Estudios originales
← vista completaPublicado el 25 de marzo de 2025 | http://doi.org/10.5867/medwave.2025.02.2915
Factores asociados a la calidad de vida relacionada con la salud en pacientes en hemodiálisis de un hospital peruano: estudio transversal
Factors associated with health-related quality of life in hemodialysis patients in a Peruvian hospital: A cross-sectional study
Abstract
Introduction Health-related quality of life in patients undergoing chronic hemodialysis has become a fundamental criterion for evaluating the effectiveness of treatments, promoting the overall well-being of this population. The study aims to identify the factors associated with health-related quality of life in patients with chronic kidney disease undergoing hemodialysis in Huancayo, Peru, from September to November 2022.
Methods Observational, descriptive, single-center, cross-sectional study in which sociodemographic data associated with health-related quality of life in hemodialysis patients were identified using the SF-36 instrument.
Results The SF-36 questionnaire on health-related quality of life (HRQoL) was administered to 88 hemodialysis patients, of whom 68.2% were men, and 87.5% were undergoing outpatient dialysis. The main cause of chronic kidney disease was hypertension, affecting 46.6% of participants. Additionally, 80.7% had been on hemodialysis treatment for less than five years. In the bivariate analysis, significant differences were observed in the vitality dimension concerning educational level (p = 0.011) and sex (p = 0.049). Likewise, there was a significant difference between the average values of the emotional role dimension (p = 0.038) of the SF-36 in the nutritional status levels and a significant difference between the average total scores of the SF-36 in the salary levels (p = 0.048). The multivariate analysis identified correlations between nutritional status and pain; educational level and vitality; nutritional status and physical role; economic income; educational level and social function; and nutritional status and emotional role.
Conclusions Patients on hemodialysis have a total health-related quality of life score ranging from low to moderate (90.8%). The factors associated with a lower quality of life are being male, poor nutrition, low educational level, and a poor emotional state. Early identification of these factors will allow the development of interventions to improve these patients' quality of life. It is crucial to design interventions focused on improving nutrition and preventing mental health disorders, paying special attention to men with low educational levels.
Main messages
- Health-related quality of life in patients undergoing chronic hemodialysis is a complex issue that encompasses multiple dimensions, including physical, emotional, social, and psychological aspects.
- This work details elements that would improve the clinical management of patients on dialysis, adopt a comprehensive approach to people with chronic kidney disease, and provide them with information about the factors that impact their quality of life.
- One limitation of the study is that it only included patients undergoing hemodialysis treatment at the Ramiro Prialé Prialé National Hospital in the Huancayo region of Junín, Peru.
Introduction
Chronic kidney disease is considered a global public health problem [1]. It is estimated that more than 850 million people worldwide are affected by kidney disease, the majority of whom suffer from chronic kidney disease. The estimated global prevalence of chronic kidney disease is 8 to 16% [2]. Data from the Global Burden of Disease (GBD) reveal a significant increase in the incidence of this disease, from 11 million to 21 million cases (89%), and an increase in its prevalence from 147 million to 275 million cases (87%) in 26 years [3]. Although there are no national prevalence studies on chronic kidney disease in Peru, research on specific population groups shows that 18% of the Peruvian population with this pathology requires renal replacement therapy as their primary treatment [4]. According to data from the Global Burden of Disease, chronic kidney disease will cause 5.28% of total deaths in Peru by 2024 [5]. Furthermore, only 30% of Peruvians have access to renal replacement therapy [6]. Similarly, the National Center for Epidemiology, Prevention and Disease Control of Peru (CDC-Peru) reports that between 73% and 89% of patients start dialysis unplanned, in an emergency context, evidencing a lack of timely management and higher cost of care [7]. In cities outside the capital of Peru, the availability of hemodialysis centers is limited, forcing patients needing dialysis treatment to travel urgently for an average of 2 to 6 hours [8].
Hemodialysis is a renal replacement therapy that consists of an extracorporeal circuit made up of a filter (dialyzer) and a system of lines (arterial and venous) for transporting blood and dialysate in countercurrent (dialysis solution). The therapy aims to restore homeostasis of the extracellular and intracellular fluids [9].
