Epistemonikos summaries
← vista completaPublished on June 9, 2016 | http://doi.org/10.5867/medwave.2016.6463
Is preemptive antifungal therapy a good alternative to empirical treatment in prolonged febrile neutropenia?
¿Es la terapia antifúngica "preemptive" (anticipada) una buena alternativa a la terapia empírica en pacientes con neutropenia febril prolongada?
Abstract
Patients with prolonged febrile neutropenia are at high risk of invasive fungal infection, so it has been standard practice to initiate empirical antifungal therapy in these cases. However, this strategy is associated with important toxicity, so diagnostic test-guided preemptive antifungal therapy has been proposed as an alternative. Searching in Epistemonikos database, which is maintained by screening 30 databases, we identified three systematic reviews including twelve studies overall. Four randomized controlled trials addressed the question of this article. We combined the evidence using meta-analysis and generated a summary of findings following the GRADE approach. We concluded it is not clear whether preemptive strategy affects mortality because the certainty of the evidence is very low, but it might slightly decrease the use of antifungal agents in patients with prolonged febrile neutropenia.
Problem
During chemotherapy-induced neutropenia fever occurs frequently but clinical infection is documented in only 20-30% of febrile episodes [1]. Invasive fungal infections usually appear after the first week of prolonged neutropenia and empirical antibiotic therapy, and constitute an important cause of morbidity and mortality [2]. It has been standard practice to initiate empirical therapy for fungal infections in patients with prolonged febrile neutropenia, and this approach has been incorporated into several guidelines. Approximately 40–50% of patients are treated with antifungals using this empirical approach, whereas the estimated actual incidence of invasive fungal infection is around 10–15% [3]. As a result, many patients are potentially exposed to unnecessary toxic treatment and considerable financial burden. Diagnostic test-guided preemptive antifungal therapy, that is antifungal treatment instituted if indicators of possible invasive fungal are identified, has been proposed as an alternative treatment strategy in these patients.
Methods
We used Epistemonikos database, which is maintained by screening more than 30 databases, to identify systematic reviews and their included primary studies. With this information we generated a structured summary using a pre-established format, which includes key messages, a summary of the body of evidence (presented as an evidence matrix in Epistemonikos), meta-analysis of the total of studies, a summary of findings table following the GRADE approach and a table of other considerations for decision-making.
|
Key messages
|
About the body of evidence for this question
|
What is the evidence. |
We identified three systematic reviews [4],[5],[6] including twelve primary studies [7],[8],[9],[10],[11],[12],[13],[14],[15],[16],[17],[18] from which five correspond to randomized controlled trials [9],[10],[13],[15],[18]. One of the trials was excluded from this summary since it does not compare against empirical strategy [9]. This table and the summary in general are based on the four pertinent randomized controlled trials [10],[13],[15],[18]. |
|
What types of patients were included |
Two studies included only adults [10],[15], one study included both adults and children [18] and one study did not report the age of the patients [13]. All studies included only patients with hematological malignancies. One study included only patients who received allogenic stem cell transplant [13], and the other three included patients undergoing chemotherapy or allogenic stem cell transplant [10],[15],[18]. |
|
What types of interventions were included |
All studies used different criteria for starting antifungal therapy in the preemptive strategy, and different tests for early diagnosis of invasive fungal disease. Three studies used galactomannan test twice a week [10],[15],[18]; one study used nested PCR for Aspergillus [15] and one study non-nested PCR for Aspergillus and Candida [13]; only one study performed blood cultures [13]. All studies used imaging as diagnostic test; two studies performed chest computed tomography if serological tests were positive [15],[18], one study performed chest and abdomen computed tomography to all patients [13], and one study performed chest radiography followed by chest computed tomography [10]. |
|
What types of outcomes |
Different systematic reviews reported meta-analysis for the following outcomes:
|
Summary of findings
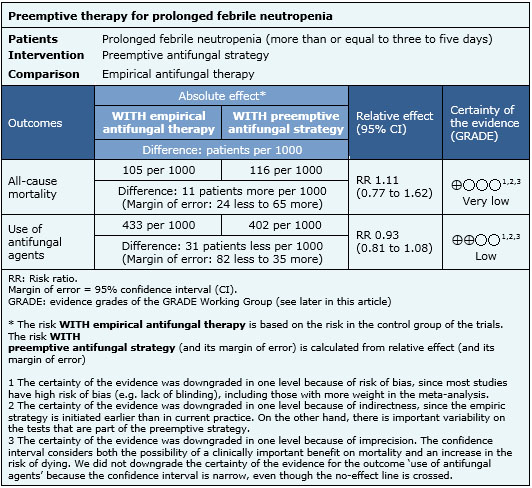
Information on the effects of preemptive strategy is based on four randomized controlled studies involving 988 patients [10],[13],[15],[18]. All of them provided information on the use of antifungal therapy, and three studies provided information on all-cause mortality [10],[13],[15]. The summary of findings is the following:
- It is not clear whether preemptive strategy affects mortality because the certainty of the evidence is very low.
- Preemptive strategy might slightly decrease the use of antifungal agents in patients with prolonged febrile neutropenia.

Other considerations for decision-making
|
To whom this evidence does and does not apply |
|
| About the outcomes included in this summary |
|
| Balance between benefits and risks, and certainty of the evidence |
|
| What would patients and their doctors think about this intervention |
|
| Resource considerations |
|
|
Differences between this summary and other sources |
|
| Could this evidence change in the future? |
|
How we conducted this summary
Using automated and collaborative means, we compiled all the relevant evidence for the question of interest and we present it as a matrix of evidence.
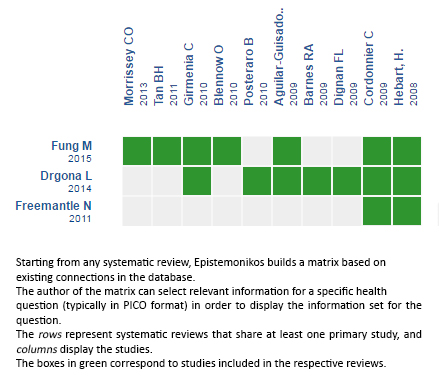
Follow the link to access the interactive version: Preemptive antifungal strategies in febrile neutropenia
Notes
The upper portion of the matrix of evidence will display a warning of “new evidence” if new systematic reviews are published after the publication of this summary. Even though the project considers the periodical update of these summaries, users are invited to comment in Medwave or to contact the authors through email if they find new evidence and the summary should be updated earlier. After creating an account in Epistemonikos, users will be able to save the matrixes and to receive automated notifications any time new evidence potentially relevant for the question appears.
The details about the methods used to produce these summaries are described here http://dx.doi.org/10.5867/medwave.2014.06.5997.
Epistemonikos foundation is a non-for-profit organization aiming to bring information closer to health decision-makers with technology. Its main development is Epistemonikos database (www.epistemonikos.org).
These summaries follow a rigorous process of internal peer review.
Conflicts of interest
The authors do not have relevant interests to declare.
