Protocols
← vista completaPublished on July 29, 2020 | http://doi.org/10.5867/medwave.2020.06.7974
Prevalence and incidence of dental caries associated with the effect of tooth brushing and fluoride varnishing in schoolchildren at Galapagos Islands, Ecuador: Protocol of the EESO-Gal study
Prevalencia e incidencia de caries dental y efecto del cepillado dental acompañado de barniz de flúor en escolares de Islas Galápagos, Ecuador: protocolo del estudio EESO-Gal
Abstract
Introduction Dental caries is the most prevalent oral disease in Ecuador. In our country, there are no studies that have included the population of the Galapagos Islands. Fluoride application to incipient lesions of dental caries has shown to be effective in avoiding the use of invasive restorative procedures.
Objectives The objective of the EESO-Gal study is to determine the prevalence and incidence of dental caries and to evaluate the effect of supervised dental brushing, accompanied by periodic applications of fluoride varnish on incipient precarious lesions of schoolchildren in the Galapagos Islands. This article presents the protocol of the EESO-Gal study.
Methods A cohort is planned with Galapagos Islands schoolchildren to determine the prevalence and incidence of dental caries, with assessments every six months, during twenty-four months.
Results We expect to determine the prevalence and incidence of caries every six months, for twenty-four months, in schoolchildren between three and ten years of age, and obtain data to show the state of the caries conditions in Galapagos schoolchildren, with the inclusion of daily brushing at school, supervised by the teacher, and with the application of fluoride varnish every six months.
Conclusions The prevalence of dental caries and incidence after the program will demonstrate the importance of implementing oral health prevention and promotion actions to create hygiene and health habits from an early age.
Key ideas
|
Introduction
Dental caries is a dynamic process of multifactorial etiology[1], resulting from a dysbiosis or rupture of the intricate balance of the oral microbiome[2],[3]. It promotes an alteration of the mineralized tissues of the teeth regarding bacterial deposits[4], which, over time, produce the dissolution of hydroxyapatite crystals by the action of organic acids[5]. In this process, factors such as poor oral hygiene, lifestyle, type of diet[6], age, affective and socioeconomic aspects are related; these components cause dental caries to be distributed heterogeneously in different populations[7].
The World Health Organization (WHO) estimates that, worldwide, dental caries affect about 2.4 billion people with permanent teeth and 486 million with deciduous teeth[8]. The Pan American Health Organization (PAHO) estimates that, in the region, caries affect more than 90% of children[9]. A continuous and slow onset of the pathology is highlighted[10], where the first clinical manifestation is a white spot[11] that can be reversed if there is an adequate diagnosis and early intervention[12].
The actions to control the lesion in these incipient stages are restricted to preventing its progression[13]. Strategies such as tooth brushing, the application of fluoride, and even the placement of pit and fissure sealants on occlusal surfaces of the posterior teeth[14],[15] have shown to be effective in avoiding invasive restorative procedures[16]. Other interventions could be considered with these treatments, such as the use of elements of the xylitol type, caseins, and chlorhexidine[17],[18].
The Ecuadorian population has a high prevalence of caries[19], and an increase in the Decayed, Missing, and Filled Teeth (DMFT) indexes has been evidenced in the epidemiological studies carried out as the age of the individuals increases[20]. In these studies, the population of the Galapagos Islands has not been considered, despite their location and characteristics. Likewise, there are no reports of national studies using the International Caries Detection Assessment System (ICDAS), which is currently considered a more sensitive and specific index[21],[22].
The objective of this protocol is to report the methodology to be applied in the Galapagos Oral Health Study (EESO-Gal) to determine the prevalence and incidence of dental caries and the presence of dental plaque, considering the development of activities associated with tooth brushing and fluoride varnish application to three to ten-year-old schoolchildren, in the Galapagos Islands.
Methods
The execution of a cohort study to determine the oral health status of children between three and ten years of age from San Cristobal, Santa Cruz, or Isabela islands, located in the Galapagos Archipelago, Ecuador, is proposed. Five visits will be made to determine the prevalence and incidence of caries and bacterial plaque. To calculate the sample size, the total school population of the Islands, 2 243 children, was taken into account. Through the Grandaria Mostral statistical program (GRANMO), a necessary sample of 837 individuals was estimated, with a confidence of 95% and an accuracy of +/- 3 percentage units, with a population percentage that is expected to be around 50%. It is anticipated that the percentage of necessary replacements will be 20%. In this way, the sample will be distributed in educational units on the islands of Santa Cruz, Isabela, and San Cristobal.
