Estudios originales
← vista completaPublicado el 27 de abril de 2026 | http://doi.org/10.5867/medwave.2026.03.3122
Estigma y discriminación hacia personas que viven con VIH en personal de salud de un hospital público en México: estudio transversal
Stigma and discrimination toward people living with HIV among healthcare workers in a public hospital in Mexico: A cross-sectional study
Abstract
Introduction In the global context of the HIV pandemic, the biopsychosocial environment of key populations remains marked by a culture that fosters stigma and discrimination. These attitudes, based on misconceptions of what it means to live with HIV, transcend the healthcare sphere and negatively impact people’s quality of life. In Mexico, systematic documentation of this issue within hospital settings remains limited. The objective of this study was to estimate the frequency of HIV-related stigma and discrimination among healthcare personnel of a secondary-level public hospital, as well as to identify differences by job category.
Methods We conducted an observational, descriptive, cross-sectional study from February to March 2025 at a secondary-level public hospital in Cancún, Quintana Roo, Mexico. We applied the short version of the HIV stigma questionnaire proposed by Nyblade et al. A total of 316 healthcare workers from different areas participated. To identify differences in stigmatizing attitudes across professional groups and to explore potential associations between sociodemographic variables and HIV-related beliefs, descriptive statistical analyses were performed, along with non-parametric tests (Kruskal–Wallis, Mann–Whitney U, and Spearman correlations) and post hoc comparisons using Dunn’s test with Bonferroni correction.
Results A total of 22.5% of participants reported having witnessed refusal to work with people living with HIV, and 30.1% observed lower-quality care toward them. Additionally, 32.9% agreed that people living with HIV are irresponsible, and 30.4% believed they “do not care about spreading the infection.” Significant differences in stigma levels were found across occupational categories (p < 0.001). Medical assistants and interns showed higher levels of stigmatizing attitudes, while family physicians, nursing supervisors, and laboratory staff demonstrated greater empathy. Personally knowing someone living with HIV was significantly associated with greater acceptance of the right to become pregnant (p = 0.047).
Conclusions Stigma toward people living with HIV remains present in hospital environments. There is an urgent need to implement institutional training and awareness programs to reduce discriminatory attitudes and promote respect, accurate information, and empathy among all healthcare staff.
Main messages
- Stigma and discrimination against people living with HIV persist in healthcare environments, and they can compromise the quality of care.
- This study provides recent evidence on the prevalence of stigmatizing attitudes among clinical and non-clinical staff at a secondary-level public hospital in Mexico.
- Significant differences in attitudes toward people living with HIV were identified by job category, as well as associations between age and certain stigmatizing beliefs.
- The study is based on self-reported information, which may imply social desirability bias, and was conducted in a single hospital, which limits the generalizability of the results.
Introduction
The transmission of the human immunodeficiency virus (HIV) continues to pose a global biopsychosocial challenge that disproportionately affects key populations. Since the onset of the pandemic, the biomedical approach has been accompanied by a significant burden of stigma and discrimination. This burden is sustained by misconceptions about what it means to live with HIV or to belong to a group associated with this infection [1].
These misconceptions include unfounded beliefs about modes of transmission, such as the perception that everyday contact poses a risk. Added to these ideas are negative moral attributions that blame individuals for having acquired the virus. These mechanisms align with Goffman’s [2] construction of stigma. This social construct has persisted across various social spheres, particularly education, employment, and healthcare. In these settings, distorted beliefs are reproduced and sustain discriminatory practices [1].
According to the Joint United Nations Program on HIV/AIDS (UNAIDS), HIV-related stigma involves a process of devaluation that leads to negative attributions. These can manifest as discriminatory acts that undermine people’s dignity and rights, regardless of whether they are living with HIV or not [3]. Stigma can be classified as internal when it is internalized by the person, or external when it comes from social actors such as the media, family, employers, or healthcare personnel [4]. The latter type is particularly concerning when it occurs in clinical settings, as it acts as a barrier to timely diagnosis, treatment initiation, and adherence to medical services [5].
