Estudios originales
← vista completaPublicado el 5 de marzo de 2024 | http://doi.org/10.5867/medwave.2024.02.2770
Caracterización de la conducta suicida en población general de la Región de Coquimbo (Chile) entre 2018 y 2020
Characterization of suicidal behavior in Coquimbo, Chile, between 2018 and 2020
Abstract
Introduction Suicidal behavior is a public health problem worldwide. The World Health Organization estimated 700 000 deaths for the year 2021.
Objective This study aimed to estimate the prevalence of suicidal behavior and describe its related factors in the Coquimbo Region, Chile, between 2018 and 2020.
Methods 2190 suicide attempt notifications from the regional epidemiological surveillance system were analyzed, corresponding to 1781 people, along with 217 reports from the Forensic Medical Service of people who died by suicide.
Results The overall suicide rate for the region during that period was 9.79 deaths per 100 000 inhabitants. The 2018 rates were standardized according to available information, with direct methods for the regional rate (9.55 per 100 000 inhabitants) and indirect methods for the communes. Rural communes presented higher rates than urban ones. Women showed a higher risk of attempts (OR 1.28; 95% CI 1.23 to 1.33) and a lower risk of suicide compared to men (0.086; 0.06 to 0.13). Young people had a higher risk of suicide attempts and a lower risk of suicide compared to older people. The increased suicide rates in older people (70 to 79 years) during 2020 are noteworthy. Basic education level is a risk variable for suicide (2.21; from 1.15 to 4.23), compared to having higher education. Previous suicide attempts and psychiatric pathology are risk factors.
Conclusions Suicide prevalence and related factors are similar to those reported in other studies and national reports, highlighting rurality and higher risk in older male adults. In contrast to suicides, attempts are more frequent in women and young people. A history of mental health problems, previous attempts, and family violence are risk factors for both outcomes. Knowing the patterns of suicidal behavior in the population is fundamental for its prevention.
Main messages
- Suicidal behavior is a relevant public health problem little studied in Chile.
- The study includes a review and analysis of three years of data on suicide mortality and records of suicide attempts from the regional surveillance system.
- The prevalence of suicide and suicide behavior-related factors are similar to those reported in other studies and national reports.
- Limitations are related to the quality of the suicide attempt records and that the study period was only three years, making it difficult to make projections.
Introduction
Suicide is understood as the death caused by harming oneself with the intention of dying, while attempted suicide is when someone harms himself with the intention of ending his life but does not die as a result of his actions [1]. The most recent theory of suicidal behavior is the three-step theory, which refers to the fact that:
-
Suicidal ideation is caused by a combination of unbearable pain (usually psychological) and hopelessness.
-
Suicidal ideation is strongest when the pain exceeds or overwhelms, disrupting valued or meaningful personal and/or social connections.
-
The transition from suicidal ideation to potentially lethal intent is facilitated by the willingness and practical contributors to develop suicidal capacity.
This theory has been used as a basis for guiding suicide prevention education programs [2]. It is theorized that suicidality, i.e., knowledge of, access to, and experience with lethal means, facilitates the passage from suicidal ideation to suicide. Thus, painful and provocative events seem to contribute more to practical ability than low fear of death. However, the small number of studies does not allow us to draw conclusions about the factors that contribute to the practical ability of committing suicide [3].
There is evidence that suicide is associated with a higher prevalence of suicide attempts in the lifetime of those affected [4,5,6], with previous attempts being the main risk factor identified [2]. Hence, the importance of characterizing both suicides and attempts. Other factors associated with suicide are depression, substance abuse, loss experiences, loneliness, discrimination, relationship breakdown, financial problems, chronic pain and illness, explosive personality, previous hospitalizations, violence, abuse, and humanitarian emergencies [4,7,8]. Recently, an increase in the incidence of suicide during the first year of the pandemic has been described [5]. Likewise, several authors report a higher risk of suicide in rural areas than in urban areas [6,9], alluding to an association with unemployment [9].
The World Health Organization (WHO) estimated more than 700 000 suicide deaths by the year 2021, representing the fourth leading cause of death in people between 15 and 34 years of age [1]. Mental health problems are the leading cause of years of life lost worldwide [10], despite a reported 5.9% reduction in the number of years lost globally due to suicide in the last 30 years [11]. International studies before 2020 estimate that the prevalence of suicidal ideation in the general population ranged from 5 to 16%, while about 1 to 8% may have attempted suicide in the past year and once in a lifetime, between 3 and 6% [12,13]. In the United States, a study described that the increase in suicidal ideation increased by 28% during the COVID-19 pandemic, while a meta-analysis found that during the pandemic, 13% of the studies showed suicidal ideation and 1% made attempts [14,15]. Factors related to the increased risk of suicide during the pandemic are related to low social support, loneliness, physical and mental fatigue, self-reported poor health, sleep, and mental health problems, among others [12,16].