All children from all schools will receive an invitation to be part of the project. All students, whose parents express their acceptance by signing an informed consent, will be considered. Classification of participants by caries risk level, periodontal disease, plaque index or caries stage will not be done.
Selection criteria
Inclusion criteria:
- Boys and girls between three and ten years of age whose permanent residence is one of the following islands: San Cristobal, Santa Cruz, or Isabela, in the Galapagos archipelago.
- Boys and girls whose parents sign the letter of informed consent, thereby accepting participation in the study.
- Boys and girls who are enrolled and regularly go to schools that agreed to participate in the study.
- Boys and girls who agree to participate in the study through acceptance of informed consent and who show a slightly positive and definitely positive collaboration, according to the Frankl classification[23].
Exclusion criteria:
- Boys and girls with signs of molar-incisor hypomineralization (HIM).
- Boys and girls with syndromes or chronic degenerative diseases.
Procedures
After enrollment in the study, each child will receive an identification code that will allow monitoring throughout the project. A visual clinical examination of his or her oral cavity will be carried out at each visit. The presence of bacterial plaque will be established according to the simplified Löe and Silness Index[24]. Subsequently, removal of the existing plaque and clinical evaluation of the presence of carious lesions will be performed using the ICDAS classification[25],[26]. In addition, before and after the oral intervention, the child's perception of the procedure will be recorded; the satisfaction criteria of the facial image scale (FIS) will be used[27]. Consequently, the primary variables to be studied will be the presence of bacterial plaque, carious lesions on the different surfaces of the teeth, and the perception of the child concerning the procedure—associated with its corresponding categorical indicator—as summarized in Table 1. The age, residence, and sex of the participants will be considered as a covariate.
After the clinical examination, all participants will receive an oral hygiene talk. From the second visit on, all participants will get fluoride varnish as a preventive method. All the activities described will be completed in the educational institution—in classrooms adapted for the project.
 Full size
Full size Plaque index assessment
The presence of dental plaque will be assessed according to the simplified Löe and Silness Index. The vestibular or palatal/lingual surfaces of the permanent central incisors (teeth 1.1 or 2.1 and 3.1 or 4.1) or temporary (teeth 5.1 or 6.1 and 7.1 or 8.1) and definitive first molars (teeth 1.6, 2.6, 3.6 and 4.6) will be explored. In case the last mentioned are lacking, the second temporal molars (teeth 5.5, 6.5, 7.5 or 8.5) will be examined. The evaluation will be performed using the OMS probe on the tooth surface, starting the inspection from the upper teeth on the right side. The assessor will record the plaque level with code zero in the absence of dental plaque; code one in the absence of dental plaque seen with the naked eye and that can only be recognized by passing a probe through the tooth surface; code two in the presence of plaque at simple sight; code three in the presence of dental plaque, as observed with the naked eye even in interproximal spaces and in the presence of dental calculus[24].
Caries assessment
The presence of carious lesions will be recorded by ICDAS classification according to their visual-clinical appearance[25]. A mouth mirror and a WHO probe will be used as complementary instruments to the visual inspection. The different degrees of injury will be recorded according to ICDAS II criteria: code zero, healthy tooth surface; code one, first visual change in enamel, white or brown lesion, observed after drying the tooth surface; code two, white or brown enamel change seen on a wet tooth; code three, localized enamel injury due to caries without visible dentin; code four, underlying dark shadow in dentin, with or without localized enamel fracture; code five, cavity with exposed dentin; code six, large cavity with visible dentin[28]; code fifty, missing tooth.
Evaluation of the degree of satisfaction
Before and after the oral analysis, the child's perception of the procedure will be recorded in the file using the satisfaction criteria of the facial image scale. Representative figures of faces, classified from happy to sad, will be used to evaluate satisfaction with the dental treatment[27]. The happy face will indicate very satisfactory treatment, the serious face will indicate that the treatment was moderately satisfactory, and the sad face will indicate that the treatment was unsatisfactory.
Supervised tooth brushing
At the completion of the oral health diagnosis, the participants will receive an oral hygiene kit along with motivational activities and instruction on oral hygiene techniques. The teaching of the "Modified Bass" brushing technique will be emphasized, both to participants and teachers. The kit will remain in the educational institution and will be used for tooth brushing. This procedure will be supervised by teachers, who had been previously trained by researchers belonging to the institutions that co-finance the project (universities) and dentists from the Ministry of Public Health of Ecuador. Teachers from educational institutions will inspect this community activity daily. In addition, staff from the Ministry of Public Health of Ecuador will conduct dental brushing monthly, with educational talks to participants and teachers.