Expressions of institutional stigma can manifest through the use of derogatory language, differential treatment, non-consensual disclosure of HIV status, or discriminatory medical practices. In countries with available data, up to 21% of people living with HIV reported having been rejected from health services in the past 12 months, and in several regions, the imposition of contraceptives as a condition for accessing antiretroviral treatment has been documented, especially among women [6,7].
In Mexico, stigma toward people living with HIV has been documented across various social spheres. However, studies exploring this phenomenon among healthcare workers in secondary-level facilities remain scarce [8,9]. The persistence of negative attitudes among professionals and administrative staff, the tendency to morally blame HIV-positive individuals for contracting the virus, the desire to keep their distance or avoid contact, the use of stigmatizing language, and the perception that they pose a risk to others all contribute to perpetuating inequality and the violation of rights. Without specific data, it is difficult to develop effective awareness programs that address the realities and needs of staff providing direct care [10].
Various instruments have been designed to measure HIV-related stigma in the hospital setting. Among these, the brief questionnaire developed by Nyblade et al. stands out; it has been validated in various countries and is adaptable for both clinical and non-clinical staff [11,12,13].
In this context, the overall objective of this study was to estimate the prevalence of HIV-related stigma and discrimination among healthcare workers at a secondary-level public hospital in Cancún, Quintana Roo, Mexico. Specifically, the study aimed to:
-
Describe the frequency with which healthcare workers observe manifestations of HIV-related stigma and discrimination within the institution.
-
To describe the frequency with which healthcare workers express opinions or attitudes that reflect stigma or discrimination toward people living with HIV.
-
To compare the level of stigma and acceptance toward people living with HIV among different job categories of healthcare workers.
-
To explore the correlation between the age of healthcare workers and the presence of stigmatizing attitudes toward people living with HIV, as well as the association between gender and such attitudes.
-
To explore the correlation between different stigmatizing beliefs toward people living with HIV, in order to identify the coexistence of these attitudes within the same participant.
In addition, the possible association between personal acquaintance with someone living with HIV and the reported attitudes was explored, aiming to generate evidence to guide the design of educational and institutional interventions aimed at reducing stigma in healthcare settings.
Methods
A single-time-point, observational, descriptive, cross-sectional study was conducted between February and May 2025 at a secondary-level public hospital located in Cancún, Quintana Roo, Mexico. The study was retrospective in nature, as both the exposures and the outcomes of interest (attitudes, beliefs, and experiences related to stigma toward people living with HIV) had occurred prior to the time the questionnaire was administered. These were collected via self-report, without reviewing medical records or following up with participants.
The study population included healthcare professionals, non-clinical staff, and clinical trainees participating in patient care activities. The reference population consisted of 438 individuals listed on the institutional roster for the year 2024. This roster included active employees and undergraduate students from the fall 2024 semester. Only individuals who voluntarily agreed to participate, signed the informed consent form, and completed the questionnaire in its entirety were included. Incomplete questionnaires or those with inconsistent responses were excluded.
The sample size was estimated at 332 subjects using the finite population formula in OpenEpi version 3.0. An expected proportion (p) of 0.5 was assumed, representing the maximum possible variance when no comparable previous studies exist, a 95% confidence level (Z = 1.96), and an absolute margin of error (d) of 5%. The equation used was: n = [DEFF × N × p(1–p)] / [(d²/Z²)(N–1) + p(1–p)], where a design effect (DEFF) of 1 was considered.
Stratified sampling with proportional allocation was used. The strata were defined by the functional category of the staff (nurses, physicians, undergraduate students, and other categories, including administrative, laboratory, social work, and support staff).
Within each stratum, a systematic selection proportional to size was performed, using updated institutional lists and random numbers generated by Epidat software version 4.2.
The total population size (n = 438) was entered into Epidat, broken down into 177 nurses, 105 physicians, 115 undergraduate students, and 41 individuals in other categories. The program calculated a total sample of 332 subjects, proportional to each stratum, resulting in 122 nurses, 83 physicians, 89 undergraduate students, and 38 individuals from other categories.
Data collection utilized the Global Stigma and Discrimination Indicator Monitoring Tool developed by Nyblade et al. and validated by the Health Policy Project in 2013, based on studies conducted in China, Egypt, Kenya, Puerto Rico, and other countries. This tool compiles six of the globally approved indicators for measuring stigma and discrimination in healthcare settings and has been adapted and validated for the Latin American population [13]. The instrument consists of four sections and nine questions distributed as follows:
-
Infection control (2 questions with 6 subitems), which explores healthcare workers’ concerns about the risk of infection in their workplace.
