Estudios originales
← vista completaPublicado el 3 de marzo de 2025 | http://doi.org/10.5867/medwave.2025.02.3023
Valores de fuerza de prensión manual y composición corporal en jóvenes universitarios ecuatorianos
Handgrip strength values and body composition in Ecuadorian university young adults
Abstract
Introduction Handgrip strength is a key indicator of functional health and overall muscular strength. These parameters are essential for assessing physical performance and health status. This study aims to assess handgrip strength and body composition in young Ecuadorian university adults.
Methods This was a cross-sectional study conducted among university students from the Faculty of Health Sciences at Universidad Católica de Santiago de Guayaquil. Participants completed a self-administered questionnaire for demographic variables. Handgrip strength was assessed in both hands with an hydraulic dynamometer. Body composition was measured using a bioelectrical impedance device.
Results 350 participants were included in the study, consisting of 65.5% (n=233) females and 33.4% (n=177) males. The mean age was 22 ± 2.09 years. The mean muscle mass was 24.4 ± 6.9 kg, and the mean fat mass was 22.0 ± 12.9 kg. The visceral fat value was 8.0 ± 3.1 points. The mean handgrip strength for males was 39.6 ± 8.07 kg in the right arm and 38.5 ± 8.07 kg in the left hand, and for females, was 23.0 ±5.57 kg in the right arm and 22.0 ± 5.84 kg in the left arm. Muscle mass positively correlated with handgrip strength in both sexes and both hands, with Rho = 0.813 (p<0.001) for the right arm and Rho = 0.798 (p<0.001) for the left arm.
Conclusions We established reference values for handgrip strength and body composition in healthy young Ecuadorian adults, showing handgrip strength’s positive association with muscle mass and anthropometric variables.
Main messages
- Handgrip strength serves as an indicator of overall strength and health and body composition in young adults can identify excesses or potential nutritional risks.
- In this study we established reference values for handgrip strength and body composition in healthy young Ecuadorian adults.
- Muscle mass was positively correlated with handgrip strength in both sexes and for both hands.
- The main limitation of this study was the lack of evaluation of physical activity, as self-reported data from participants may not be sufficiently accurate and reliable.
Introduction
Muscle mass is strong indicator of health due to its role in metabolism [1], hormonal status [2], and physical function [3].
In this sense, muscle mass and quality are essential in clinical outcomes such as frailty [4], sarcopenia [5], malnutrition [6], and functional disability [7]. A common practice in evaluating muscle quality often involves measuring muscle strength [8].
Muscle mass and strength are at their peak in young adults, and it can be increased more easily than in older adults [9]. In young adults, muscle strength is influenced by dietary patterns [10] and physical activity [11].
Handgrip strength is a simple and practical metric method for assessing upper limb muscle force, that can reflect overall body muscle mass, especially in young adults.
Our study aimed to analyze the relationship between muscle mass and muscle strength in young adults.
Methods
Study design
An observational cross-sectional study was conducted from July to December 2023. Healthy young adults studying at the Faculty of Health Sciences of the Universidad Católica de Santiago de Guayaquil were enrolled.
Subjects
Young adults of both sexes aged 18 or older were included. Pregnant university students, individuals with lower limb amputations, and those who did not sign the informed consent for participation were excluded.
Sociodemographic information, including age and sex, and basic medical information about possible chronic disease, medication were registered. The acceptance or denial of participation in the survey formed the principal basis for inclusion or exclusion criteria in the study.
Variables
Basic anthropometric measurements were registered following the International Society of Advancement of Kinanthropometry protocol [12], and consisted of weight (kg), height (m), waist circumference (cm), and body mass index (BMI) (kg/m2). BMI was categorized according to the consensus [13] classification: underweight: < 18.5 kg/m2, normal weight: 18.5 to 24.9 kg/m2, overweight grade I: 25.0 to 26.9 kg/m2, overweight grade II: 27.0 to 29.9 kg/m2, obesity type I: 30.0 to 34.9 kg/m2, obesity type II: 35.0 to 39.9 kg/m2, obesity type III: 40.0 to 49.9 kg/m2, obesity type IV: ≥ 50 kg/m2.
Body composition compartments such as muscle mass, fat mass, and body fat percentage were measured using a Multifrequency Segmental Body Composition Analyzer (InBody 270 DSM-BIA®). Before the bioelectrical impedance analysis procedure, participants were advised not to eat solids or drink liquids 4 hours before the test, and restrict caffeine, alcohol and exercise.