In 1994, the World Health Organization (WHO) defined health-related quality of life as “an individual’s perception of physical and mental health over time, in the context of the environment in which he or she lives, taking into account their personal goals, expectations, values, and interests” [10]. However, as it is a chronic disorder, the most appropriate concept to define health-related quality of life is described as the subjective evaluation of how current health status, healthcare and health promotion influence the individual’s ability to achieve and maintain an overall degree of functioning that allows them to carry out activities that are important to them and that impact on their general well-being [11]. As this is a very subjective definition, instruments have been developed to measure health-related quality of life and obtain more objective results based on its multidimensional components. The concept of health-related quality of life is made up of different situations in which the patient sees a specific dimensions altered, such as physical functioning, psychological well-being, emotional state, pain, social functioning, general perception of health, the degree of satisfaction with life, the impact on work productivity and daily life activities [12].
The health-related quality of life of people undergoing hemodialysis encompasses physiological, psychological, economic, and social aspects. According to Huaynate et al., higher hemoglobin levels are associated with an improvement in the score for the emotional role dimension, according to the Kidney Disease Quality of Life (KDQOL) questionnaire designed for patients with kidney disease [13]. Furthermore, treatment adherence has a positive influence, since “lack of adherence seems to increase the perception of feeling healthy among patients and reinforces the control that the individual has over their illness and treatment, which can have an impact on emotional and physical aspects” [12].
It is crucial to investigate the factors associated with health-related quality of life in patients with chronic kidney disease undergoing hemodialysis in the Peruvian highlands. This will improve the clinical management of dialysis patients, adopt a comprehensive approach towards people with chronic kidney disease and provide them with information about the factors that impact their quality of life. Furthermore, it will facilitate the evaluation of clinical interventions from the patient’s perspective. The study’s objective is to identify the factors associated with health-related quality of life in patients with chronic kidney disease on hemodialysis treatment in Huancayo, Peru, from September to November 2022. Specifically, the aim is to determine the psychological and socioeconomic factors associated with health-related quality of life in patients with chronic kidney disease on hemodialysis. We hypothesize that there are psychological and socioeconomic factors and lifestyle choices linked to quality of life in patients with chronic kidney disease on hemodialysis.
Methods
Study design and sources of data
A descriptive, observational and cross-sectional study was carried out, using data provided by hemodialysis patients in Huancayo, Peru from September to November 2022. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for observational studies were followed for the report of this study [14].
Population and sampling
The study population consisted of patients diagnosed with chronic kidney disease who underwent hemodialysis at the Nephrology Unit of the Ramiro Prialé National Hospital for three months in 2022. A total of 125 patients were counted, of which 88 were finally enrolled. This size would be sufficient to detect a minimum difference of between 9 and 10 points in health-related quality of life between equal groups with an approximate power of 80% and an α value of 5% when the standard deviations are around 15 points (OpenEpi: Open Source Epidemiologic Statistics for Public Health, Version.
Selection criteria
For the present study, the following inclusion criteria were established: patients with a confirmed diagnosis of chronic kidney disease on hemodialysis, who are physically independent, over 18 years of age, and who agreed to participate by signing the informed consent form. Thirty-seven patients were excluded due to hearing impairments or difficulties in completing the questionnaire, as well as serious pathologies that had decompensated three months before the personalized interview (Figure 1).
Flow chart of the patients in the study.
