Estudios originales
← vista completaPublicado el 27 de agosto de 2025 | http://doi.org/10.5867/medwave.2025.07.3070
Caracterización de la demanda expresada y efectiva de servicios oncológicos del régimen de Garantías Explícitas de Salud en el sistema de salud público de Chile
Characterization of the expressed and effective demand for oncology services under the explicit health guarantees of the Chilean public health system
Abstract
Introduction Efficient and effective cancer management is a priority for the Chilean healthcare system. In recent years, significant progress has been made through public policies integrating management at different levels (micro, meso, and macro). However, gaps between the population’s needs, service availability, and effective demand may impact health outcomes.
Objective To describe the national effective demand for prioritized cancer services within the Chilean public healthcare system.
Methods A descriptive comparative analysis was conducted using data from the public sector Health Guarantees Management Information System between 2018 and 2022. The rates of new cases granted health guarantees by intervention type and the analysis of delayed guarantees were performed.
Results A total of 3.8 million new cases of explicit health guarantees and 3.9 million fulfilled opportunity guarantees were included. The rates of primary treatment opportunity guarantee by tracer intervention declined in 2020 and 2021, while delayed guarantees showed an increasing trend throughout the entire period. Effective demand varied across cancer types. Breast cancer, preventive cholecystectomy, and gastric cancer exhibited the largest sex-based differences in new cases and primary treatment. Delayed guarantees were similar between sexes, except for breast cancer.
Conclusions This study provides valuable insights into the demand for cancer services in Chile and the performance of the public healthcare system concerning sex and cancer type, highlighting the impact of the COVID-19 pandemic. The findings emphasize the need to strengthen the public system’s response capacity to reduce gaps and improve equity in oncological care.
Main messages
- The COVID-19 pandemic aggravated the gaps between the need for oncologic care, the supply of services, and the effective demand in the Chilean public health system, resulting in a decrease in treatments and an increase in delayed guarantees.
- This study analyzes the effective demand for oncological services in the Chilean public system, differentiating by type of cancer and sex, and highlights the impact of the COVID-19 pandemic on access to treatment and guarantees.
- This study used secondary data from the Explicit Health Care Management Computer System, which may imply biases in the registry. No clinical or socioeconomic factors that may influence effective demand are analyzed. In addition, the impact of the pandemic may not fully reflect other structural barriers to cancer care.
Introduction
Cancer is a global public health problem that negatively impacts individuals, families, teams, and health systems, leaving devastating sequelae in society. In Chile, this disease is the leading cause of death [1], and the number of people dying is expected to continue to increase by 10% [2]. Access to cancer diagnosis is one of the most delayed health problems [3]. In terms of costs, this disease represents 8.9% of total health expenditure, 67% of which is associated with only five types of cancer [4].
In response, Chile has made progress in terms of health policies and programs aimed at people with cancer. Currently, there is Law No. 21 258 (National Cancer Law), the National Cancer Plan 2018-2028, the General Framework of the National Cancer Plan 2022-2027, and Law 19 966 on Explicit Health Guarantees. All these instruments establish a regulatory framework with strategic and organizational guidelines for the healthcare response, from an integrated network of services perspective, for cancer care in the country. For example, the National Cancer Plan 2018 to 2028 considers, in its strategic lines, the provision of care services, highlighting the need to improve the supply to ensure comprehensive care at all levels. These regulatory instruments converge in clinical practice with management commitments, health goals, and financial incentives to providers and health teams, significantly impacting the productivity of the system and health outcomes.
Effective policy making must consider the relationship of the three key elements of health care: need, demand, and supply [5]. The definition of need is complex, as it is determined by the perspective from which it is made. As early as 1972, Bradshaw proposed four types of need: normative needs (defined by experts); comparative needs (comparison of one group of people with another); expressed needs (needs manifested by an action, such as going to the doctor); and perceived needs (the needs that people say they have) [6]. Although the health need underlies the need for health care, it does not entirely determine the need for health care. Indeed, the need for health care is commonly measured as demand, which is a subset of need, and is usually supply-induced to a significant extent [7]. More operationally defining need as the ability to benefit from health care represents an important advance [8]. This definition of need, formulated by the British health system, rests on the morbidity dimension and the effectiveness of care [9]. In addition, it enables the evaluation of specific services [8]. The capacity to benefit is dynamic and varies with the advancement of knowledge, as well as the ethical and cultural determinants of society [9].