Fluoride varnish application
From the second visit on, all participants will receive the application of fluoride varnish at 22 600 ppm (Duraphat®, Colgate Palmolive) on their dental surfaces; this procedure will be executed every six months until the study is completed. The application will be supervised by nine researchers (AAV, ACR, AGZM, CPF, GML, IOR, MCZB, MJCD, MPG) and fulfilled by dentists from the Ecuadorian Ministry of Public Health, following the recommendations for its application in community conditions: cleaning and drying of dental surfaces with gauze, with partially isolated and dry teeth; application of a thin layer of fluoride varnish, by quadrants, starting from the molar to incisor area; ending with the instruction of not eating food, for at least three hours, and of abstaining from tooth brushing[29].
Evaluator standardization
As a previous step, the evaluators (specialist dentists) involved in the study received training and coaching on the actions to be developed (assessment of the state of collaboration according to the Frankl classification, differential diagnosis between molar incisor hypomineralization and fluorosis, assessment of the presence of bacterial plaque according to the simplified Löe and Silness Index, assessment of caries according to the ICDAS system, assessment of satisfaction with the intervention according to criteria of the facial image scale and instructions on the application of fluoride varnish). The ICDAS evaluation system was standardized. Only obtaining a grade higher than 0.65 points in the Kappa intra and inter exam, enabled them to act as evaluators and received a certificate of this process, issued by Global Management Collaborative Caries (GCCM); the mean inter-examiner reproducibility score was 0.83, and the intra-examiner reproducibility was 0.81.
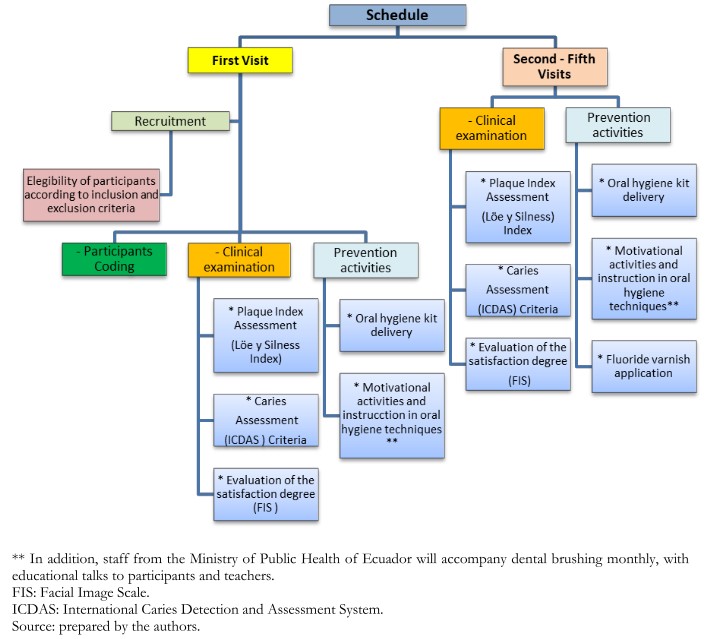
Schedule of activities to be accomplished
A total of five periodic visits will be made, every six months for two years, to the participating schools. During the first visit, participants will be recruited according to inclusion and exclusion criteria. The schoolchildren included in the study will undergo a clinical examination that will determine the presence of bacterial plaque according to the simplified Löe and Silness Index, presence of dental caries using ICDAS, and evaluation of the degree of satisfaction with the procedures carried through. In addition, the planned preventive activities of education and instruction on oral hygiene will begin.
From the second visit to the last visit, the clinical evaluation will be done, as well as the described preventive activities, and the application of fluoride varnish with 22,600 ppm will be added, following the previously established protocol (see Figure 1).
 Full size
Full size Data management
The data obtained after each evaluation will be stored in specific sheets, and registered in Excel tables, identifying each participant with a numerical code. The sheets will be sent to the principal researcher (AAV), who will coordinate the entry and filtering of the obtained information in the statistical program. The storage and custody of the files will be the principal researcher's responsibility, preserving the participant's confidentiality, and using the data only for research purposes.
Analysis of data
The data will be analyzed using the SPSS statistical package in its 23rd version. For the description of the categorical variables, frequencies and percentages will be used; for quantitative variables, means and their standard deviation or medians and interquartile ranges will be described according to the characteristics of the variables. The normal distribution of the evaluated variables will be verified using the Kolmogorov-Smirnov test.
