Estudios originales
← vista completaPublicado el 14 de mayo de 2025 | http://doi.org/10.5867/medwave.2025.04.3059
Evaluación de la capacidad funcional mediante la prueba de sit-to-stand de 5 repeticiones: valores de referencia para personas que viven a gran altitud
Functional capacity assessment through five-repetition sit-to-stand test: Reference values for people living at high-altitude
Abstract
Introduction The five repetitions sit-to-stand test is commonly used to evaluate physical function, mainly to determine the risk of falls, and is also included as a component in other evaluations, such as the Short Physical Performance Battery. However, reference values are currently unavailable for populations living at high altitudes. This study aimed to establish normative values for the five repetitions sit-to-stand test in the population living 2500 meters above sea level.
Methods A multicenter, cross-sectional research was carried out, collecting data from two high-altitude cities in Ecuador. Healthy adults aged 18 to 80 were recruited. Anthropometric measurements, physical activity levels, and tobacco use were registered. Reference equations were determined using multiple linear regression separately for men and women. The predictive model was generated using stepwise method.
Results 400 healthy subjects (58% women) were recruited in the study. The participants had a median (P25 to P75) height of 1.62 (1.56 to 1.68) m, weight of 63.0 (57.8 to 70.1) kg, and Body Mass Index of 24.2 (22.5 to 26.0) kg/m. For men aged 18 to 29 years, the results for the five repetitions sit-to-stand test ranged from (P25 to P75) 5.1 to 9.3 seconds and between 8.2 to 12.2 seconds for people aged 70 to 80 years. For women aged 18 to 29 years, the results for five repetitions sit-to-stand test ranged from (P25 to P75) 5.0 to 7.9 seconds and between 8.2 to 14.3 seconds in the range 70 to 80 years.
Conclusions Reference values were established for the five repetitions sit-to-stand test in the healthy population living at high altitudes, between 18 and 80 years old.
Introduction
Functional capacity is defined as the autonomous execution of activities that make up our daily chores in a way desired at an individual and social level [1]. Functional capacity can be measured with several tests, including the time-up-go test, usual gait speed, and the five-repetition sit-to-stand test [2,3,4].
The five-repetition sit-to-stand test is a frequently tool used to evaluate physical function due to its similarity to an activity of daily living and depends significantly on the function of the muscles of the lower extremities [2,5,6]. This test measures the time required to complete five repetitions of sitting and rising from a chair as quickly as possible [2], and correlates with fall risk in various studies [7,8]. One notable advantage of the five-repetition sit-to-stand test is the short time required for its execution and minimal need for materials or equipment as it only requires a straight-backed chair and a stopwatch [2].
This assessment evaluates physical function when applied independently and is also a key component of multidimensional assessments such as the Short Physical Performance Battery, which consists of three tests: balance, walking speed, and the ability to stand up and sit down from a chair five times [9,10].
When utilizing functional tests such as the five-repetition sit-to-stand test, having reference values is essential to interpret the results accurately within the appropriate context [11]. Currently, reference values are available for healthy people but these normative values are usually established for individuals over 60 years of age and for populations residing below 2500 meters above sea level [2,12].
While current reference values from other settings can provide a helpful starting point, it is essential to account for differences in other countries and local environments, particularly in regions with high altitudes. Therefore, establishing local reference values is necessary to facilitate a more accurate and adapted evaluation of subject’s physical function and progress in their specific environment. In addition to establishing reference values, predicting the performance of the five-repetition sit-to-stand test can be beneficial when direct measurement is not feasible, particularly in clinical or epidemiological contexts. Predictive equations based on demographic and anthropometric characteristics, such as age, height, and weight, provide a practical tool to estimate functional capacity. For this reason, this study aims to determine reference values of the five-repetition sit-to-stand test in people living at high altitudes by sex, and age and, secondarily, to develop predictive equations to estimate test performance when direct assessment is not possible and to determine the correlation between anthropometric characteristics, physical activity levels and the duration of the test.
Methods
Study design and participants
We conducted a cross-sectional study from January to March 2024 in two cities of Ecuador, in Quito (2850 m) and Latacunga (2860 m). This protocol was approved by the Ethics Committee of Ecuador, Quito (CEISH-HGDC 2024-004). All subjects gave written consent. This research was conducted in accordance with the “Strengthening the Reporting of Observational Studies in Epidemiology” (STROBE) Guidelines [13].