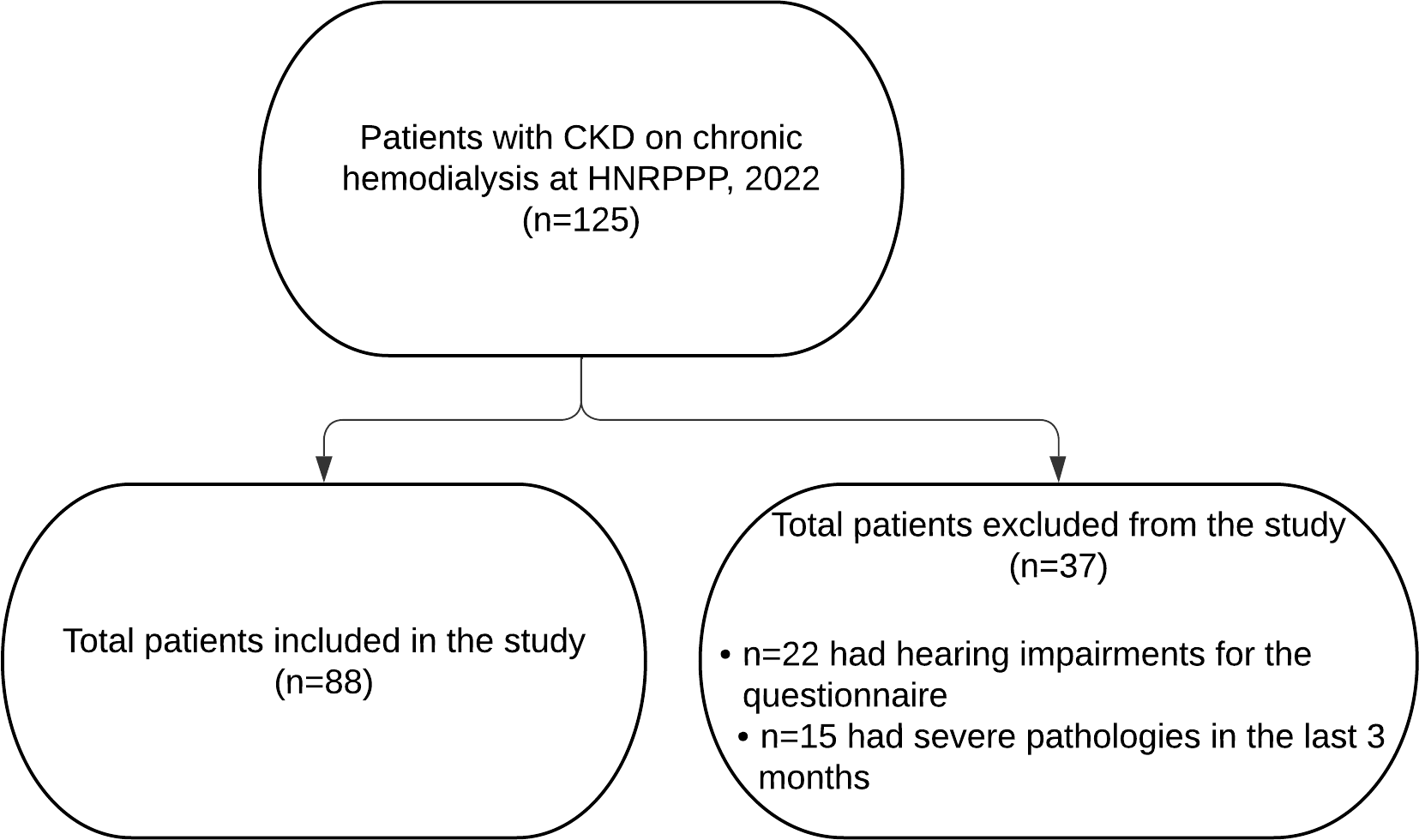
HNRPP: Hospital Nacional Ramiro Prialé Prialé.
Source: Prepared by the authors based on the study data.
After obtaining the approval of the study’s ethics committee, permission was requested from the hospital authorities for data collection. Before sampling, the purpose of the study was explained to patients attending their renal replacement therapy, leaving the option to participate in the survey to their choice. They were also described the content of the questionnaire by the lead investigator during a face-to-face session lasting approximately 45 minutes. During this session, detailed instructions were given on the correct administration of the questionnaire, appropriate interaction with participants to answer questions and the study presentation to obtain informed consent.
Data collection was carried out in person at the hemodialysis unit of the Ramiro Prialé Prialé National Hospital. The authors took on the role of surveyors, being external to the clinical team that attends to hemodialysis patients. Using the documentary technique, a survey was applied to address a form for collecting relevant information and sociodemographic data, as well as the SF-36 questionnaire, through the PAPI technique (Paper And Pencil Interviewing) [15].
