Estudios originales
← vista completaPublicado el 8 de mayo de 2025 | http://doi.org/10.5867/medwave.2025.04.3010
Efectos de nuevos programas de ejercicio multicomponente sobre los niveles del factor neurotrófico derivado del cerebro y la aptitud física en mujeres mayores
Effects of novel multicomponent exercise programs on brain-derived neurotrophic factor levels and physical fitness in older women
Abstract
Introduction Multicomponent exercise programs have demonstrated benefits for both cognitive and physical function. However, their effects on brain-derived neurotrophic factor (BDNF) levels remain inconsistent, particularly in protocols incorporating functional exercises. This study aimed to evaluate the impact of two distinct multicomponent exercise protocols on BDNF levels and physical fitness in older women.
Methods Ninety physically active. community-dwelling older women (70.4 ± 7.2 years) were allocated to three different groups: 1) Multicomponent program 1: Circuit-based functional training; 2) Multicomponent program 2: Pilates Method; and 3) control group that received only health education. Both multicomponent programs were conducted over a 12-week period, with 50-minute sessions held three times per week. The control group participated in 12-week Health Education intervention with 90-minute sessions once a week. Brain-derived neurotrophic factor levels, short physical performance battery, agility, six-minute walk, and handgrip tests were measured.
Results Brain-derived neurotrophic factor levels increased significantly in both the functional training group (p<0.001) and Pilates group (p=0.005), with a more pronounced increase observed in the functional training group. The distance covered in the six-minute walk test also increased significantly in the functional training group (p=0.001) and was greater compared to both the Pilates (p<0.001) and control (p<0.001) groups.
Conclusions Both multicomponent exercise programs led to increased BDNF levels after 12-week intervention. However, functional training yielded superior results compared to the Pilates method, possibly mediated by improvement in physical function.
Main messages
- To date, no studies have investigated the effects of different multicomponent exercise programs on BDNF levels in older adults.
- Both functional training and Pilates significantly increased BDNF levels; however, functional training resulted in a more pronounced increase.
- The multicomponent exercise program that included functional activities led to significant improvements in physical function.
Introduction
Maintenance of fitness and cognitive functions has been identified as one of the main factors for healthy aging [1]. Exercise is known for reducing the deleterious effects of aging and maintaining and improving physical and cognitive function in older adults [2]. In this population, different types of physical exercise programs have shown improving in muscle strength, mobility, agility, gait speed, cardiorespiratory fitness and preserving cognitive [3,4,5]. Despite previous investigations into the effects of exercise programs on fitness and cognitive function, significant discrepancies persist regarding the specific types of exercises, modalities, intensities, and whether incorporating functional tasks into exercise programs could yield additional benefits on physical and cognitive markers.
In the context of physical exercise and cognitive function. the brain-derived neurotrophic factor (BDNF), an important neurotrophin related to survival and plasticity of neurons, has been widely studied. Reductions in peripheral BDNF levels may be important biomarkers related to depression [6] and mild cognitive impairment (MCI) [7] , the latter being considered a risk factor for Alzheimer’s Disease. Recent evidence indicated that physical exercise stimulates metabolic pathways capable of regulating the expression of peripheral BDNF [8,9]. However, there are still divergences regarding the type of exercise program that presents the most promising results. For instance, Dinoff et al. [10] showed a significant increment of BDNF levels in aerobic interventions, but not in resistance training. On the other hand, a meta-analysis study showed that strength training and combined training (aerobic and strength) had a positive effect on peripheral BDNF concentrations in older adults, while isolated aerobic training did not induce the same response [11]. Most systematic reviews about the effect of physical exercise on BDNF in older population, have shown that most clinical trials have mainly evaluated the benefits of aerobic and/or strength training [11,12,13,14]. Only one systematic review [14] examined the effects of multicomponent exercise on BDNF levels, including three clinical trials with controversial results [15,16,17].
