Estudios originales
← vista completaPublicado el 30 de septiembre de 2024 | http://doi.org/10.5867/medwave.2024.08.2784
Factores asociados a prevalencia de recesiones gingivales en alumnos de pregrado de la Facultad de Odontología de la Universidad de Los Andes en 2022
Factors associated with gingival recession prevalence in undergraduate students of the Faculty of Dentistry of the Universidad de los Andes in the year 2022
Abstract
Objective To determine the prevalence of gingival recessions in students of the faculty of odontology at Universidad de Los Andes and the factor associated with its presence.
Methods In this cross-sectional study, a randomized stratified sampling was used to select the students. The sample included 311 undergraduate students evaluated between March and December 2022. The year spectrum was from 17 to 29 years old. Two calibrated examiners intra e interoperator completed a clinical evaluation with a periodontal probe, where the purpose was to diagnose gingival recessions and identify if there were any related factors such as smoking, braces, bruxism, marginal insertion frenulum, fine phenotype, and malposition. The total prevalence was described with each trust interval of 95%. The association between categorical variables was analyzed with the chi-square test, and the t-student test of the Mann-Whitney test analyzed the difference between continuous variables and recession prevalence.
Results 93,56% of the students presented at least one gingival recession. The highest prevalence related to teeth occurred in pieces 1.6, 3.4, 2.6, and 4.1, and the most severe were 3.3, 4.3, and 1.3. The most associated factor related to recessions was orthodontics, with a prevalence of 75,2%. Bruxism showed a positive association with the number of recessions, with a prevalence of 60,7%.
Conclusions Buccal gingival recessions were very prevalent in undergraduate students at the dental school of Universidad de los Andes during 2022, and they were strongly associated with the history of orthodontics.
Main messages
- Gingival recessions are associated with esthetic problems, dentin hypersensitivity, inflammation, bleeding, and plaque retention. In addition, the exposure of the tooth surface increases the risk of root caries and non-carious cervical lesions.
- Few studies on the prevalence of gingival recession are available in Chile, so it is important to establish the frequency of this condition in population groups, such as dental students, to guide public policies with primary or secondary prevention measures.
- The limitations of this study include not being able to extrapolate the results to all age groups and not having analyzed aspects such as factors associated with the presence of healthy teeth, the time and number of orthodontic treatments, years of smoking, or the duration of bruxism, among others.
Introduction
Gingival recession is defined as the migration of the gingival margin apically to the amelocemental junction, exposing the root surface to the oral environment [1]. According to published studies, the prevalence of this condition varies between 30 and 100%, depending on the characteristics of the studied population [2].
The prevalence of gingival recessions varies by country or region. In the United States, according to data from the National Health and Nutrition Examination Survey III (NHANES III), the prevalence of recessions greater than or equal to 1 millimeter was 58% in adults aged 30 to 90 years. The study by Chrysanthakopoulos et al. reported a prevalence of 63.9% in 1430 young adults. In Sri Lanka, according to Löe, it ranged between 60 and 90% in a sample of 480 workers [3,4,5]. In the study by Rivera-Valerio et al., in Peru, an 85.7% prevalence of gingival recession was found among 77 postgraduate students [6]. Among the few studies available in Santiago, Chile, Guerrero reported a prevalence of 93.5% in a population of 703 adults [7].
Gingival recession is a multifactorial condition. Factors related to a higher incidence of gingival recession have been established, including traumatic brushing, the presence of calculus, fine periodontal phenotype, marginally inserted braces, malpositioned teeth, orthodontic treatment, bruxism, inadequate restorations, and smoking, among others [4,8].
Orthodontic appliances turn out to be conditioning factors for the development of gingival recession in thin periodontium. The tooth movement produced by this treatment can create bone dehiscence, which may lead to a gingival recession in the future. For this reason, it is important to diagnose the presence of gingival recession and evaluate the periodontium when orthodontic treatment is indicated. The thickness of the marginal soft tissue overlying the dehiscence is an important factor in predicting this condition during or after orthodontic treatment [2].
The major problems associated with gingival recessions are esthetic and dentin hypersensitivity. These two are the most frequent reasons for consultation among individuals seeking treatment [9]. On the other hand, gingival recessions are associated with periodontal problems, including higher inflammation, bleeding, and plaque retention. Exposing the tooth surface also increases the risk of root caries and non-carious cervical lesions [9].
Considering this background, it is relevant to determine the situation regarding the prevalence of gingival recession in Chile. In addition, it is relevant to establish the frequency of this condition among individuals who may be at higher risk, including dental students, in order to establish primary or secondary prevention measures. Therefore, this study aimed to determine the prevalence of gingival recessions in undergraduate students of the Faculty of Dentistry of the Universidad de Los Andes during the year 2022 and to identify the possible factors associated with their presence.