Before patients were recruited, a pilot test was carried out in another national hospital with a hemodialysis unit. This center did not participate in the final study because it belongs to a different healthcare system. In the pilot test, areas for improvement were identified based on the participants' recommendations, which allowed adjustments to be made to the final instrument.
The survey was administered to patients upon arrival at the hemodialysis unit, regardless of whether ambulatory or hospitalized for non-renal reasons. The survey was conducted during the hemodialysis session, in compliance with all established biosafety measures. The estimated time to complete the survey was 20 to 25 minutes.
Once the information had been collected from the patients, the authors entered it into a Microsoft Excel database in preparation for the subsequent stages of analysis. In the event of any inconsistencies in the data, a second author reviewed the original surveys to ensure the accuracy of the information.
Instruments and variables
The first page of the printed survey presented to the participants contained the informed consent form, which detailed aspects of the research and the importance of their contribution in answering the survey.
The questionnaire consisted of six sections that collected various variables. The dependent variable was health-related quality of life, while the independent variables included psychological and socioeconomic determinants, which are detailed below:
It included sociodemographic data and a data collection form that described age (in years), biological sex (female or male), the type of dialysis facility (inpatient or outpatient), the cause of kidney disease, and the years of hemodialysis treatment.
Economic salaries (less than the minimum living wage, the minimum living wage or more than the minimum living wage), employment status (self-employed, employed or unemployed) and educational level (primary, secondary or higher) were recorded.
Hours of sleep (less than or more than six) were assessed.
In addition, the following instruments were used:
Trait-State Depression Inventory (TSDI)
This self-assessment inventory is designed to estimate two relatively independent forms of depression: depression as a state (transitory emotional condition) and depression as a trait (propensity to suffer depressive states). It consists of 20 items in which the respondent must indicate the option that best describes their situation, with four response options: “Not at all” (1 point), “A little” (2 points), “Quite a bit” (3 points) and “A lot” (4 points). This instrument allows the levels of depression-trait to be classified as low, medium, or high. The score is obtained by adding the scores of the direct and inverse items, to which the value 50 is added to ensure that all the values are positive. The scores range from 20 to 80 points for the state scale; and 22 to 88 points for the trait scale [16].
This mini-scale is designed to screen malnutrition in patients on chronic dialysis and consists of seven items. According to the score obtained, patients are classified as malnourished (0 to 7 points), at risk of malnutrition (8 to 11 points) or with a normal nutritional status (12 to 14 points) [17,18].
SF-36
This questionnaire evaluates health-related quality of life based on eight dimensions (physical function, physical role, bodily pain, general health, vitality, social function, emotional role and mental health) and 36 items. It evaluates both positive and negative states of quality of life related to physical and psychological health. The metric characteristics include different scoring scales, where a higher value indicates a better quality of life. The variables were categorized as low (less than 25 points), moderate (between 25 and 75 points) and high (more than 75 points) [19].
The “health-related quality of life” variable was studied with the SF-36 and validated for Spanish and Peru [19]. The depression dimension was evaluated using Martín’s IDERE [16], while the eating dimension was analyzed with the MNA® SF [17]. Socioeconomic status was compiled using a data collection form designed by the authors, which was classified according to salary amount and categorized to facilitate grouping. Cronbach’s α coefficient was calculated for the total SF-36 score and a value of 0.82 was obtained. For the dimensions, Cronbach’s α was between 0.66 and 0.92, indicating good internal consistency for the questionnaire applied.
Statistical analysis
The data were tabulated in Microsoft Excel and processed in STATA version 17. A descriptive analysis of the categorical variables was carried out using frequencies and percentages, while the numerical variables were described using measures of central tendency and dispersion. The Kolmogórov-Smirnov normality test (p < 0.05) was carried out for the total SF-36 values and dimensions. In all cases, the normal hypothesis was rejected. Therefore, comparisons between groups given by independent variables were made using non-parametric tests. A bivariate analysis was performed to compare the distributions of the SF-36 dimensions between the groups defined by categorical variables such as sex, educational level and nutritional status, using the Mann-Whitney U test for two groups and the Kruskal-Wallis test for more than two groups. Finally, a multiple linear regression model was used to identify the factors independently associated with the SF-36 dimensions.
