily living.
Notes
Contributor roles
PM- G is the sole author of this manuscript.
Acknowledgments
The author thanks all the participants in this study, especially the Communal Union of Seniors, Talca - Chile.
Competing interests
There are no competing interests regarding this manuscript.
Funding
The author declares that he did not receive funding to carry out this work.
Ethics
This study has the approval of the Scientific Ethics Committee of the Universidad Católica del Maule, Talca, Chile (No. 002/2014).
Provenance and peer review
Not commissioned. Externally peer- reviewed by four reviewers, double- blind.
Language of submission
English.