Methods
A cross-sectional study was carried out. The sample was recruited at the Faculty of Dentistry of the Universidad de Los Andes, in Santiago, Chile. The examination and anamnesis of the undergraduate dental students, who are studying six years to graduate with the degree of dental surgeon, was conducted in their clinical facilities during the year 2022. The sample size was of 311 students out of a total universe of 497. We included students who consented to participate in the study and who provided age and gender information. Gingival recessions on third molars or on palatal sides of the remaining teeth, as well as dental implants, were not considered.
A cross-sectional study was carried out. The sample was recruited at the Universidad de Los Andes Faculty of Dentistry in Santiago, Chile. The examination and anamnesis of the undergraduate dental students, who are studying for six years to graduate with a degree in dental surgery, was conducted in their clinical facilities in 2022. The sample size was 311 students out of a total universe of 497. We included students who consented to the study and provided age and gender information. Gingival recessions on third molars or palatal sides of the remaining teeth and dental implants were not considered.
After signing an informed consent form, the participants completed a questionnaire with their history and habits.
The presence of gingival recessions was evaluated on the vestibular surface of all teeth except the third molars. Gingival recession measurements were taken on three vestibular tooth surfaces (mesial, medial, and distal) using a North Carolina probe (Hu-Friedy®) graduated in millimeters. When the record was a decimal number, it was approximated to the nearest whole number. In the case of being half, the more significant number was considered. These values were entered in a clinical record with a specific periodontogram for each individual.
The position of the gingival margin was analyzed with respect to a fixed reference, which in most cases corresponded to the amelocemental limit. The gingival phenotype was determined by probing the gingival margin in the mid-vestibular region of the upper central incisor. If the periodontal probe lines could be visualized, it was classified as a fine phenotype. Conversely, if the marks could not be visualized, it was classified as a coarse phenotype. The width of keratinized gingiva in millimeters was measured with a periodontal probe.
The following variables were the associated factors in the clinical record: braces inserted at the marginal level, malposition or dentomaxillary anomalies, bruxofacets, and premature or supra contacts. The variables of smoking, orthodontic treatment, bruxism, oral piercings, and type of toothbrush were asked for in the questionnaire and considered as self-reports. The variables of inadequate restorations and the presence of bacterial plaque were not analyzed.
Two investigators were calibrated intra- and interoperator to assess the clinical gingival status of the patients. An intraclass correlation higher than 0.75 was obtained. Categorical and ordinal variables were described in frequency and percentage, continuous variables were expressed as averages or medians as a measure of central tendency, and their standard deviations as a measure of dispersion. The distribution of continuous variables was analyzed using the Shapiro-Wilk test.
The total prevalence was described with their respective 95% confidence intervals. The association between categorical variables was analyzed with the Chi-square test. Student’s t-test or Mann-Whitney test analyzed the difference in means between continuous variables and the prevalence of recessions. Risk was evaluated using logistic and linear regression models according to the description of the dependent variable.
Correlation between continuous variables was determined by Pearson’s or Spearman’s test. A p value < 0.05 was considered statistically significant. All data were analyzed in STATA 14.0.
The study was approved by the Scientific Ethics Committee of the Universidad de Los Andes and authorized by the Centro de Salud San Bernardo to perform the measurements. The procedures were performed in accordance with the principles of the Declaration of Helsinki, and there were no competing interests among the participants. The students were not coerced in case they decided not to participate. On the contrary, the participants benefited from receiving an early diagnosis of gingival recessions without potential risks.
Results
A total of 311 students were examined, and 93.56% had at least one gingival recession. The demographic parameters and the distribution of associated factors are shown in Table 1.
When we looked at the distribution of recessions by age, the median was the same for both groups. The median for the group without recessions was 22.25 years, with an interquartile range of 1.86, and 22.62 years for the group with recessions, with an interquartile range of 2.12. On the other hand, when analyzing the number of recessions in both genders, we observed a median of four recessions for the women and six for the men (Figure 1).
Association between frequency of gingival recessions and gender.