-
Institutional environment (2 questions with 3 subitems), which examines the practices and experiences of staff who provide care to people living with HIV.
-
Institutional policies and work environment (3 questions with 4 subitems), which assess the existence of anti-discrimination policies and the availability of protective supplies.
-
Personal opinions about people living with HIV (2 questions with 4 subitems), which examine stereotypes, negative attributions, and attitudes toward the autonomy of people living with HIV.
Each item is answered using a four-point Likert scale (strongly agree, agree, disagree, strongly disagree) or a dichotomous format (yes/no), depending on the type of question. Responses were analyzed as absolute and relative frequencies. Overall scores were not calculated because the instrument is designed to describe the frequency and distribution of stigmatizing attitudes rather than to generate a total score.
For the inferential analyses, the study focused on four specific statements from the section “Personal opinions about people living with HIV,” selected because they directly aligned with the study’s objectives and reflected explicit stigmatizing beliefs that could be compared across occupational categories and sociodemographic variables. The statements analyzed were:
-
“Most people with HIV don’t care if they infect others.”
-
“People living with HIV should feel ashamed.”
-
“People become infected with HIV because they engage in irresponsible behavior.”
-
“Women living with HIV should be able to get pregnant and have children if they wish.”
The response options were ranked from the lowest to the highest degree of stigma, with increasing ordinal values assigned (1: strongly disagree, 2: disagree, 3: agree, 4: strongly agree). For the positive-content item related to the reproductive rights of people living with HIV, the order was interpreted in reverse, with higher values indicating a greater level of acceptance. This coding was used exclusively to enable ordinal comparisons between groups and to calculate mean ranks in nonparametric tests, without generating sum scores.
For the nonparametric analyses (Kruskal–Wallis and Dunn’s post hoc comparisons), the variables corresponding to stigmatizing statements were recoded in reverse, so that lower values indicated a higher degree of stigma and higher values indicated lower stigma. This recoding was performed solely to facilitate the comparative interpretation of the mean ranks, without altering the ordinal nature of the scale.
The questionnaires were administered in person by the lead researcher, without collecting any identifying information. The data were coded and entered into an Excel database, and the analysis was performed using IBM SPSS Statistics version 26. Measures of central tendency and dispersion were used for quantitative variables, and absolute and relative frequencies were used for qualitative variables, in accordance with the first and second specific objectives.
For the comparative analyses, the following were defined as independent variables: occupational category (doctors, nurses, students, and other categories), sex, and prior contact with people living with HIV.
Attitudes toward people living with HIV and experiences of discrimination were analyzed as ordinal or dichotomous dependent variables.
Due to the lack of normality in the distributions (assessed using the Shapiro-Wilk test), nonparametric tests were used: the Kruskal-Wallis test to compare more than two groups and the Mann-Whitney U test for binary comparisons. In cases of significant differences, post hoc analyses were performed using the Dunn test and the Bonferroni correction.
In addition, a heat map was created as a descriptive tool to visualize the relative ranking of stigma across occupational categories, defined as the comparative ordering of positions 1 through 15 based on the degree of agreement with the evaluated stigmatizing statements.
The diagram was constructed based on the average ranks obtained in the nonparametric tests (Kruskal-Wallis and Dunn’s post hoc comparisons with Bonferroni correction). For presentation purposes, a relative ordinal ranking was generated from these ranks and organized in ascending order of stigmatization, with 1 corresponding to the occupational category with the lowest relative level of stigma and 15 to the category with the highest for each item. This representation reflects only a comparative visual reordering and does not alter the analytical direction of the original average ranks.
The color scale was designed so that lighter shades represent a lower relative level of stigmatization and darker shades represent a higher relative level of stigmatization.
Correlations between continuous or ordinal variables (e.g., age and attitudes toward people living with HIV) were assessed using Spearman’s correlation coefficient (ρ). Results were reported as p values, with a level of statistical significance set at p < 0.05. Where appropriate, 95% confidence intervals were considered and reported in the results tables.