Multicomponent exercise programs are those in which aerobic and resistance training are combined with other physical abilities (e.g. balance, flexibility, motor coordination, etc.) including or not functional tasks. Functional exercise programs have emerged as a new modality of multicomponent exercise programs, emphasizing functional tasks tailored to various physical abilities [18]. In older adults, this modality has demonstrated benefits in cognitive and physical function, particularly when incorporating dual-task activities. Given that dual-task activities are commonly performed in the daily living, training in such activities could lead to functional improvement and stimulate cerebral areas associated with learning in older adults [19,20]. Although this exercise modality has been shown to improve the cognitive capacity of older adults [21,22,23], there is no evidence about the effect on BDNF levels. We hypothesized that multicomponent exercise protocols would result in significant increases in BDNF levels and physical fitness, with more pronounced improvement observed in participants who engaged in functional exercises incorporating dual-task activities. Therefore, the present study analyzed the effects of two multicomponent exercise protocols on the level of BDNF and physical fitness in physically independent older women. One exercise protocol incorporated functional exercises with dual-task activities, while the other utilized multicomponent exercises based on pilates method.
Methods
Study design
A non-randomized controlled trial registered on the Brazilian Registry of Clinical Trials platform (RBR-2HJJ7G/UTN: U1111-1254-3147). The study included a non-probabilistic or convenience sampling of 90 older women, recruited via social media, social networks and community health care centers from Londrina, Brazil. The Study was approved by the Ethics Committee from the State University of Londrina (UEL) (approval number: 2.788.802). The study followed the principles of the Declaration of Helsinki [24]. The study was conducted between August and November 2018.
Participants
The inclusion criteria were: (1) woman aged 60 years or more; (2) physically independent (capable of performing basic and instrumental activities of daily living without assistance); and (3) no participation in regular physical exercise programs during the last three months. The exclusion criteria comprised diseases and/or conditions that could interfere in the performance of the tests, such as neurological, vestibular, orthopedic, psychiatric, and decompensated respiratory or cardiac diseases. Initially, 166 volunteers signed up to participate, in which 90 met the eligibility criteria and were allocated in one of the groups, according to their proximity to the location where the program took place and the order of enrollment. Blinding of the physiotherapists involved in the treatment groups and the older adults was not possible, given the nature of the interventions. However, assessors involved in the assessment tests and the statistician were blinded to which group the subjects belonged. All participants read and signed an informed consent form.
Outcome measurements
To characterize the sample, sociodemographic data (age, education, and marital status) were collected using a questionnaire developed specifically for this study. The economic level was measured using the procedures proposed by the Brazilian Association of Research Companies (ABEP) which estimates the purchasing power of families and classifies in accordance with the score that ranges from 0 to 100, with 100 being the highest economic level. Anthropometric variables were measured, such as body mass (kg), using a digital scale to the nearest 0.1 kg (Balmak. Class III model. São Paulo. Brazil), height (cm), using a stadiometer to the nearest 0.1 cm and body fat mass percentage and fat-free mass percentage, using bioelectrical impedance (Biodynamics 310TM, Biodynamics Corp. USA). From this information, the body mass index (BMI) was calculated using the ratio between body mass and the square of height.
Cognitive function was assessed using the Montreal Cognitive Assessment (MoCA), validated for the Brazilian population [25]. The MoCA is a simple and independent cognitive screening tool, which accesses different cognitive domains: visuospatial skills, executive functions, naming, memory, attention, abstraction, language, and orientation. The total score ranges from 0 to 30 points.
The Brazilian version of the Geriatric Depression Scale of Yesavage and Sheikh, reduced version, was used to assess depressive symptoms (GDS-15) [26]. The GDS-15 is composed of 15 questions with dichotomous answers (yes and no). The total score ranges from 0 (absence of depressive symptoms) to 15 points (maximum score for depressive symptoms).