On the other hand, the concept of health care supply includes curative and preventive services and treatments delivered by the health system, excluding informal care and social assistance [10]. Health care involves treatment, prevention, and supportive care that, either alone or as part of a comprehensive therapeutic scheme, are effective in improving, maintaining, or attenuating health impairment now, in the future, or both [10]. The demand for health care will be, then, the result of the needs perceived and expressed by the users (demand). Normative needs, on the other hand, will be determined by health professionals according to clinical recommendations and guidelines that stimulate the principal agent (health care provider) to induce a certain demand, and the effective utilization of health services. This last aspect is what we will call effective (or achieved) demand.
In Chile, the regime of Explicit Health Guarantees is a public policy established in Law 19,966 since 2004 [11], which determines for the public and private health system: access (to a specific list of benefits), timeliness (time commitment for access to health intervention benefits), quality (accreditation of providers) and financial protection (maximum co-payment ceilings) for a set of 87 health problems, 17 of which are cancers. These are prioritized and defined every three years by a joint decree of the Ministry of Health and the Ministry of Finance. For each health problem, specific conditions of access, opportunity, quality, and financial protection are established. In operation, these are expressed in a set of benefits to be delivered at specific times, in accredited institutions, free of charge in the public system, and with co-payments in the private system (Figure 1). For the public system, the use of benefits for each health intervention for each stage of cancer is registered in a national computer system, called the Information and Management System for Explicit Health Guarantees (SIGGES) of the National Health Fund, which represents 82% of the population [12]. This system requires the systematic and standardized recording of clinical and administrative data, which makes it possible to monitor compliance with deadlines and evaluate the performance of the health system. Thus, this information, among other aspects, is used to estimate the effective demand, since it represents the health needs of a population at the primary, secondary or tertiary care levels.
General flowchart of the health problems pathway of the Explicit Health Guarantees regime.
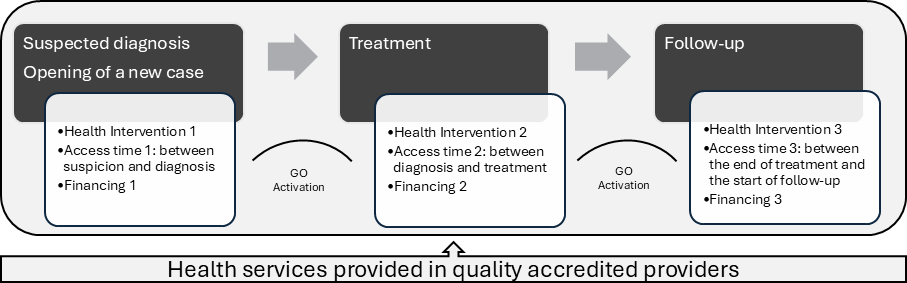
Source: Prepared by the authors of this study.
In the area of oncology, detailed knowledge of the effective demand for health services provides crucial information on the existing gaps between territories. This is useful for the annual health planning carried out in the country. Our study aims to describe the expressed demand and effective demand for health interventions associated with some prioritized cancers in the Chilean public health system between 2018 and 2022, and to compare patterns according to sex and health problem. This work is inserted in a broader project, whose purpose is the confirmation of an interuniversity research center called Centro de Prevención y Control del Cáncer (CECAN).
Methods
A comparative descriptive study was conducted, based on anonymized data from the Information and Management System of Explicit Health Guarantees, obtained from publicly accessible databases from the National Health Fund, belonging to the public system, for the period between 2018 and 2022.