The prevalence of caries will be considered as the primary variable, taking into account the ICDAS scores at two cut points: ICDAS greater than three, to compare it with the DMFT or DMFS score, and the ICDAS scores of one, two and three, using the Student T-test or the Mann–Whitney U test, as appropriate for hypothesis testing of these scores, with a significance value of less than 0.05 for all the analyzes to be carried out. Additionally, comparative studies will be performed by means difference for samples related to the scores, considering the baseline, and at six, twelve, eighteen, and twenty-four months of follow-up.
Discussion
Currently, there are different strategies for controlling caries that are based on the use of fluoride incorporated in salt consumption, drinking water, toothpaste, and mouthwashes as the main preventive measures[30]. Other strategies are the placement of pit and fissures sealants, xylitol in chewing gums, and the control of sucrose consumption in the diet[31]. The application of fluoride varnish is recognized as one of the main tools in the prevention and control of dental disease when it is applied every three to six months. This practice considerably reduces dental caries in children[30],[32],[33]. Different results have been reported, attributing to limited and inconclusive evidence of the preventive effect of the topical application of fluoride varnish against dental caries in permanent and deciduous teeth[34].
In Latin America, the prevalence of caries in schoolchildren is high. Studies done in Ecuador describe its presence in 75.6% of the school population between six and fifteen years of age[19]; in Chile, the prevalence reaches 70.36% in six-year-olds and 66.9% in twelve-year-olds[35]. The Peruvian Ministry of Public Health reports that 85.6% of schoolchildren have cavities[36]; in Colombia, the prevalence reaches 51%[37]. Studies in other parts of the world, such as Saudi Arabia, indicate that eight out of ten children from six to eight years of age suffer from this condition[38]; in Italy, these values reach 44.97% for twelve-year-old children[39]. These data show that reinforcing strategies and decisions, from a public health point of view, are required to decrease the prevalence of dental caries.
The existing data in Ecuador have not incorporated the population of the Galapagos Islands and the influence that promotion and oral health activities have had so far, which is why it is necessary to carry out this type of project and propose modifications to health policies if necessary. At the same time, this observational study will be the first to establish a baseline of dental plaque and caries in schoolchildren in the Galapagos Islands.
One of the strengths of this cohort study is that the Galapagos Islands feature a population with little migration, an ideal condition for the execution of this project, which, due to its intervention characteristics, requires monitoring over time. However, one of the limitations that we consider is that the study will be carried out in children, and, as they lack autonomy due to age, the results will depend entirely on the collaboration of parents and caretakers.
Notes
Authorship roles
All the authors contributed to the conceptualization, development, and design of the project, in the writing or critical revision of the manuscript, and the approval of the final version of the article.
Acknowledgment
We would like to thank MSc. Susana Hidalgo, professor at Universidad UTE, for her advice in translating this article into English. Also, MSc. Walter Vega, Stomatology Director of District 20D01 of the Ecuadorian Ministry of Public Health, for his collaboration in the logistics required to this study.
Competing interests
The authors declare that they belong to one of the four higher education institutions that co-finance this study as a conflict of interest and that Colgate Palmolive financed the calibration process for the ICDAS scale assessment.
Funding
This research project is co-financed by Universidad UTE, Universidad Católica de Santiago de Guayaquil, Universidad de Guayaquil, and Universidad San Gregorio de Portoviejo. Colgate Palmolive Company will finance the delivery of oral hygiene kits (toothbrush and toothpaste), as well as fluoride varnish (Duraphat®) for periodic application according to the established protocol. None of these institutions will influence the analysis and reports of the future results of this work.
Ethical considerations
The study will be developed in accordance with the principles established in the International Ethical Guidelines for Biomedical Research and Experimentation in Human Beings of the World Health Organization (CIOMS). The proposal has the approval of the Ethics Committee of Eugenio Espejo Hospital (resolution number CEISH-HEE-01.08.2017), recognized by the Ministry of Public Health of Ecuador and the Directorate of Health Intelligence, complying with the requirements established by these institutions. The researchers' team declares, freely and voluntarily, that the project described in this document is an original work, the authors of which are part of the team of investigators. The project does not violate any legal or ethical regulation and has prior permits to its execution.
From the editors
The original version of this manuscript was submitted in Spanish. This English translation was provided by the authors and has been copyedited by the Journal.