To measure BDNF, 10 mL of venous blood were collected from each volunteer by a qualified professional from the local University Hospital. Collections were performed in the morning after an eight-hour fast and volunteers were asked not to exercise on the previous day. Blood samples were centrifuged at 3000 rpm for 10 min and the extracted plasma was stored at -80°C until use. BDNF levels were determined using microspheres multiplex immunofluorimetric assay (ProcartaPlex™ Multiplex Immunoassay, Thermo Fisher Scientific, Waltham, Maryland, USA) for Luminex platform (MAGPIX™, Luminex Corp., Austin, Texas, USA), and the procedures were performed according to the manufacturer’s instructions and their reference values.
The physical fitness of lower limbs was assessed using the Short Physical Performance Battery, composed of three tests: a) standing balance test (side-by-side, semi-tandem, and full tandem positions); b) walking speed on 4-meters, and c) the chair stand. Each test was scored from 0 to 4 points, according to established performance criteria. The full Short Physical Performance Battery is scored from 0 to 12, in which zero indicates the worst physical function, and 12 is the highest level of physical function.
Agility assessment was performed using the battery protocol of the American Alliance for Health, Physical Education, Recreation & Dance, which consists of following a route as quickly as possible. The participant started the test sitting in a chair with armrests. On the command to start, they got up and moved to the right around a cone, returning to the chair and sitting back down, then repeated the route to the left side and returned to sit in the chair. This circuit was consecutively performed twice, without interruption. Two attempts were performed and the shortest time in seconds obtained was considered into the analysis.
The six-minute walk test was performed to assess aerobic endurance, according to the norms of the American Thoracic Society. The test consists of walking as fast as possible (without running) on a hard, flat surface on a linear path 30 meters long, delimited by two cones, for six minutes. Standardized encouragement phrases were used to encourage older women to achieve their best results. Two attempts were performed at intervals of 30 minutes, and the longest distance covered in meters between the two attempts was considered in the analysis.
To measure the maximum isometric strength of the hand and forearm muscles, the handgrip test (HGT) was performed using a hydraulic dynamometer (Saehan®, SH5001, resolution 1 Kg). The test was performed in a sitting position with arms parallel to the trunk, elbows flexed to 90 degrees, and forearm and hand in a neutral position. At the evaluator’s signal, the participant pressed the device as hard as possible for five seconds. Three measurements were taken in each hand, alternately, at one-minute intervals. For the analysis, the best result, independent of the side, was used. During all repetitions, the participants were encouraged to achieve their greatest strength.
Intervention protocols
The Functional Training and Pilates method were performed in the afternoon, three times a week, on alternate days, lasting approximately 50 minutes, totaling 36 sessions, and monitored by professionals and students of Physical Education and Physiotherapy. The Health Education group held one meeting a week of approximately 90 minutes, totaling 12 sessions, and was conducted by a previously trained physical education professional. The characteristics of each intervention modality are presented below.
The functional training consisted of a functional exercise program with motor dual-task training using the Functional Exercise Circuit method [18]. Each session started with a 10-minute warm-up, with running, walking, stretching, and recreation exercises, followed by the Functional Exercise Circuit lasting about 30 minutes. The Functional Exercise Circuit consisted of aerobic, resistance, balance, and coordination exercises applied as functional tasks distributed in 15 stations (for details, see Loyola et al. [27]). Participants remained for one minute at each station and they had to complete the circuit twice. Before the beginning of the intervention, the maximum number of repetitions in one minute was calculated to control the exercise intensity. In the first week, the intensity of 50% of the maximum number of repetitions was defined and gradually increased during the following weeks, reaching the value of 150% of the maximum number of repetitions in the 12th week. Balance exercise stations were not evaluated with repetitions. but by the level of difficulty, and the progression of these tasks was accomplished by reducing stability and increasing complexity (e.g. moving from two legs standing to one leg standing and/or the inclusion of dual tasks). At the end of each session, relaxation activities lasting about 10 minutes were performed.