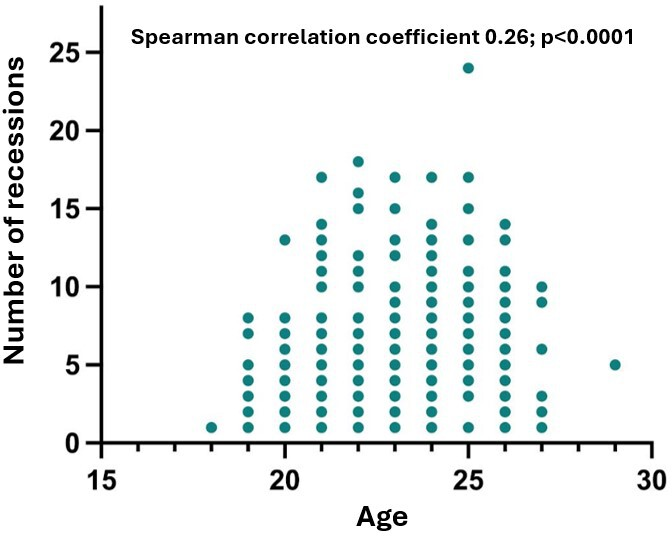
On the other hand, the correlation between age and the number of gingival recessions was analyzed using Spearman’s correlation test, and a correlation was found (P value < 0.001). Furthermore, the degree of correlation for both variables resulted in a Rho of 0.26, indicating a low correlation (Figure 2).
Association between the number of gingival recessions and age.
When analyzing the distribution of recessions by arch, 85.2 % of the individuals had at least one recession in the mandible, while in the maxilla recessions were present in 79.4% of the patients. Of the total recessions, 1021 (59%) were in lower teeth and 710 (41%) in upper teeth. According to the location, recessions in upper teeth had a median of 2 with an interquartile range of 2 and lower gingival recessions had a median of 3 with an interquartile range of 4.
When analyzing the distribution of recessions by arch, 85.2 % of the individuals had at least one recession in the mandible, while in the maxilla, recessions were present in 79.4% of the patients. Of the total recessions, 1021 (59%) were in lower teeth and 710 (41%) in upper teeth. According to the location, recessions in upper teeth had a median of 2 with an interquartile range of 2, and lower gingival recessions had a median of 3 with an interquartile range of 4.
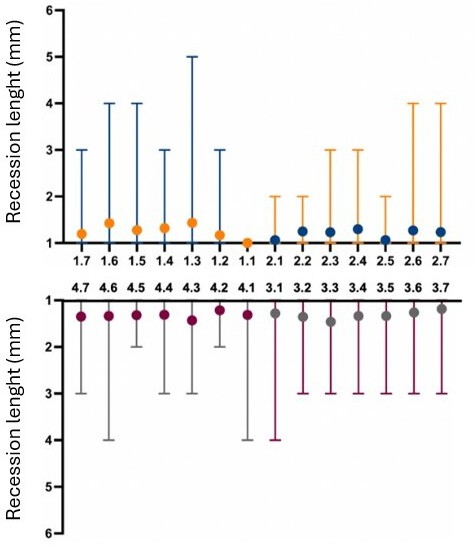
The average millimeters of teeth recessions was 1.3. The deepest recessions were observed in the canines. Teeth 3.3 had an average of 1.46 millimeters, followed by teeth 4.3 and 1.3, which had 1.43 millimeters. The least severe tooth was tooth 1.1, which had an average of 1 millimeter (Figures 3 and 4).
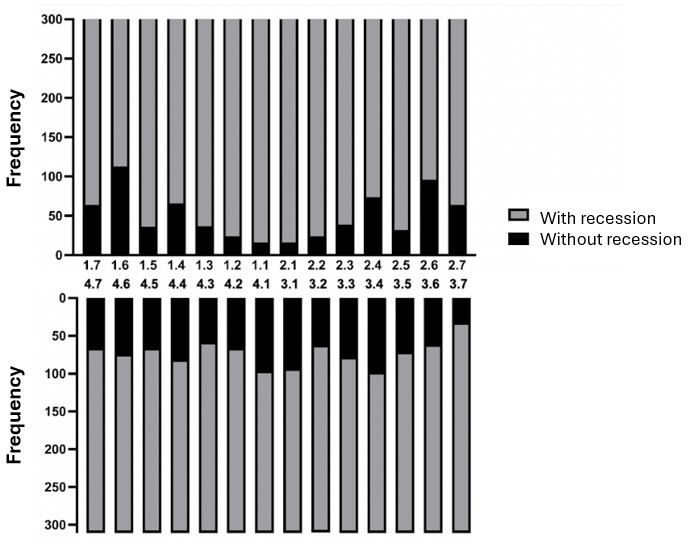
Frequency of gingival recession by tooth.
Severity of gingival recessions by tooth.
The teeth with the highest prevalence of gingival recessions were 1.6 with 113 recessions (36.3%), followed by teeth 3.4 with 98 (31.5%), 2.6 with 96 (30.9%), and 4.1 with 96 (30.9%). The tooth with the lowest prevalence was 1.1, with 5.1% (Figure 4).