Eight health problems included in the Explicit Health Guarantees regime were studied: cervical cancer, pain relief and palliative care, breast cancer, preventive cholecystectomy, gastric cancer, prostate cancer, colorectal cancer and lung cancer. The selection was based on the types included in the Cancer Prevention and Control Center, prioritized according to their prevalence, impact on mortality, and associated social and territorial inequities.
Registry of Explicit Health Guarantees
Access and timeliness of the 87 health problems included in Law 19,966 are recorded in the Information and Management System of Explicit Health Guarantees [13]. This records and activates, among other aspects, new cases, fulfillment of the guarantee of opportunity, and delay of the guarantee of opportunity (Table 1). In this study, the new cases created in the study period and their total opportunity guarantees, opportunity guarantees fulfilled and delayed opportunity guarantees were used. It is important to note that a new case may make use of more than one opportunity guarantee (timely access to health interventions), so there may be fewer cases than opportunity guarantees in a year.
For each health problem, the health interventions are different. For example, for pain relief and palliative care, only incorporate the health intervention of treatment. At the same time, for cervical cancer it includes screening, diagnostic confirmation, staging, pre-invasive cancer treatment, primary or adjuvant treatment, pre-invasive follow-up and invasive follow-up. Given this variability, a tracer health intervention was selected, corresponding to the primary treatment of each health problem, in order to allow comparison between different problems (Table 2). In the case of breast cancer, we added the guarantees of opportunity for primary treatment of the right and left breast.
Data collection
The data collected came from national guarantee reports from the Explicit Health Guarantees Information and Management System for the years 2018 to 2022 regarding new cases, opportunity guarantees fulfilled according to health intervention and delayed opportunity guarantees. The information collected represents the totality of guarantees generated at the country level, including its 29 health services and 16 regions. The records of timeliness guarantees were received, grouped by health problem, broken down by sex.
Data analysis
New cases and guarantees of opportunity fulfilled at the national level were analyzed by health problem according to sex. Rates per 1000 persons were calculated, using as a denominator the National Health Fund beneficiary population for each year, according to the explicit health guarantee of access for the cancers mentioned. In the case of pain relief, palliative care and gastric cancer, the denominator was the total population of the National Health Fund. In breast cancer, colorectal cancer and lung cancer, the analysis was made of people over 15 years of age of both sexes. For cervical cancer, persons over 15 years of age of female sex were considered. For prostate cancer, persons older than 15 years of age of male sex were reviewed. And for preventive cholecystectomy, people between 35 and 49 years of age of both sexes were studied.
To describe the delayed opportunity guarantees, a ratio was constructed to indicate how many delayed guarantees exist for every 100 new cases created, using the following formula:
From the perspective of demand, the new cases indicator indicates expressed demand from users of the public health system, while the timeliness guarantee met is an indicator of service utilization, and therefore of effective or achieved demand from these users. The indicator of delayed timeliness guarantees provides information on the unmet demand for these health problems.
To describe differences by sex, male-to-female (M:F) ratios were calculated for each of the indicators.
The study was approved by the Scientific Ethical Committee of Health Sciences of the Pontificia Universidad Católica de Chile (No. 231 005 010). This research used only secondary, pooled and unidentified data, and therefore, waiver of informed consent was authorized.
Results
An analysis of 3 783 711 new cases was performed for the health problems studied during the period between 2018 and 2022, and 3 999 312 total opportunity guarantees, being 8.2% opportunity guarantees fulfilled according to tracer interventions identified in Table 2. 36 233 delayed opportunity guarantees were analyzed. Table 3 shows the distribution of new cases, total timeliness guarantees, primary treatment timeliness guarantees by tracer intervention, and delayed timeliness guarantees by health problem and sex for the years 2018 to 2022.
It should be noted that lung cancer entered the Explicit Health Guarantees regime in 2019, so the data presented for this health problem correspond to the period from 2019 to 2022.