The Pilates method involves strength, balance, and coordination exercises, following the principles of concentration, control, centering, fluidity, precision, and breathing. The intervention was developed in four cycles of nine classes, where each cycle progressed as follows: 1) familiarization with the Pilates method; 2) basic movements; 3) intermediate movements; and 4) advanced movements. Each session started with 10 minutes of stretching, followed by 10 minutes of strengthening exercises for each of the main body segments: lower limbs, trunk, and upper limbs (totaling 30 minutes), and ended with 10 minutes of stretching and relaxation. All exercises were performed in 1 set of 10 repetitions, with a 1-minute rest interval between exercises, using equipment such as Swiss balls, rubber bands, dumbbells, sticks, shin guards, and balance discs. The complexity of the exercises increased with each cycle and the intensity was controlled using the Borg rating of perceived exertion scale, modified by Foster et al. [28] maintained between 5 and 6 (heavy).
Both interventions were supervised by previously trained professionals and students of Physical Education and Physiotherapy.
The control group participated in a Health Education intervention, carried out through the Active Living Improving Health Program (“VAMOS”) [29], whose goal is to motivate behavior change towards a healthy lifestyle in relation to physical activity and nutrition. At each meeting, one chapter of the specific booklet was discussed, made available free of charge to the participants. The subjects were related to physical activity, healthy eating, how to identify and overcome obstacles, planning and setting goals, and strategies to achieve and maintain positive changes. Although encouragement was given to change behavior, we have not offered a systematic practice of physical exercise to the participants in this group.
Statistical analysis
For data analysis, only participants who had a frequency ≥75% in the interventions were considered. Descriptive data are presented as mean ± standard deviation and 95% confidence intervals. A Generalized Estimating Equations model with link function and appropriate distribution assumptions was used to compare the effect of the intervention between groups, controlled for age, BMI, years of education, depressive symptoms, and MoCA score. The model selected for each variable was based on the lowest value of the Quasi-likelihood under the Independence Model Criterion – QIC. The Generalized Estimating Equations was employed due to their robustness and appropriateness for longitudinal data analysis. Generalized Estimating Equations enables the use of different distributions according to the nature of the data, and it has been demonstrated that Generalized Estimating Equations can achieve greater statistical power in cases with small sample sizes and missing data [30]. The Bonferroni post-hoc was used for pairwise comparisons and Cohen’sd [95% CI] for effect size, considering the effect to be trivial (<0.2), small (0.2 to 0.5), medium (0.5 to 0.8) or large (>0.8) [31]. In addition, the intention-to-treat approach was performed. Missing data in the dependent variable, identified as “missing not at random”, were imputed using mean imputation based on observed values within each group. Analyses were performed using SSPS software (v. 25.0) and statistical significance was established at p<0.05.
Results
Of 90 older women who participated in the study (Functional training = 24; Pilates method = 25 and Control group = 41), 73 had a frequency ≥75% in the interventions (Figure 1). The descriptive data of participants are shown in Table 1. There were no significant differences between groups regarding the baseline characteristics.
Flowchart sample distribution.