The volunteers were invited from the general population and one of the recruitment strategies consisted of disseminating the plan through posters that were sent through social networks. The inclusion criteria were individuals aged between 18 and 80, perceived themselves as healthy, and self-reported the ability to sit and rise from a chair. Exclusion was based on the following criteria: body mass index (BMI) ≥ 35 kg/m2, having acute or chronic respiratory pathology in the last 30 days, having an chronic or acute musculoskeletal injury, related cardiac, neuromuscular or cerebral disease that prevents testing, and having a disability to understand instructions.
Measurements
The five-repetition sit-to-stand test was executed based on the specific methodology in Cruz-Montecinos et al. study, which consists of starting from a seated position in a chair, reaching a straight position in a bipedal posture with the knees in maximum extension, and returning to the initial seated position in the chair [14]. The entire technical gesture must be performed with crossed arms at the contralateral shoulder [14]. A standard 46 cm height of the chair was used [15]. Participants sat upright in a chair placed against the wall, with hips and knees positioned at 90 degrees and feet flat on the floor [15]. The time required to complete five full sit-to-stand cycles was precisely measured using a stopwatch [16]. The participants were instructed to perform sitting and standing up five times as quickly as possible. Using a stopwatch, it started quickly after the participant got up from the chair and ended once he sat down again during five repetitions [15].
The evaluators performed the five-repetition sit-to-stand test on three individuals to verify consistency across centers, documenting each session [14]. The principal investigator reviewed the videos, paying particular attention to technique adherence and repetition accuracy [17]. Sampling was allowed to commence only once all three videos met the established standards [14,17]. The objective was to verify that the staff was aware of compliance with the study protocol.
All participants were assessed following a standardized evaluation protocol [14]. At baseline, data on participants' physical and demographic characteristics were collected. For tobacco use, participants were asked to indicate whether they were “Active smokers,” “Never smokers,” or “ex-smokers”. The short version of the International Physical Activity Questionnaire (IPAQ-SF) [18] was used to indicate the level of physical activity [18]. Participants were categorized according to their activity level as low, moderate, and high [18].
Statistical analysis
Data were analyzed using the statistical IBM SPSS version 25.0 (IBM Corporation, Armonk, NY, USA). The Kolmogorov-Smirnov test was applied to assess data distribution. Continuous variables were presented as median (percentile 25th to 75th), and categorical variables were presented as frequency and percentage. The Spearman test was applied to analyze correlations among variables, for example, age, weight, height, and BMI, with the five-repetition sit-to-stand test results.
To examine the relationship between individual performances in the five-repetition sit-to-stand test and age, we generated dispersion graphs to visualize performance in relation to age and sex. To assess the physical activity impact on five-repetition sit-to-stand test performance, we compared the time at different levels of physical activity, as measured by IPAQ-SF. This comparison was conducted using t-tests or Kruskal-Wallis tests.
To derive the reference equations, multiple linear regression was conducted separately for men and women, using performance in the five-repetition sit-to-stand test as the dependent variable. The predictive model was developed using the stepwise method. Sex- and age-specific normative percentiles (2.5th, 25th, 50th, 75th, and 97.5th) were calculated directly from the observed test values to establish the reference values.
Results
Four hundred people were included in the study, including 167 men (41.8%) and 233 women (58.2%). Regarding physical activity, 36.8%, 47.8%, and 15.6% reported having low, moderate, and high physical activity, respectively. The 32.5% declared themselves smokers and 65.5% declared themselves non-smokers. The baseline characteristics of the population can be found in Table 1.
The correlations between the values of five-repetition sit-to-stand test and age revealed a strong correlation (r = 0.7; p < 0.001), a low correlation with BMI (r = 0.3; p = <0.001), and with the height (r = - 0.3; p = <0.001). The median duration according to physical activity level did not show statistical significance.
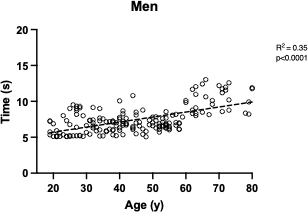
The median duration of the five-repetition sit-to-stand test varies between 5.5 and 11.4 seconds in women and between 5.7 and 11.4 in men. The performance behavior of the test and age are depicted in Figures 1 and 2. The values obtained by sex and age range can be observed in Table 2.
Association between the duration of the five-repetition sit-to-stand test and age in men.
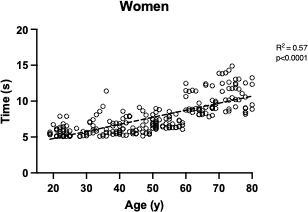
Association between the duration of the five-repetition sit-to-stand testand age in women.