Ethics
The research was approved by the Institutional Committee for Research Ethics of the Universidad Continental and the Junín Healthcare Network of the Social Security Organization EsSalud (Certificate No. 28-CIEI-GRAJ-ESSALUD-2022). Participation in the study was voluntary, and all participants signed an informed consent form beforehand. To ensure privacy and confidentiality, all data collected was anonymized and coded, allowing for detailed analysis and processing without putting the participants' identities at risk. This data was stored securely and was only available to the authorized research team. Furthermore, the research complied with the ethical principles of autonomy, beneficence, and justice, guaranteeing responsible and ethical handling of sensitive information.
Results
Of the 88 respondents, 60 (68.2%) were men and 28 (31.8%) were women. The average age was 63.5 years, with a standard deviation of 9.32. The main causes of chronic kidney disease were high blood pressure, which affected 41 patients (46.6%), followed by diabetes mellitus with 30 patients (34.1%), obstructive uropathy with four patients (4.5%) and non-affiliated causes with six patients (6.8%). Regarding the duration of hemodialysis treatment, 71 patients (80.7%) had been on hemodialysis for less than 5 years, 13 patients (14.8%) for 6 to 10 years, and four patients (4.5%) had been on treatment for 11 to 15 years (Table 1).
Table 2 shows the factors studied in relation to the measured results indicating health-related quality of life, using the non-parametric Mann-Whitney U or Kruskal-Wallis tests. Regarding the vitality outcome, a statistically significant difference was observed between groups stratified by sex (p = 0.049) and educational level (p = 0.01). When evaluating the emotional role outcome, a significant difference was found between groups based on nutritional status (p = 0.038). However, no other significant differences were identified between groups based on the remaining independent variables concerning the total SF-36 scores or its dimensions.
Due to the study’s characteristics and the multiple variable interactions, it was decided to include all the independent variables in the multivariate model. The regression resulting from the multivariate analysis is shown in Table 3. When analyzing the groups that previously showed statistical differences, it was observed that when analyzing the vitality outcome by educational level, patients with secondary education are estimated to have 17.3 points less vitality on average than those with primary education or less. No significant statistical difference between sexes was obtained in the multivariate analysis. Regarding the emotional role by nutritional status, patients with a normal nutritional status are estimated to have an average of 37.1 points more in the emotional role than patients suffering from malnutrition. Other variables that showed statistical significance (p < 0.05) in the multivariate analysis were pain and the physical role by nutritional status. It was also identified that patients at risk of malnutrition had an estimated average difference of 16.8 points more in the pain dimension than those suffering from malnutrition, and it is estimated that patients with normal nutritional status have 26.5 points less on average in the physical role than patients with malnutrition. It is important to emphasize that these last two results did not show statistical significance in the bivariate analysis. This value could change if more subjects are included in the study.
Discussion
Several studies, such as those carried out in Brazil and in the countries of the PDOPPS (Peritoneal Dialysis Outcomes and Practice Patterns Study) group, which includes Australia, Canada, Japan, the United Kingdom and the United States, show that women on renal replacement therapy have a lower health-related quality of life than men. This could be because women bear a more significant social burden than men, assuming more responsibilities within their social circle. This social burden is aggravated with age, as subsequent generations depend on them for care. This phenomenon is observed in patients on renal replacement therapy and the general population [20,21,22]. In Peru, specifically in Ica, Gadea and Campos describe that hemodialysis patients obtained scores ranging from fair to low in functional status of health-related quality of life and physical, social and emotional dimensions [23]. However, they do not describe gender differentiation. Recent research has shown that being male positively influences health-related quality of life and care in hemodialysis, so men generally have a better quality of life than women [22,24]. However, the present research does not present the same scenario, since no statistical correlation was found between sex and the SF-36 dimensions.
9.1% of patients are economically independent, while the rest are dependent or unemployed. This result is probably due to the fact that chronic kidney disease is a disabling condition that limits the functional capacity and quality of life of patients, in addition to causing them to lose years of productive life [25].