Behavior of new cases
In general, a decrease in the rates of new cases in 2020 is observed for most health problems, except lung cancer, which maintained an upward trend in both sexes (Figure 2).
Rates of new cases Explicit Health Guarantees/1000 beneficiaries National Health Fund, by health problem and sex, Chile, 2018 to 2022.
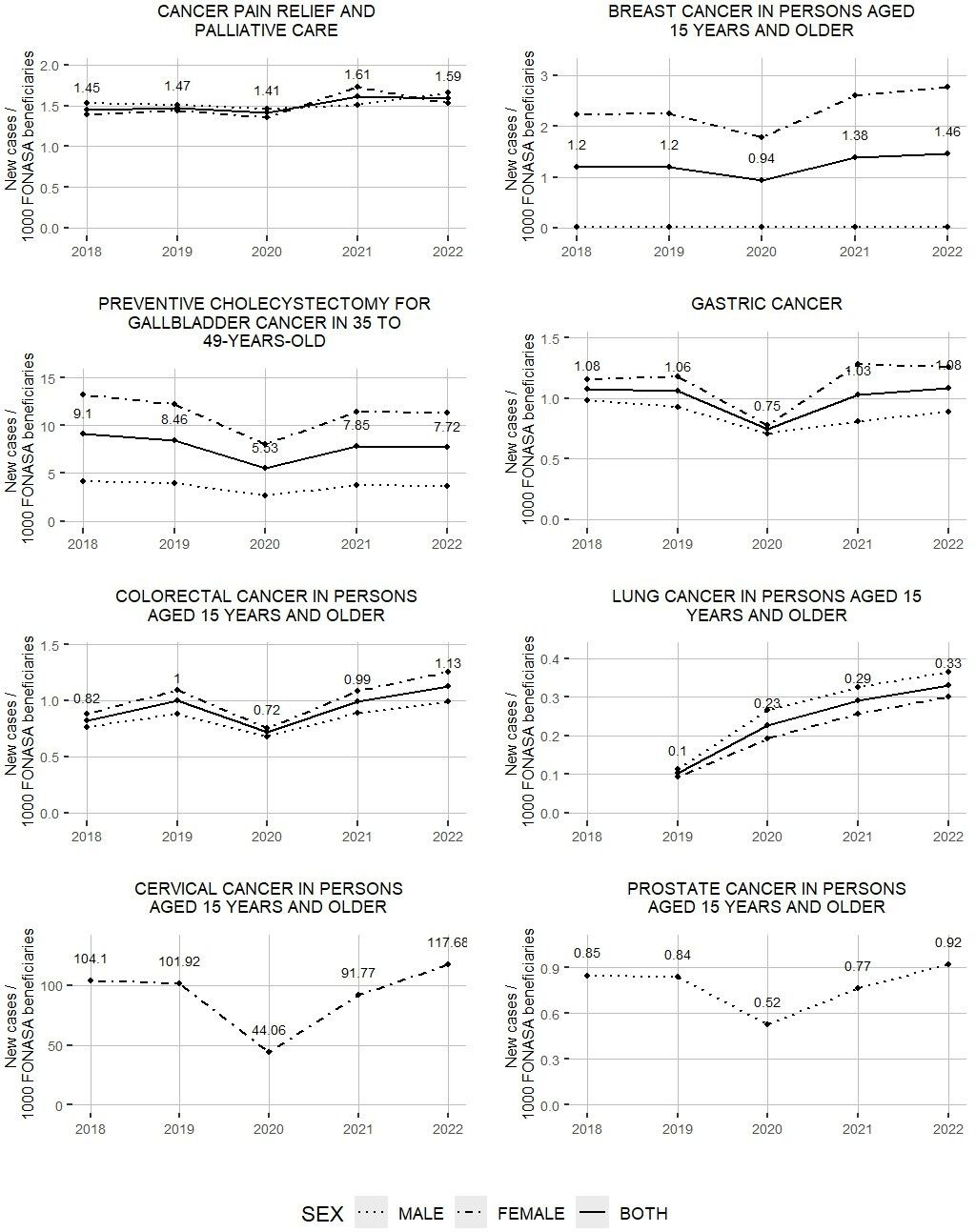
The greatest differences by sex within the same health problem are observed in breast cancer and cholecystectomy, with a male/female ratio of 0.01 and 0.3, respectively (tables 4 and 5).