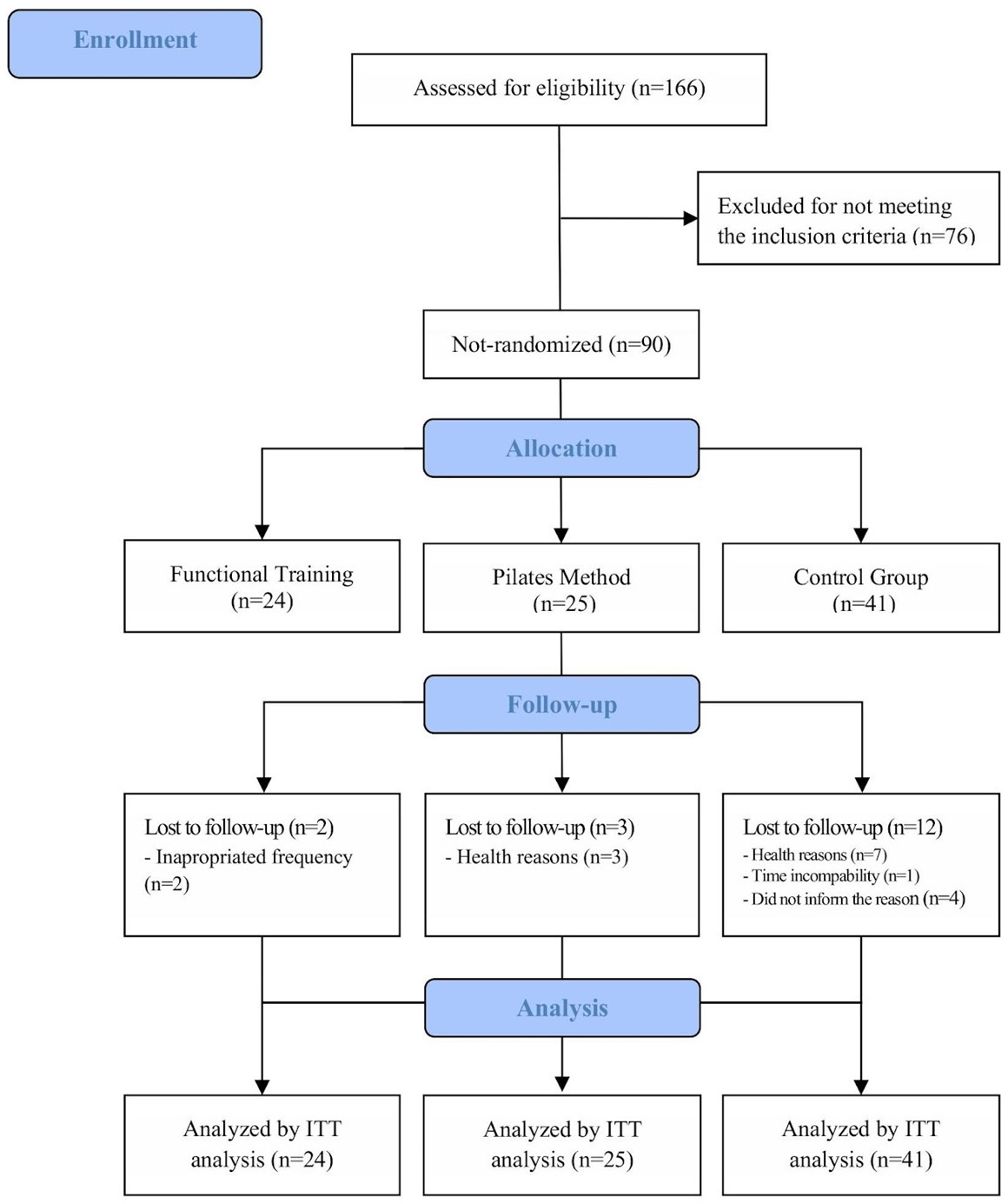
Table 2 summarizes the descriptive and comparative analyses of BDNF levels and physical fitness variables across the three groups, using thee Generalized Estimating Equations analysis. Bonferroni post-hoc was used for pairwise comparisons and Cohen’s d for effect size for Pre-post and post-post comparison. A significant group × time interaction effect was detected for BDNF levels (p = 0.001) and the six-minute walk test (p = 0.007), indicating differential responses to the interventions. Significant increases in BDNF levels were observed following the exercise programs in both the functional training group (p < 0.001; Cohen’s d = 0.884) and the Pilates group (p = 0.001; Cohen’s d = 0.777). In contrast, the control group experienced a reduction in BDNF levels (p = 0.025; Cohen’s d = -0.292). Regarding physical fitness outcomes, the distance covered in the six-minute walk test significantly increased exclusively in the functional training group (p = 0.001; Cohen’s d = 0.491). The Short Physical Performance Battery scores improved in both the functional training group (p = 0.001; Cohen’s d = 0.580) and the control group (p = 0.001; Cohen’s d = 0.463). As a post hoc analysis, the distance covered in the six-minute walk test increased significantly in the functional training group compared to both the Pilates (p<0.001; Cohen’s d =-1.122) and control (p<0.001; Cohen’s d =-1.075) groups. As a post hoc analysis, the Short Physical Performance Battery score increased significantly in the functional training group compared to the Pilates (p=0.05).