The leading cause of chronic kidney disease in this study was high blood pressure in 46% of patients, a finding also found in another study conducted in Huancayo [26], followed by diabetes with 34.1%. This latter pathology is probably associated with physiological factors related to altitude, since insulin is more effective at high altitudes and there is a tendency towards hypoglycemia. For this reason, diabetic patients are advised to reduce their insulin dose when traveling to high altitudes, to avoid the possible risk of hypoglycemia [26,27].
An important finding in the present study is that 80.7% of the patients have been on hemodialysis for less than 5 years, 14.8% between 6 and 10 years, and only 4.5% for more than 10 years. This can be explained by the high risk of mortality in this type of patient. Studies in Spain and the United States indicate that five-year survival is 42% [28,29].
The present study found that hemodialysis patients have an average total SF-36 score of between 45 and 52 points, indicating a fair health-related quality of life. In addition, it was observed that the lowest categories are general health, emotional role, and physical role, with averages of 43.5, 42.0, and 25.7, respectively. Other studies support these findings, pointing out that the physical role is the most impaired dimension, as these patients perceive that their physical health interferes with their daily activities, reduces their performance and limits their ability to perform other activities [30].
The educational level is significantly associated with vitality in both bivariate and multivariate analyses. This observation coincides with the findings of Ebrahimi et al., who mention the positive impact of education on the health-related quality of life of patients on dialysis [31]. In addition, several studies have found a negative correlation between low education, lower income and unfavorable socioeconomic conditions, factors that can negatively affect adherence to treatment and understanding of it [32,33].
A statistically significant association was found between nutritional status and the dimension of the emotional role. This observation is supported by previous studies carried out by Cepeda et al. in the Dominican Republic [34], Yixin et al. in China [35] and Visiedo et al. in Spain [36], among others. These studies indicate that patients with a normal nutritional status tend to improve their emotional role, which could contribute to better functionality in those undergoing hemodialysis [37].
A relationship was established between hours of sleep and emotional role, as adequate sleep quality is a determining factor for health and an essential component for a good health-related quality of life. This is not limited to just sleeping well at night, but also involves functioning well during the day. It was found that sleep disturbances can have a direct impact on patients' mental health, causing symptoms of depression or anxiety, which in turn can affect the emotional role [38]. On the other hand, Ynga Hidalgo emphasizes that hemodialysis patients face various sources of stress that cause unpleasant symptoms, both due to the disease and the treatment, which weakens the perception of their health-related quality of life, showing a low average health-related quality of life [39], results that are similar to this study. For this reason, adjuvant non-pharmacological therapy, such as cognitive-behavioral therapy, relaxation techniques, and regular exercise [40,41,42], is suggested to improve health-related quality of life in hemodialysis patients.
Marín López carried out a study in Spain that revealed that the health-related quality of life of hemodialysis patients is mainly influenced by factors such as depression, activity, age, and comorbidities. Consequently, interventions aimed at improving health-related quality of life in patients with advanced chronic kidney disease should promote physical activity and pay attention to patients' mental health [43].
It is important to note that among this study’s limitations, the small sample size is a key factor, along with the potential omission of other relevant variables, such as psychological factors (e.g., anxiety, depression) or those related to renal treatment. Therefore, further research is recommended, utilizing adjusted models to validate and expand upon these findings. In the bivariate analysis, some associations did not reach statistical significance; however, in the multivariate model, these relationships became statistically significant when controlling for additional variables.
Similarly, the small sample size could also limit the generalizability of the findings. In addition, the lack of normality of the variables could have affected the interpretation of the results.
One of the main challenges in this study was the use of multiple regression, which does not follow a normal distribution. For future work, it would be advisable to explore alternative statistical models or perform transformations on the variables.
Conclusions
The present research shows significant findings on health-related quality of life in patients undergoing hemodialysis, who generally have a total health-related quality of life score ranging from low to moderate.
We identified factors in these patients negatively associated with health-related quality of life, such as being male, low educational level, malnutrition, and poor emotional state.
These results are useful for designing health interventions and policies that improve the quality of life of hemodialysis patients.