For all cancers, there is a decrease in the creation of new cases in 2020, except lung cancer, which maintains an increasing trend until 2022. Regarding the post-pandemic period (2022), there is a higher number of new cases compared to the pre-pandemic years (2018 to 2019), except for preventive cholecystectomy for gallbladder cancer.
Results of the analysis of primary treatment timeliness guarantees according to tracer intervention
Figure 3 shows the rates of primary treatment timeliness guarantees by tracer intervention for each health problem. It is noteworthy that the highest rates are observed in preventive cholecystectomy, both for male and female patients. The lowest rates correspond to the primary treatment of breast cancer in men.
Rate of primary treatment opportunity guarantees according to tracer intervention/1000 National Health Fund beneficiaries by health problem and sex. Chile 2018 to 2022.
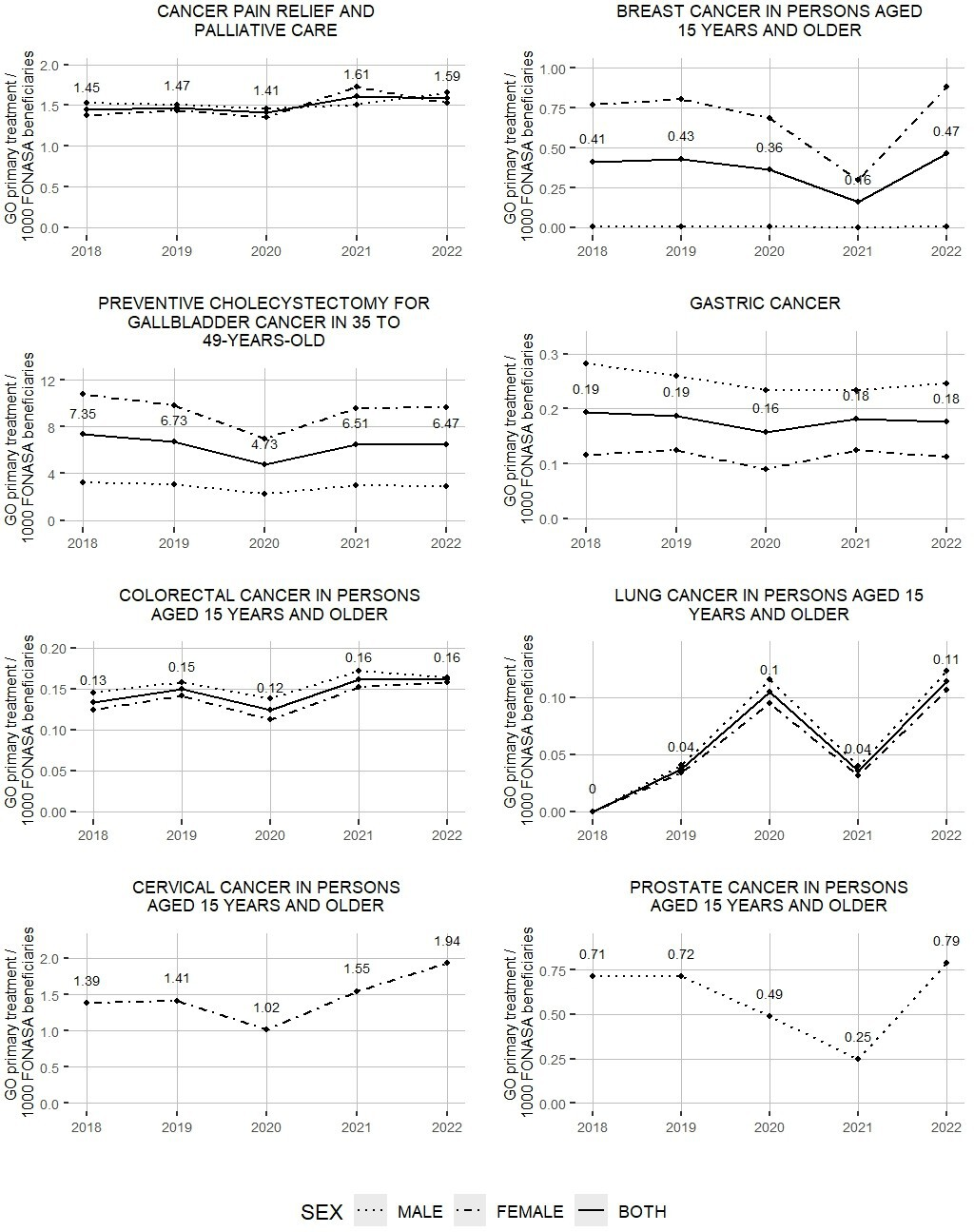
A decrease in the rates of primary treatment opportunity guaranteed by tracer intervention is observed for all cancers in 2020 and 2021. By 2022, a recovery of guarantees is observed for most health problems, which reached values higher than the pre-pandemic years (2018 and 2019), except for gastric cancer and preventive cholecystectomy.