Suicidal behavior has been scarcely studied in our country. Chile presented an age-standardized suicide rate of eight deaths per 100 000 inhabitants in 2019, being higher in men than in women (13.3 versus 3 per 100 000 persons, respectively) [2]. According to the Legal Medical Service, in Chile, the number of suicides has increased from 3.3 suicides per day in 2000 to 5.5 deaths in 2010 [17]. In the country, mortality records are of high quality but have few variables, which makes it difficult to characterize deaths. For more and better information to characterize suicidal behavior in Chile, it is necessary to resort to the death registries of the Legal Medical Service. In addition, the health authority has more detailed records of suicide attempts reported by emergency units and various healthcare centers.
The Chilean evidence on suicide attempts is more limited than for suicides. A study on suicidal behavior and psychiatric disorders in Chile found that women triple the risk of suicide attempts compared to men [18,19] and that older adults seem to be less exposed to suicide attempts compared to young people. This tendency repeats itself in ideation and in desires of being dead. The same source reports that the lower the educational level, the higher the risk of any of the suicidal behaviors [18].
The Coquimbo Region registered 8.2 suicide deaths per 100 000 inhabitants in 2015, and in 2017, the figure increased to a rate of 10.2, exceeding the national average, where the rate for men is three times that of women [17]. At the time of writing this article, there are no published studies on suicide attempts in the Coquimbo Region.
Given the scarce evidence on suicidal behavior in that region, the study aimed to estimate the prevalence of suicidal behavior and describe factors related to this behavior in the Coquimbo Region between the years 2018 and 2020. It is expected that the resulting characterization will serve to guide preventive programs.
Methods
Study design
This is a descriptive cross-sectional study on suicidal behavior in the Coquimbo Region from 2018 to 2020.
Sources of data
Two sources of data were analyzed:
-
2190 suicide attempt notifications from the epidemiological surveillance system of the Regional Ministerial Secretariat of Health.
-
Consummated suicides registered by the Legal Medical Service (n = 217).
Variables
All the registered variables were studied: demographic (sex, age, educational level, occupation, and commune of residence); time (day, month, year of occurrence); medical history (chronic pathologies, psychiatric, mental health treatment, history of violence, substance use) and suicidal behavior (cause, method used, previous suicide attempts, suicide attempts and suicide in the family). In addition, when reporting suicide attempts, the family and clinical history and the cause of the attempt were recorded. An Excel spreadsheet database was created, excluding sensitive case data (name, identification number, and address).
Data sources and measurements
For the age- and commune-specific suicide rates, the numerator was the annual sum of suicide deaths, and the denominator represented the sum of the population indicated in the document Estimates and Projections 2002 to 2035 of the National Institute of Statistics (years 2018, 2019 and 2020) [20]. For 2018, an indirect adjustment was made for each commune, using as a standard the most updated suicide rate available in the country, according to age groups, and calculating the standardized mortality ratios. The regional standardized rate was calculated for the same year with a direct method, using the population of Chile as the standard [21].
Suicide standardized mortality ratio was calculated for each commune by dividing the overall communal rates (2018 to 2020) by the regional rate. The data were entered into the ArcGIS Online geographic information system to obtain the regional map in four ranges of ratios between rates:
-
Zero registration.
-
Mortality ratio equal to or less than 1.
-
Mortality ratio between 1.0 and 1.39.
-
Mortality ratio greater or equal to 1.4.
Statistical analysis
Results were described using absolute and relative percentage frequency measures. Pearson’s Chi-square test was used to determine differences in the distribution of cases according to behavior (suicide and attempt) for the variable categories of sex, age group, and level of education. The confidence level was 95%.
The study was approved by the Suicide Prevention and Mental Health Program of the Coquimbo Health Service and the Department of Health Planning of the Coquimbo Regional Health Ministerial Secretariat, who provided the data via the Transparency Law. The Ethics Committee did not review the study protocol since it was an aggregate analysis of anonymized databases without sensitive data.
Results
From a total of 2190 suicide attempts reported to the Regional Ministerial Secretariat of Health of Coquimbo, 1781 corresponded to people with at least one suicide attempt between 2018 and 2020. The age range of those who attempted suicide was 7 to 91 years old. Of the total of 217 completed suicides in the region (from 2018 to 2020), 208 corresponded to residents of the area, with an age ranging from 12 to 99 years old. The regional prevalence of suicide ranged from 9.24 to 10.17 per 100 000 inhabitants, being higher in 2019 (Table 1). The regional age-standardized rate for 2018 was 9.55 deaths per 100 000 persons. Rural communes consistently showed the highest suicide rates.