Of the total, 122 students (39.2%) recorded gingival recessions exclusively 1 millimeter in length, while 169 (54.3%) presented recessions greater than or equal to 2 millimeters. The largest recession recorded was a single case of 5 millimeters (0.3%).
If we analyze the number of gingival recessions by academic year, the prevalence was over 90%. In the first year, it was 91.67%; in the second year, 91.43%; in the third year, 96%; in the fourth year, 91.07%; and in the fifth year, 93.22%, with the last year having the highest prevalence of 96.83%.
Of the 311 students evaluated, 75.24% had a history of orthodontic treatment, of which 95.3% had a gingival recession in the mouth.
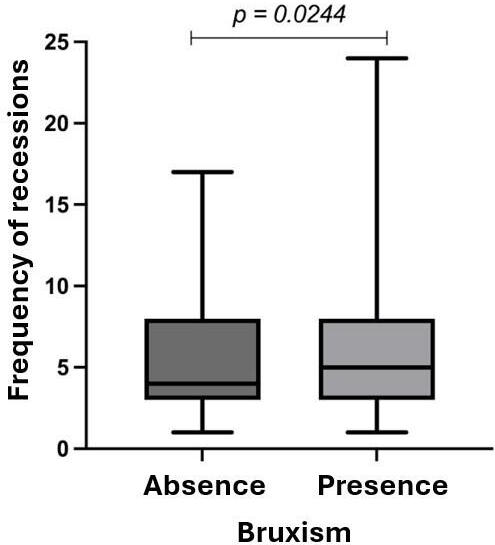
The number of gingival recessions in students with a history of bruxism was higher compared to those without this condition. The prevalence was 60.7% (Figure 5).
Association between bruxism and frequency of gingival recessions.
When comparing smokers and nonsmokers, no statistically significant differences were found regarding prevalence or number of gingival recessions in the mouth.
No statistically significant differences were found between smokers and nonsmokers regarding the prevalence or number of gingival recessions in the mouth.
Patients who presented with a gingival recession and had associated bruxofacets were more likely to have a gingival recession.
On the other hand, the presence of marginal insertion frenulae was detected in 5.7% of the examined students.
Regarding the gingival phenotype, the fine biotype was more prevalent. However, a higher prevalence of gingival recession was found among students with coarse phenotype.
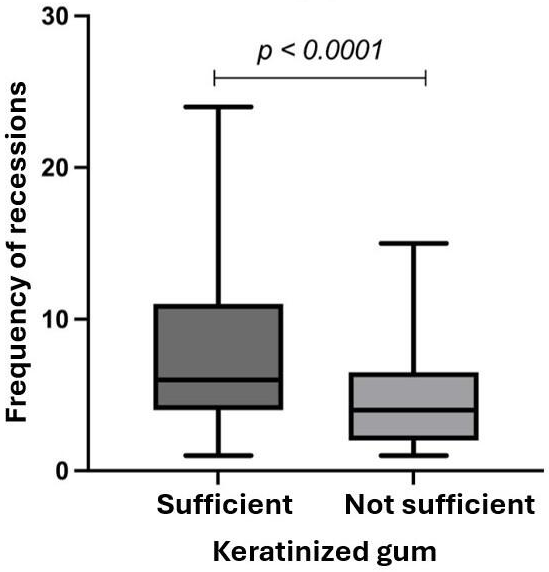
Students with insufficient keratinized gingiva (less than 2 millimeters) had more gingival recessions than those with sufficiency (Figure 6).
Association between sufficiency of keratinized gingiva and frequency of gingival recessions.
Finally, the soft brush was the most used in the sample and showed a positive association compared to the medium-hard brush students. Gingival recessions were more prevalent among students who brushed with soft bristles.
Discussion
When comparing the results of this study with those available in the literature, it is possible to conclude that the prevalence of gingival recession among dental students at the Universidad de Los Andes was indeed higher than in other populations. The observed prevalence of gingival recession of 93.56% in the students correlates with that reported by Kasaj, who informed a worldwide prevalence ranging from 50 to 100%
[10]. These results are similar to those of Castro-Rodriguez [11] who reported 94.3% of individuals with gingival recessions in a population between 25 and 75 years. Furthermore, it was higher than that reported by Chrysanthaopolus in the same age group (but not among dental students), only evidencing its presence in 63.9% of the studied individuals [4].