Handgrip strength was evaluated using a Jamar Plus Hand Dynamometer. Participants were given instruction for the procedure. They were then asked to grip the instrument and perform maximum handgrip strength. All measurements were taken while standing, with both arms hanging naturally at the sides and the dynamometer facing the evaluator. The highest value recorded for each hand was registered. Participants who reported any discomfort during the evaluation were excluded.
Statistical analyses
Descriptive statistics included means, standard deviation, and prevalence. Normality tests were included in the analysis using the Kolmogorov-Smirnov test, and the Spearman correlation coefficient was used to evaluate the correlation between main variables. In addition, the U-Mann Whitney test was used to compare the mean values of the dominant and non-dominant hand dynamometry for both gender and age groups. Data collected were analyzed using the SPSS 25.0 statistical package.
Ethics
The Ethics Committee for Research in Humans of Hospital Clínica Kennedy reviewed and approved the research protocol (Protocol approval: CEISH No: HCK-CEISH-20-0001). All participants were informed about the research and gave written consent to participate. The study followed international bioethical standards following the Declaration of Helsinki Statement of 2008, updated in Fortaleza, October 2013.
Results
Figure 1 shows the flowchart of the recruitment process for the study. 856 university students registered in the 2022 academic period were invited to participate and a total of 362 individuals expressed their willingness to participate in the survey.
Flowchart of the participant recruitment process.
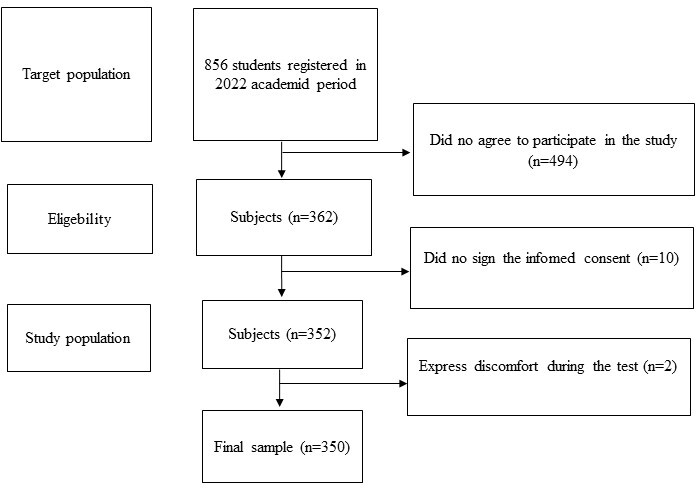
A total of 350 individuals were finally recruited, comprising 66.5% (n=233) females and 33.5% (n=117) males. The mean age was 22 ± 2.09 years (95% confidence interval (CI): 21.3 to 21.8). Participant distribution by university carrer was as follows: 37.7% (n=132) medicine, 28.6% (n=100) nutrition and dietetics, 17.4% (n=61) physiotherapy, 16% (n=56) dentistry, and one student was from nursing.
Mean BMI was 24.9 ± 4.4 kg/m2 (95% CI: 24.2 to 25.2). According to BMI classification, 17.4% (n=61) and 12.9% (n=45) presented overweight grade I and overweight grade II, respectively, while 10.9% (n=38) presented obesity type I and 1.7% (n=6) presented obesity type II.
Mean muscle mass was 24.4 ± 6.9 kg (95% CI: 23.5 to 25.1), and fat mass in kilograms as well in percentage was 22.0 ± 12.9 (95% CI: 20.1 to 23.3) and 32.2 ± 9.0 (95% CI: 30.9 to 33), respectively. The visceral fat was 8.0 ± 3.1 points (95% CI: 7.4 to 8.2). Males presented higher mean values, except for fat mass and visceral fat. The measurements showed significant differences between sexes (p<0.05). The anthropometric and body composition characteristics are summarized in Table 1.
Mean handgrip strength values for males were 39.6 ± 8.07 kg (right arm) (95% CI: 38.2 to 41.1) and 38.5 ± 8.07 kg (left hand) (95% CI: 37 to 39.9); females handgrip strength was it 23.0 ± 5.57 kg (right arm) (95% CI: 22.3 to 23.7) and 22.0 ± 5.84 kg (left arm) (95% CI: 21.3 to 22.7). There was no significant difference in handgrip strength values between both hands.
Figures 2A and 1B show the handgrip strength distribution for both hands, according to sexes and by size ranges, whereas higher average values were observed in males.
Handgrip strength of the right and left arms across different height ranges and by sex.