Discussion
The present study aimed to examine the effects of two different multicomponent exercise programs on BDNF levels and physical fitness in older women. Our results demonstrated that functional training and Pilates method led to increased BDNF levels. However, the functional training program notably resulted in a more significant increase in BDNF levels and enhanced performance in functional test after training.
BDNF plays a pivotal role in synaptic modulation, neurogenesis, and neuronal survival. Notably, skeletal muscle also synthesizes BDNF, where it is critical for maintaining muscle function and adaptability [32,33]. Basic research indicated that intracellular messengers such as calcium and cyclic adenosine monophosphate (cAMP) indirectly activate the BDNF production [32]. Emerging evidence highlights BDNF’s involvement in key cellular processes such as the reinforcement of neuromuscular junctions, promotion of muscle regeneration and regulation of insulin-mediated glucose uptake during exercise [32,34]. These mechanisms explain the significant increases in BDNF observed in the functional training and Pilates groups in our study. Functional training, characterized by dynamic, multi-joint exercises, likely induces greater neuromuscular activation and metabolic demands, thereby enhancing BDNF synthesis in skeletal muscle and its subsequent release into circulation [35]. Similarly, Pilates, which focuses on controlled movements and core stabilization, may stimulate BDNF production through sustained activation of targeted muscle groups and the modulation of central and peripheral pathways. Conversely, the reduction in BDNF levels observed in the control group aligns with existing evidence suggesting that physical inactivity leads to diminished BDNF production. These findings underscore the importance of well-designed and carefully prescribed exercise programs to promote optimal physiological and molecular responses, particularly those related to BDNF levels [32,34]. Although control group also received cognitive stimuli through the Health Education intervention, the frequency of these stimuli may not have been sufficient to induce changes at the brain level, especially as this group did not receive any physical stimuli. In this context, previous studies have suggested that activities combining physical and cognitive stimuli are a more promising approach for enhancing cognitive performance in older adults than cognitive training alone [36]. Additionally, it is important to highlight that although a statistically significant decrease in BDNF levels was observed in the control group, the effect size was small (d = -0.292), indicating no negative impact on functional tests such as the Short Physical Performance Battery and six minute walk test. Furthermore, no adverse events were reported in this or any other group.
Netz [37] described two categories of exercise that promote improvement in cognition in older adults: (1) physical training (aerobic and strength, modulated by intensity), and (2) motor training (balance, coordination, and flexibility), modulated by the complexity of the task. Both categories were incorporated into the multicomponent exercise programs in our study, particularly in the functional training program. The motor training component in both interventions involved various combinations of movements with different levels of complexity. Consequently, the progressive increase in task complexity provided continuous cognitive stimulation, similar to the acquisition phase of motor learning, which promotes brain reorganization and plasticity in cortical and hippocampal areas [38]. In addition, exercises with high cognitive and attentional demands. such as motor coordination exercises, are known to stimulate brain plasticity [33,38]. This cognitive stimulation may have contributed to the increase in BDNF levels observed in both multicomponent programs. However, since the task complexity and cognitive stimulation were greater in the functional training program, the increase in BDNF was more pronounced in this group.
While motor training enhances neuroplasticity through neuromuscular mechanisms, physical training benefits cognition by improving cardiovascular fitness [37]. Aerobic and strength exercises have demonstrated positive effects on cardiovascular fitness in older adults, particularly on endothelial function, which is one of the mechanisms by which physical exercise positively impacts cognitive function in this population [39]. The mechanisms underlying these effects are not yet fully understood, but it is hypothesized that physical exercise stimulates certain brain areas, leading to an increase in local blood flow to meet neuronal metabolic demands [40]. This increased brain activity subsequently stimulates the release of BDNF and other neurotrophins associated with brain plasticity [8]. In addition, increased blood flow also generates an increase in shear stress [40] which, in turn, triggers a cascade of cell signaling. including the release of BDNF from platelets and vascular endothelial cells [8].