Comparisons and association analyses were conducted to identify differences in the expression of stigmatizing attitudes according to the occupational category of healthcare workers, as well as to explore the relationship between participants’ gender and beliefs related to HIV, in accordance with the study’s specific objectives.
This manuscript was prepared following the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist for cross-sectional observational studies to ensure transparency, comprehensiveness, and methodological quality.
Ethical Considerations
The study was approved by the institution’s local research ethics committee. All procedures were conducted in accordance with the General Health Law regarding research and the principles of the Declaration of Helsinki. Confidentiality was safeguarded at all times through the use of anonymous codes.
Results
Regarding the general characteristics of the study population, a total of 316 participants were included. The majority were women, accounting for 66.5% of the total, compared to 33.5% men. The most represented age group was 18 to 29 years old, at 37.3%, followed by the 30 to 39 age group at 29.2%, and the 40 to 49 age group at 22.4%. Only 1.5% of the participants were over 60 years old. The average age was 34.4 years (standard deviation: 11.0), with a median of 33 years and an age range of 18 to 67 years.
Regarding the highest level of education, a bachelor’s degree was the most common academic qualification, reported by 38.9% of respondents, followed by a graduate degree at 22.8%, a technical degree at 19.6%, and high school at 17.7%. In terms of religion, Catholicism predominated at 60.4%, while 13% reported practicing Christianity and 26.3% identified with other beliefs.
Regarding job categories within the hospital, 23.1% of the staff were general nurses, making this the most represented category, followed by nursing interns (15.8%) and non-resident physicians (15.5%). Nursing directors and deputy directors accounted for a smaller proportion, at 1.3% each.
Regarding length of service, 47.8% of staff had 0-5 years, 41.4% had 6-19 years, and only 10.7% had more than 20 years. The average length of service was 8.3 years (standard deviation: 7.9), with a median of 6 years and a range of 0 to 26 years and 9 months. Table 1 summarizes the general characteristics of the study population.
Regarding the influence of knowing someone close to them with HIV on the attitudes of healthcare personnel, our study reported that of the total participants, 32.6% stated that they personally knew someone who was HIV-positive. Meanwhile, 67.4% indicated they had no prior contact with someone diagnosed with HIV. Attitudes between the two groups were compared using the Mann-Whitney U test.
No statistically significant differences were found in items related to stigma toward people living with HIV in statements such as:
-
“They don’t care about spreading the infection” (U = 99 84.5; p = 0.141).
-
“They should feel ashamed” (U = 10,342.5; p = 0.305).
-
“They are irresponsible” (U = 10,716; p = 0.724).
However, a statistically significant difference was observed for the item “people living with HIV should be able to become pregnant” (U = 9,553.5; p = 0.047), where the group that did not personally know someone living with HIV expressed greater disagreement with this statement compared to those who did know someone living with HIV.
Regarding the frequency of observing discriminatory acts, 22.5% of staff reported having witnessed refusal to work with people living with HIV at least once within the hospital. Additionally, 30.1% reported observing lower-quality healthcare services for these individuals than for other patients.
In addition, 93.7% of staff believed that engaging in discriminatory behavior toward people living with HIV could lead to professional consequences, while only 3.8% indicated there would be no repercussions.
A notable finding was the frequency with which healthcare staff expressed opinions reflecting stigma and discrimination. Table 2 shows the distribution of healthcare staff responses to four statements related to stigma toward people living with HIV.
Regarding the statement “people living with HIV do not care about transmission,” 30.4% of staff expressed some degree of agreement (9.5% strongly agreed and 20.9% agreed), while 69.6% disagreed.
Regarding the statement “people living with HIV should feel ashamed,” 30.3% agreed (4.4% strongly agreed, 25.9% agreed), while the majority (69.6%) strongly disagreed.
As for the belief that “people living with HIV are irresponsible,” 32.9% agreed, while 67.1% disagreed.
Finally, regarding the statement “people living with HIV should be able to become pregnant,” 70.9% agreed, and only 29.1% disagreed.