The predictive equations presented in this study are intended to estimate the five-repetition sit-to-stand test performance based on demographic and anthropometric variables. These equations are helpful when direct measurement is not feasible, offering a reliable method for assessing functional capacity. Additionally, the correlation between the test results and variables such as age, height, and weight provide insight into the factors influencing test performance.
The predictive equations found were:
Men:
5STST = 9.822 + (0.064 × age) − (0.054 × height) + (0.054 × weight)
R² = 0.40; Adjusted R² = 0.39; RMSE = 1.461
Residual Mean Square Error = 2.134
Standard Errors: Age = 0.008, Height = 0.021, Weight = 0.015
Women:
5STST = 13.289 + (0.088 × age) − (0.082 × height) + (0.049 × weight)
R² = 0.61; Adjusted R² = 0.61; RMSE = 1.444
Residual Mean Square Error = 2.086
Standard Errors: Age = 0.006, Height = 0.018, Weight = 0.014
Discussion
This research has established a standardized benchmark specific to high-altitude settings, enabling more precise comparisons of individual five-repetition sit-to-stand test performance within these regions. This effort aims to improve the comprehension and interpretation of clinical findings within this distinctive context. These values were derived from a diverse healthy population aged between 18 and 80 years from Ecuador residing at altitudes of 2500 meters above sea level.
Integrating such diverse and representative group allows for the application of these reference values in comparable contexts where regional data may be lacking. Additionally, using standardized values from different groups may result in inaccuracies and diagnostic errors, as individual differences might not be properly considered. Consequently, the American Thoracic Society (ATS) and European Respiratory Society (ERS) Statement advises utilizing normative values derived from the same population where the procedures will be implemented [19].
Our data revealed that the median five-repetition sit-to-stand test duration for women was lower than that of men in almost all age ranges. Our data aligns with Klukowska et al. for individuals under 60 years of age; however, they differ in those over 60 years of age in which they showed that men took around 0.8 seconds less time in Klukowska’s cohort [12]. Although they exist in our sample and are approximately 10 cm shorter in height, they simulate BMI and a very similar test protocol, with an almost identical male/female distribution [12].
Contrastingly, the influence of sex on the predictive equations of the five-repetition sit-to-stand test appears less straightforward. For instance, Vilarinho et al. did not use the sex variable in their predictive equation, citing its lack of significance in the model’s construction [15]. Moreover, Furlanetto et al. showed heterogenous behavior across age ranges, with men exhibiting lower values in certain age groups (30 to 39 years, 50 to 59 years) and women having lower values in others (i.e., 20 to 29 years, 40 to 49 years) [20]. Furthermore, Furlanetto et al., despite having a higher percentage of women (55%), had almost equal times for both sexes [20].
The literature has shown lower physical function performance in individuals residing at high altitudes [22]. For instance, in a cross-sectional study comparing older adults living at sea level vs. older adults living above 3300 meters above sea level, it was observed that those who lived at altitude took longer to complete the five-repetition sit-to-stand test, in addition to having a higher score in the short physical performance battery compared to those who lived at sea [22]. While our study does not compare individuals at different altitudes, these findings underscore the importance of establishing reference values specifically tailored for individuals living at high altitudes.
The development of predictive equations adds value to the clinical application of the five-repetition sit-to-stand test, mainly when the test cannot be directly performed. These equations allow healthcare professionals to estimate expected performance based on readily available anthropometric data, supporting decision-making and patient evaluation in diverse settings.
Strengths and limitations
One of the strengths of our data is the high r2 value, which exceeds 0.6 for women and reaches 0.4 for men. These values are notably higher compared to those reported in the literature. For instance, Vilarinho et al. reported an r2 of 0.27 in their equation incorporating both sexes [15], while Furlanetto et al. reported an R-squared of 0.28 for both sexes [20].
We acknowledge several limitations in our study. Firstly, the categorization of seemingly healthy individuals is defined by self-report and the lack of clinically diagnosed health conditions. However, it is important to recognize that studies with extensive cohorts designed to establish reference parameters often include subjects with unrecognized conditions or diseases. Secondly, some age ranges, particularly older adults, are underrepresented. This is a common challenge in studies of this nature, given that recruiting “healthy” older people can be difficult, mainly in Latin America. Additionally, our study did not compare individuals living at high altitudes with those residing at sea level. Therefore, future studies should explore these potential differences.
Conclusions
Reference values were established for the five-repetition sit-to-stand test in the healthy population living at high altitudes, between 18 and 80 years old. These data are valuable for performing optimal evaluations and determining the impacts of interventions that involve the evaluation of physical function using this test.