Interventions incorporating strength training for durations between 6 and 12 weeks, as well as combined aerobic and strength training lasting between 8 and 24 weeks, have been shown to positively affect peripheral blood BDNF concentrations in older adults [11]. In the current study, functional training led to a more pronounced increase in BDNF levels compared to Pilates. This can be attributed to the functional training program’s incorporation of various dual-task activities alongside substantial aerobic stimuli, which facilitate greater cardiovascular benefits, as evidenced by the improvements in the six-minute walk test observed in this group. Improvements in aerobic conditioning have been associated with increases in BDNF levels in older women who participated other multicomponent exercise programs [41]. Aerobic exercise also benefits brain structure and function, such as increased blood flow and brain volume. which are factors related to higher levels of BDNF [42].
Functional training with different physical stimuli combined with cognitive-motor dual-task is a new method compared to traditional Pilates. While previous studies have reported benefits for physical and cognitive functions in older adults in functional exercise programs [23,27,35], this is the first study to demonstrate the effect of this type of exercise on BDNF levels in this population. Our findings indicate that a functional exercise program involving tasks with varying levels of complexity has a positive impact on BDNF levels and physical function, as measured by the six minute walk test and Short Physical Performance Battery. These results are significant for clinical practice, as they suggest that functional exercises can also produce systemic effects. Future research should explore different intensities and frequencies of multicomponent exercises on physical and cognitive variables and determine whether there is a minimum frequency required to achieve the benefits of physical exercise.
This study has several limitations that should be acknowledged. One limitation is the use of a convenience sampling method, which may not accurately represent the broader population and thus limits the generalizability of the findings. Additionally, the non-randomized nature of the sample introduces the possibility of unmeasured confounding factors beyond those accounted for as covariates that could have influenced the results. However, the similar baseline characteristics among the women in the three groups likely helped mitigate potential confounding effects. Moreover, as the sample exclusively comprised physically independent older women, the findings may not be applicable to older men or individuals with varying levels of functional status. Another limitation of this study is the lack of assessment or control of participants' protein intake, overall dietary consumption, and medication type or dosage, all of which could have influenced the results. Future randomized controlled trials are needed to confirm and expand upon the results observed in this study. These trials should include both men and women, account for dietary intake, and measure additional biological variables associated with cognitive function to provide a more comprehensive understanding of the observed outcomes.
According to the guidelines for reporting Sex and Gender Equity in Research (SAGER), it is important to acknowledge that, despite efforts to recruit men, most participants in this study were women [43]. Consequently, only women were included as participants, as recruiting men for each group proved challenging. Furthermore, it is important to highlight the persistent gap in the representation of women in studies involving human subjects, underscoring the significance of this study in addressing this underrepresentation.
Despite the limitations, the exercise programs included in this study demonstrate high applicability to clinical practice within the context of community-dwelling older adults. Furthermore, this is the first study to analyze the biological effects of the Functional Exercise Circuitprotocol on BDNF levels in older women. Future studies are necessary to determine whether these effects are also observed in older men and in older adults with other functional status.
Conclusions
In conclusion. while both multicomponent exercises increased BDNF levels over a 12-week intervention with a large effect size, functional training yielded superior results compared to the Pilates method, possibly mediated by improvement in physical function. Additionally, although an increase in physical function was observed in the control group in the Short Physical Performance Battery, individuals exhibited a decrease in BDNF levels with a small effect size. The control group received an educational program without an exercise intervention. These findings highlight the significant impact of exercise programs on BDNF levels and other clinical variables in older adults. Future studies should explore varying intensities and frequencies of multicomponent exercise on both physical and cognitive outcomes and determine if there is a minimum frequency required to achieve the benefits of physical exercise.