On the other hand, it is striking that the rate of primary treatment opportunity guarantees according to tracer intervention shows a greater male predominance in colorectal and gastric cancer. To these are added lung cancer and pain relief, which have more cases admitted (Table 4).
Behavior of delayed warranties granted
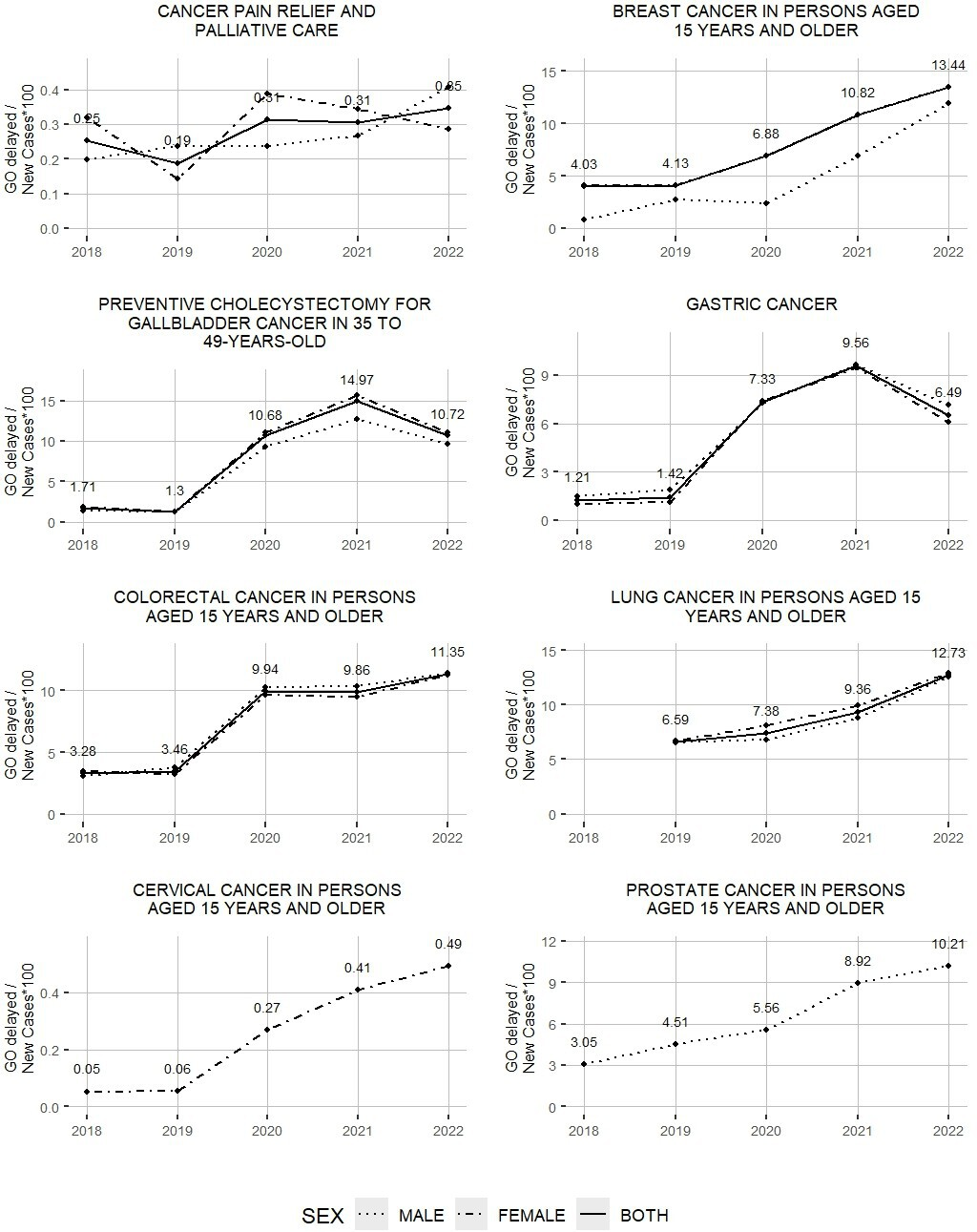
Figure 4 presents the ratio of delayed warranties per 100 new cases for each health problem and sex, between 2018 and 2022. In general, an increasing trend is observed for all health problems over the period. The lowest values are observed in pain relief, palliative care, and cervical cancer. In contrast, the highest values are presented in preventive cholecystectomy, where a maximum of 15.62 is reached in the female sex in 2021. The delayed guarantees concerning new cases show a sustained increase in cervical, colorectal, breast and lung cancer. Meanwhile, there is an increase until 2021 and a subsequent reduction in the case of gastric cancer and preventive cholecystectomy. There are no major differences by sex in this indicator, except breast cancer, where the male/female ratio varies between 0.21 and 0.89 during the period studied (Table 3).
Ratio of delayed opportunity guarantees/new cases *100, by health problem and sex. Chile 2018 to 2022.
Discussion
This study describes the behavior of the demand for health interventions for the cancers prioritized by the Center for Cancer Prevention and Control in the country, providing different perspectives that facilitated the identification of variations in the different stages of the health problems. On the one hand, the new cases created represent the total number of people who required some service (expressed demand) associated with the cancer studied, without differentiating whether these demands correspond to screening interventions, diagnostic confirmation or treatment, among others. In contrast, the guarantees of opportunity fulfilled and guarantees of opportunity of primary treatment according to the tracer intervention provide a perspective on the effective demand. Meanwhile, delayed timeliness guarantees reflect a proportion of the demand that is not satisfied.
Regarding new cases, the high rates associated with cervical cancer are explained by the fact that cases are generated from the screening stage, and all cytodiagnostic tests performed in primary care are reflected in these figures. This is independent of the fact that a negative result implies the closure of the case, or that a positive result triggers a series of additional interventions, such as diagnostic confirmation, staging and treatment, each with their respective guarantees of timeliness.