Figure 1 presents the map of ranges of age-standardized mortality ratios for each commune, taking the regional rate as a comparison. Two communes (La Higuera and Paihuano) had zero cases. The localities with a low rank were urban communes or those close to an urban radius (La Serena, Coquimbo, and Andacollo), except for Combarbalá, which is farther away. The moderate rank was for less urbanized communes, or those close to cities (Ovalle, Monte Patria, Vicuña, Illapel, and Los Vilos), and the high rank was for rural communes far from urban centers (Río Hurtado, Punitaqui, Canela, and Salamanca).
Map shows ranges of age-standardized suicide mortality ratios, according to communes in the Coquimbo Region, from 2018 to 2020.
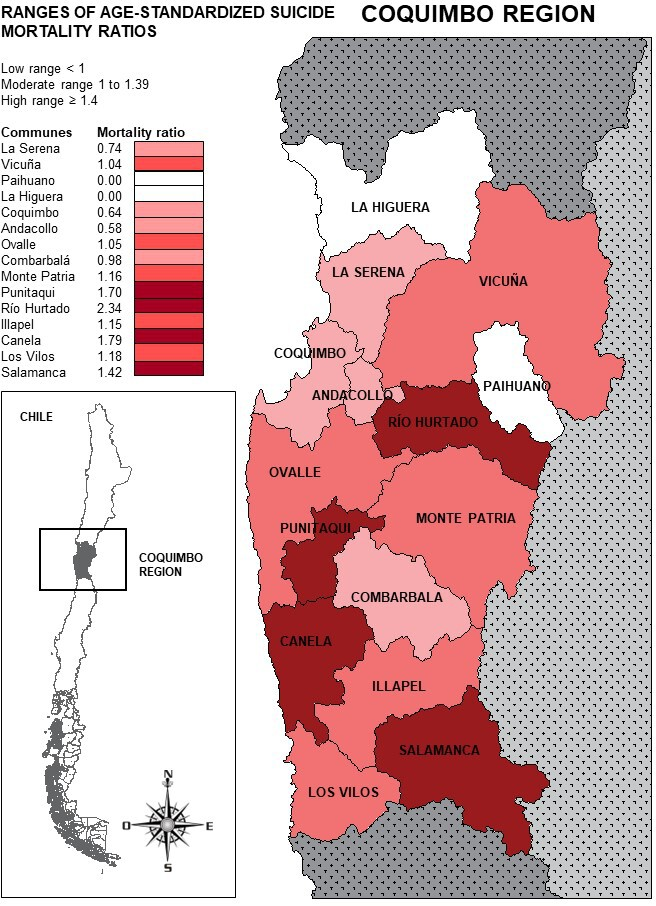
Source: Prepared by the authors with data from the study, using ArcGIS Online.
Table 2 shows the rates by age group. It highlights the increased rates in 2019, especially in the 30 to 39 age group. In 2020, there was an increase in older people aged 70 to 79 years.
Regarding the percentage distribution of cases (Table 3), there is a statistically significant difference between attempted and completed suicide in terms of sex and age distribution, with attempts predominating in women and completed suicides in men. In addition, there were more attempts in young people and completed suicides in adults. Suicide attempts were more frequent during May and November, and completed suicides were more frequent in January.
Table 4 presents the frequencies of the different methods used, both for suicide attempts and suicides, by gender. Statistically significant differences were observed in the method used according to the type of behavior, with drug ingestion being the most frequently used method among suicide attempts (57.9%) and hanging the most frequent form of consummated suicide (89.4%). At the same time, there are significant differences between genders in terms of the methods used. Among suicide attempts, women used more drugs and cutting wounds, while men used more firearms, ingestion of toxins or poison, and hanging (p < 0.001). As for suicides, women commit suicide much less frequently than men, using hanging, cutting wounds, and asphyxiation by suffocation. Men used hanging more frequently, followed by firearms (p = 0.026).
Table 5 shows that about half of those who attempt suicide report one or more previous attempts, and about 60% have a personal history of psychiatric pathology. A quarter of the attempters report a history of substance abuse. Family history of violence, attempts, and suicides are present among attempters in variable proportions, although one-third of the cases reported no history. Slightly more than half of the cases present two or more risk variables, whether these are psychiatric pathologies, substance abuse, violence, or previous attempts. The causes motivating the attempt are also diverse (details in Table 6). It is interesting to note that the distribution of occupations shows variation between suicide attempts and suicides. Among those who attempted suicide, students and workers in the transportation sector predominated, while those who completed suicide were more frequently pensioners and people working in the sales and commerce sectors (Table 7).