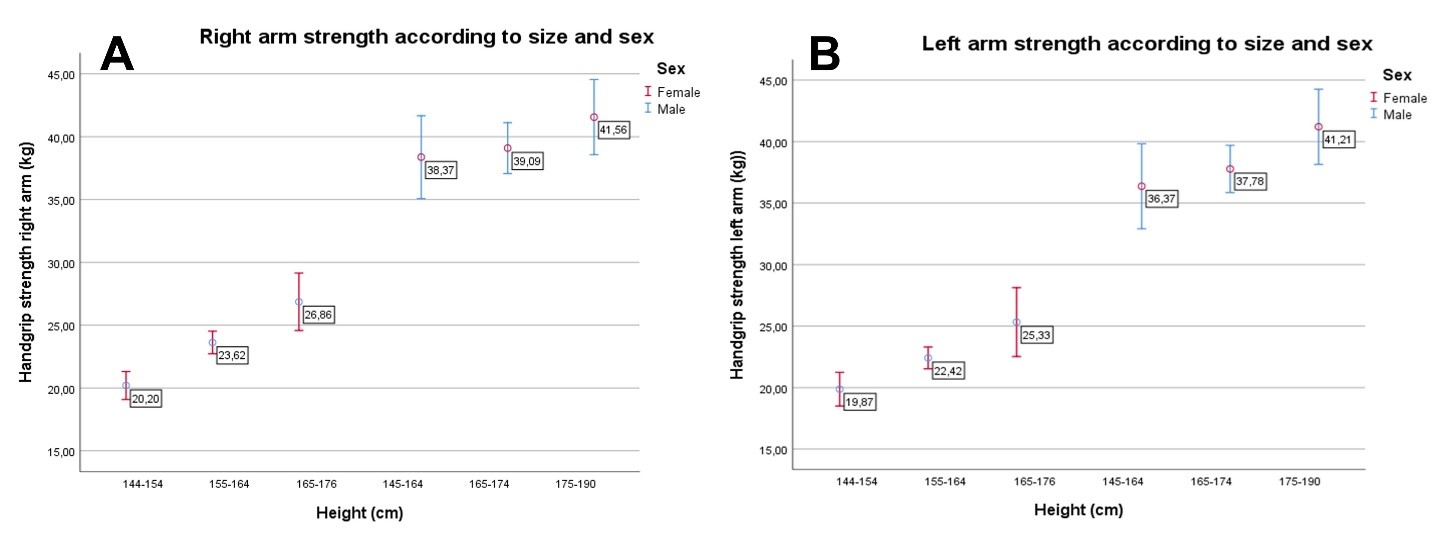
Source: Prepared by the authors of this study.
Fat-free mass (muscle mass) correlated positively with handgrip strength in both sexes and both hands, with Rho = 0.813 (p<0.001) for the right arm and Rho = 0.798 (p<0.001) for the left arm (Figure 3).
Positive correlation between fat-free mass and handgrip strength for both arms.
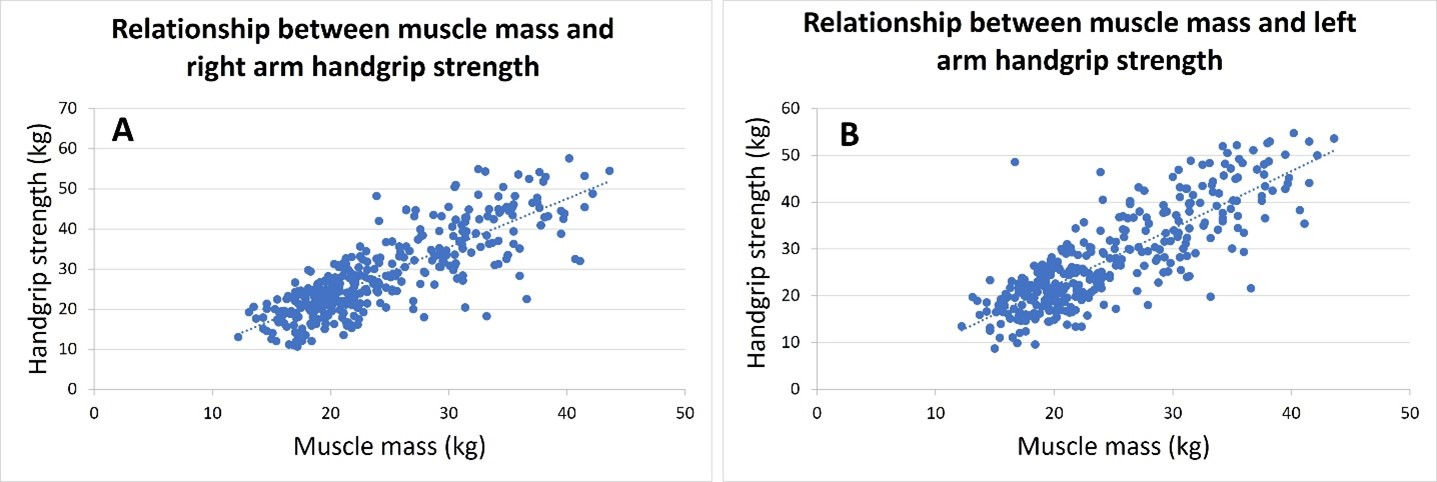
Data and source: Prepared by the authors of this study.