Concerning delayed guarantees of opportunity, the study developed an indicator that facilitates the comparison of the performance of the health system for various conditions, using health problems with delayed access time to benefits as a reference. An increasing trend is observed in almost all the health problems analyzed, suggesting that the system’s capacity for timely response has been exceeded. Even up to two years after the onset of the COVID-19 pandemic, differences are observed between the different health problems, but between sexes, they are smaller, except for breast cancer. In the latter, the male sex has fewer delayed assurances, which could be explained by the low number of cases, thus facilitating greater individualized follow-up. Regarding the differences observed over the years within the study period, the negative effect of the COVID-19 pandemic on both case creation and treatments granted is evident. In all the health problems studied, a decrease in new case rates is observed in 2020, except for lung cancer, whose inclusion in the Explicit Health Guarantees in 2019 could explain the increasing trend in case creation. The magnitude of the drop in new case rates varies among the different health problems studied. This suggests that the pandemic affected each health problem differently. For example, cervical cancer presented a drastic reduction in its rates from 101.92 in 2019 to 44.63 new cases per 1000 beneficiaries in 2020, which is explained by the postponement of cytodiagnostic examinations in primary care, as occurred with other screening and prevention activities [14]. In contrast, in palliative care the decrease was smaller, reflecting a lower interruption in their care.
Regarding timeliness guarantees, the selection of a primary treatment timeliness guarantee according to the tracer intervention of the different health problems allowed, to some extent, comparisons at a similar stage in the history of the disease. Thus, we observed differences between health problems when comparing sexes and over the observation period. However, the rates observed for palliative care and preventive cholecystectomy cannot be directly compared with the other problems, since they do not correspond to the primary treatment of cancer per se. Even so, it is noteworthy that in palliative care, the figures reflect the combined demand for palliative treatment not only for the cancers prioritized in this study, but also for other types of cancer. On the other hand, preventive cholecystectomy represents a preventive intervention, which differs from the specific demand associated with confirmed cancers.
The actual demand for the tracer intervention was also affected by the pandemic in a heterogeneous manner. Some problems recorded their lowest rates in 2020, while others reached their highest rates in 2021. This suggests possible differences in the responsiveness of health services, depending on the type of cancer. The results of this study reinforce the need for progress in strengthening health systems to be resilient [15], capable of maintaining their basic functionality and responding appropriately in crises.
When looking at new cases and effective demand for the tracer intervention together, we found a relationship, as cases requiring treatment are a subset of new cases. Differences were observed by sex. In gastric cancer, although the rate of new cases created is higher in the female sex throughout the period, the rate of primary treatment is consistently higher in the male sex, consistent with a higher incidence in this group [16]. This could reflect a higher suspicion of disease in females associated with a higher prevalence of gastrointestinal disorders, such as gastroesophageal reflux disease [17] or irritable bowel syndrome [18]. This would lead many of these cases to be discarded prior to diagnostic confirmation. The same occurs in the case of colorectal cancer, with a lower rate of new cases in men compared to women, but greater timely access to treatment-tracer intervention. Here we know that the incidence is slightly higher in men than in women [16]. In this case, it would be worthwhile to investigate whether women are entering earlier for diagnosis and are quickly discarded, or do not continue to the confirmation phase, or whether the men who enter mostly correspond to the disease and, therefore, go to diagnosis.
One of the main strengths of our study is its national representativeness regarding the most prevalent cancers. This was achieved through the use of a single source of information, which allowed us to have a comprehensive view of the behavior of the public health system. On the other hand, the study limits the scope of the total population by excluding the beneficiaries of the private health system, since they have another information system. Another limitation is that the information available in the records of the Explicit Health Guarantees depends directly on the accurate data entry in the system. This could lead to underreporting of cases, even if the benefits were provided. Finally, the delayed guarantee indicator (unmet demand) was constructed using the total of delayed guarantees for each health problem, and does not allow the identification of specific delays in access to the tracer intervention. Obtaining disaggregated data by type of health intervention would help to identify specific gaps and, therefore, possible intervention targets.
Conclusions
The analysis presented here provides robust information on the demand for cancer services in Chile and the response of the public system. This information favors decision-making and resource allocation under existing regulations.
In addition, future lines of research are seen in the field of analysis of the behavior of opportunity guarantees in other stages of the care process, as well as in the territorial or regional distribution and detailed demand for the benefits of health interventions, which will allow complementing these results.
The challenge now lies in strengthening the response and performance of the system in the integral approach to cancer, concretizing the advances in public policies that promote equity and efficiency in cancer care in the country.