Discussion
The prevalence of suicide found (9.7 per 100 000 inhabitants) during the study period falls within the estimated ranges for the Coquimbo Region. It is slightly lower than the national rate for 2018, which was 10.4 per 100 000 inhabitants [22,23], and that of the Araucanía Region (13 per 100 000 inhabitants, from 2004 to 2015) [10]. The higher suicide rates in rural sectors are consistent with those described for Spain and Canada [6,9] and the study conducted in the Araucanía Region [24]. Internationally, the rurality factor has been associated with suicides due to pesticide use [17,25]. However, this does not seem to explain the case due to the low use of pesticides in this region. A more plausible explanation is the difficulty of accessing health centers to address mental health problems associated with a higher risk of suicide [19,26]. This situation is also reflected in our study, which shows a higher prevalence of mental pathologies among the attempters. Social conditions in the rural world, such as isolation, the gaps between life expectations and reality, and personal and work development, could also explain what was observed [9]. It would be of interest to identify the causes behind the higher frequency of suicides in rural areas of our country. The increase in suicide rates in rural communities and the elderly during the year 2020 was probably linked to lockdown and restrictions derived from the pandemic situation, as has already been described in further studies [11,15,16].
Only 11% of the suicide cases were women, while women accounted for 65% of the attempts. Previous studies also agree that women are more likely to make suicide attempts, while men consummate the act more frequently [23,27]. The predominance of older males was also reported in Brazil before the pandemic (2015) [23].
Our information confirms that the most commonly used method for suicide is hanging, followed by firearms, as described at the national level and in the study of the Araucanía Region [17,24]. Toxic substances are not frequently used compared to other countries [4,25]. In addition, the methods used showed differences by gender, which is more relevant in suicide attempts, given that consummated suicide occurs in a low percentage of women. Hanging is the most frequent method used by both genders and in both suicidal behaviors. In the attempts, women also used cutting wounds and ingestion of medication, while men used firearms, hanging, and poison ingestion. It is noteworthy that the methods used by men coincide with those more frequently found in completed suicides.
Concerning age, it is observed that young people attempt suicide more frequently than adults and older people, but it is the latter who end up committing suicide. International studies have warned about the impact of the pandemic on the increase in suicides, with emphasis on the elderly [26,28,29,30].
The results found are consistent with other national studies in that higher education appears to be protective against suicide [24,31]. However, among the suicides, there is a high proportion of people who do not register the data. Other studies agree that unmarried people have a higher frequency of suicide than people with other marital status [9]. In agreement with national and international literature, we observed a high prevalence of mental health disorders, including substance abuse, in people with suicide attempts [17,19,25,31,32].
We suggest an influence of climate on the seasonality of suicide; perhaps changes in sunlight exposure throughout the year seem to explain the increase in suicides during warm months [33]. According to data from the Metropolitan Region, 28% of suicides occur in the spring season [34]. In our region, the month with the highest frequency was January, reaffirming the hypothesis described previously.
Previous studies point to the condition of "attempter" as an important risk factor, suggesting the establishment of interventions aimed at preventing this behavior [28]. Regarding attempts, more than half of the people who attempted suicide had made at least one attempt in the previous three years. The most frequent attempt method used is the ingestion of medication, which is usually less effective than the methods used to achieve suicide (hanging and firearm) [17]. As in other research, a high percentage report a family history of violence [18,19,35] or having mental health problems [7,8,36]. It is of concern that, in our study, only a quarter of them are under treatment.
Among the limitations of this study are the possible underreporting of attempts, especially during the year 2020, due to the pandemic situation and the reduction of healthcare consults. On the other hand, the registration quality of attempts is a limiting factor. However, the quality of the suicide death data is good, being a strength in terms of the validity of the results [23]. The study covers only three years, making it difficult to verify trends in suicidal behavior in the Coquimbo Region.
Finally, the scarce evidence published in Chile on the subject makes it difficult to propose explanations of the phenomenon and to plan interventions to prevent suicidal behavior using a territorial approach. More research is needed on suicidal behavior in our country. The records and publications currently available do not go beyond the simple characterization of the phenomenon and its risk factors, posing certain challenges to studying this phenomenon, which should be oriented toward determining risk algorithms with a personalized perspective and using current technologies [37].
Conclusions
The prevalence of suicide found is similar to that reported in other national studies and slightly lower than the national prevalence. Knowing the patterns of suicidal behavior in the population is essential for its prevention. It is confirmed that factors related to a higher risk of suicide are rurality, male gender, older age, lower level of education, history of mental pathologies, and having made previous attempts. The increased number of suicides in elderly people during the pandemic is relevant. The most common method used was hanging. Although information is limited, suicide attempts are more frequent among women and young people in individuals with a history of psychiatric disease and a history of violence in the family, and the most frequently used method is the ingestion of medication.