Discussion
Main findings of this study were the establishment of reference values for handgrip strength and its relationship with anthropometric variables. Our country lacks handgrip strength values across all life stages and some studies have been carried out in older adults [14,15,16]. In our young adult population, handgrip strength varied from 35 to 44 kg for males and 19 to 29 kg for females. In young adults, handgrip strength is strongly and positively associated with anthropometric variables related to higher muscles mass, such as body weight, and height [17].
Our study found, mainly in the females, that handgrip strength is strongly and positively associated with body size, with taller and heavier individuals. However, compared to studies from other regions [18,19,20], handgrip strength values for both sexes in our cohort are lower. In this sense, the mean handgrip strength in young adult men and women of a Chinese cohort present values of 44.0 ± 7.4 kg and 25.5 ± 4.48 kg, respectively, while in the Portuguese reference values they reflect a mean of 47.6 ± 4.1 kg for men and 31 ± 6 kg for women in this same age group.
This discrepancy may be attributed to differences in anthropometric characteristics and population-specific factors. In particular, height was identified as a significant predictor of handgrip strength among women, a trend also observed in previous studies [21].
Most of our cohort exhibited normal weight status, similar to other university populations in Latin America, yet showed higher waist circumference, BMI, and fat mass compared to a Spanish cohort and lower values compared to a Chilean sample [22]. These differences underscore the need for region-specific reference values.
Handgrip strength is a simple, noninvasive, rapid, objective, and low-cost procedure used in clinical and epidemiological studies [23]. Recently, it has been proposed as a “new vital sign of health,” acting as a fundamental measure for assessing muscle function and physical capability [24].
Handgrip strength values are useful as indicators of present and future physical function and health status, reflecting nutritional status related to muscle mass quality [25]. Reference ranges for handgrip strength throughout life have been published mainly in developed countries [20,26,27]. In Latin America, Brazil, Chile, and Colombia have contributed handgrip strength data for adults and older adults [17,22,28]. The usefulness of having reference values for handgrip strength lies in interpreting them according to geographic zone, ethnicity, age, sex, and height [29].
Most of our study cohort exhibited normal weight status as determined by BMI measurements, similar to other university cohorts in Latin America [30,31,32]. Additionally, body composition compartment variables and anthropometric data were significant and positive independent contributors to handgrip strength for both sexes, as other authors have reported [33]. The significant positive correlation between muscle mass and handgrip strength (Rho>0.8, p<0.001) observed in both genders underscores the interdependence between body composition and functional capacity, as reported by other studies [21]. We did not find significant differences between dominant and non-dominant hands.
Our findings provide valuable insights into handgrip strength and body composition in Ecuadorian young adults, representing the first steps in researching the long-term health impacts of these variables in our country.
There are limitations considered for this study. First, physical activity was not evaluated because the self-reported data from participants may need to be more accurate and reliable. We recommend assessing this variable in future research using validated questionaries, as it can significantly impact muscle mass and grip strength and could influence the interpretation of results. Moreover, the gender distribution is uneven, which might skew the results, especially when analyzing sex differences. On the other hand, the academic cycle of the students was not recorded, limiting our ability to explore variations in handgrip strength and body composition indicators across different stages of their academic careers. Finally, the sample was not randomized, which represents a risk of selection bias.
Conclusions
This study establishes reference values for handgrip strength and body composition in healthy Ecuadorian young adults of both sexes, providing baseline data for future research. Our findings indicate that handgrip strength is positively associated with muscle mass and anthropometric variables such as height and weight. The study reveals that Ecuadorian young adults have lower handgrip strength values than their counterparts in other regions, potentially influenced by different anthropometric characteristics. The reference data for handgrip strength presented in this study for young adults in Ecuador highlight the importance of considering geographic, ethnic, age, sex, and height differences when interpreting these values.