Comparing the results of this study with data obtained in Latin America, we can see that in Brazil, in a population of 1460 adults, the prevalence was 83.4%, indicating that the prevalence was directly proportional to the age of the individual observed [12]. In Ecuador, in a sample of 361 patients seen in a dental center, the prevalence of gingival recessions was 94.46%, similar to our study [13]. Another study by Rivera-Valerio et al. on Peruvian students showed a prevalence of 85.71% in 77 students [6].
It is worth noting the difference found when compared with Vignoletti's results, who, in an Italian population of 251 dental students, obtained a prevalence of only 39% among patients [14].
In the present study, the distribution of recessions was 59% in the mandible and 41% in the maxilla. Although the arch type was not a significant variable for developing gingival recessions, this is contrary to what was reported by Vignoletti, who showed a significantly higher prevalence in the maxilla (60%) versus the mandible (40%). Likewise, in that study, it was observed that the teeth with the highest prevalence were the first premolars with 23%, followed by the first molars with 20%, while in ours, the most affected was the 1.6 with 36%, followed by the 3.4 with 31% [14].
As in the previous study, age was associated to the presence of gingival recessions in our investigation. Furthermore, in Vignoletti’s work the insufficient amount of keratinized gingiva was found to be linked to the severity of gingival recessions (t = -4.19; 95% CI; -0.19 to -0.07), whereas in our study it correlated with the amount of gingival recessions at the patient level. This was higher among students with insufficient keratinized gingiva (less than 2 millimeters).
As in the previous study, age was associated with gingival recessions in our investigation. Furthermore, in Vignoletti’s work, the insufficient amount of keratinized gingiva was found to be linked to the severity of gingival recessions (t = -4.19; 95% CI; -0.19 to -0.07), whereas in our study, it correlated with the number of gingival recessions at the patient level. This was higher among students with insufficient keratinized gingiva (less than 2 millimeters).
Students who self-reported bruxism showed a higher prevalence of gingival recessions (95.8%) than those who did not report it (90.2%), with no significant differences. On the other hand, students with a history of orthodontics showed a prevalence of 95.73% gingival recessions, compared with 88.3% who did not have this history, registering a statistically significant value.
According to Shah [15], the ratio between the prevalence of thin and thick periodontal phenotypes was 43.3% and 56.7%, respectively. In the present study, the prevalence of fine phenotype was higher, with a ratio of 69 and 31%.
The 94.4% of the subjects with coarse phenotype (determined by Rouk’s method) presented recessions versus 93.1% of the individuals with fine phenotype. In this case, there were no significant differences between the two groups. Nevertheless, it is possible to speculate that the phenotype would be a determining factor in the long term, with little relevance among young populations [16,17].
Müller et al.'s study mentions that there was no significant difference between the prevalence of gingival recession among smokers and nonsmokers [18], and this study can support this assertion. Considering that the sample is young, it is possible to conjecture that smoking has not acted long enough to be an important factor.
We can show a different result from the literature based on what was discussed in this work. This is because the prevalence of gingival recession described for the 20 to 29 age group was 73.9% and 63.9%, compared to 93.6% in this study [4,11].
Regarding the limitations of the study, on the one hand, the factors associated with healthy teeth were not evaluated in order to compare their relationship with the affected teeth. This means that the association factors were analyzed only when recession was present. In addition, we did not specify which vestibular surface presented the recession, as it could be found in the mesial, medial or distal area.
Regarding the study's limitations, on the one hand, the factors associated with healthy teeth were not evaluated to compare their relationship with the affected teeth. This means that the association factors were analyzed only when recession was present. In addition, we did not specify which vestibular surface presented the recession, as it could be found in the mesial, medial, or distal area.
The time of orthodontic treatment, the amount of orthodontic sessions, the years of smoking, and the amount of time the patient had a history of bruxism were not taken into account.
Likewise, external factors such as orthognathic surgeries were not considered. It is worth mentioning that no information was collected on the frequency or duration of brushing. Finally, these results cannot be extrapolated to all age groups.
Conclusions
Vestibular gingival recessions reached 93.6% of all dental students at the Universidad de Los Andes in Chile. The most prominent factor in the prevalence of gingival recessions was the history of orthodontics and, to a lesser extent, age. Consequently, clinical surveillance in patients undergoing orthodontic treatment is highly recommended to detect, and thus prevent, the appearance of gingival recessions.
Vestibular gingival recessions reached 93.6% of all dental students at the Universidad de Los Andes in Chile. The most prominent factor in the prevalence of gingival recessions was the history of orthodontics and, to a lesser extent, age. Consequently, clinical surveillance in patients undergoing orthodontic treatment is highly recommended to detect and thus prevent the appearance of gingival recessions.
However, longitudinal studies are needed to verify cause-effect associations, considering the predisposing factors for gingival recession we found in this study.