Similarly, a weak but statistically significant negative correlation was observed between the age of healthcare workers and certain stigmatizing and discriminatory beliefs toward people living with HIV. In general, older participants showed less agreement with statements such as “people living with HIV don’t care if they infect others,” “people living with HIV should feel ashamed,” and “people living with HIV become infected because they are irresponsible.” In contrast, age was positively associated with agreement that “people living with HIV should be able to become pregnant if they wish,” reflecting greater acceptance of reproductive rights among older participants.
The correlation coefficients and their 95% confidence intervals are presented in Table 3.
Additionally, statistically significant correlations among the various belief items were analyzed to explore the coexistence of stigmatizing beliefs within the same individual. This served as a descriptive analysis to identify patterns of expressed stigma (Table 4). For example, a correlation was observed between agreeing that people living with HIV should feel ashamed and considering them irresponsible, as well as between the latter and believing that they do not care if they infect others. These findings indicate that individuals who agreed with one stigmatizing statement also tended to agree with others of similar content.
The comparison of groups by gender in terms of stigmatizing attitudes toward people living with HIV, using the Mann-Whitney U test, showed no statistically significant differences in any of the items evaluated (p > 0.05). This suggests that biological sex does not significantly influence beliefs related to transmission, shame, responsibility, or reproductive rights in this sample.
In contrast, a comparison of stigmatizing attitudes based on participants’ roles within the hospital, using the Kruskal-Wallis test, revealed statistically significant differences across all four statements evaluated:
-
Item 15.1 – “Most people with HIV don’t care if they infect others”: H = 39.358, p < 0.001.
-
Item 15.2 – “People living with HIV should feel ashamed”: H = 48.038, p < 0.001.
-
Item 15.3 – “People become infected with HIV because they engage in irresponsible behavior”: H = 67.135, p < 0.001.
-
Item 16 – “Women living with HIV should be able to become pregnant and have children if they wish”: H = 44.570, p < 0.001.
This indicates that a professional position within the hospital influences the level of stigma or acceptance toward people living with HIV.
To analyze differences between specific categories, a post hoc comparison was performed. Specifically, Dunn’s tests with Bonferroni correction were applied, revealing statistically significant differences in stigma levels based on the occupational category of healthcare workers.
For the item “Most people with HIV do not care if they infect others,” medical assistants had the lowest mean rank (R = 90.68), where R corresponds to the mean rank assigned by the nonparametric tests (Kruskal–Wallis and Dunn’s post hoc comparison with Bonferroni correction), with lower ranks indicating greater agreement with the stigmatizing statement. Statistically significant differences (p < 0.05) were identified when comparing this category with family physicians (R = 192.27), the deputy head of nursing (R = 193.67), and nursing assistants (R = 189.15), who exhibited significantly lower levels of stigma.
For the item “People living with HIV should feel ashamed,” the lowest scores were again observed among physician assistants (R = 94.41) and general nursing staff (R = 101.55). These categories differed significantly (p < 0.05) from general practitioners (R = 180.18), nursing assistants (R = 193.08), and deputy nursing supervisors (R = 190.63), who exhibited less stigmatizing attitudes.
Regarding the statement “People become infected with HIV because they engage in irresponsible behavior,” the categories with the highest levels of stigma were medical interns (R = 104.68), physician assistants (R = 106.73), and general nurses (R = 121.12). These groups showed statistically significant differences (p < 0.05) compared to family physicians (R = 184.69), general practitioners (R = 183.14), and assistant nursing supervisors (R = 195.19), who obtained the highest scores.
Finally, regarding the item “Women living with HIV should become pregnant and have children if they wish,” greater acceptance of reproductive rights was observed among family physicians (R = 177.59), laboratory technicians (R = 177.16), and assistant nursing supervisors (R = 174.92). These groups differed significantly (p < 0.05) from physician assistants (R = 101.46), medical interns (R = 120.48), and social workers (R = 127.09), who expressed greater disagreement with this statement. Figure 1 summarizes the ranking of stigma and lack of empathy by occupational category, with values representing the relative ordinal list derived from the average ranks obtained from nonparametric tests. A value of 1 indicates the lowest relative level of stigmatization, and a value of 15 indicates the highest relative level of stigmatization among the occupational categories.
Heat map: Ranking of stigma and lack of empathy by occupational category.
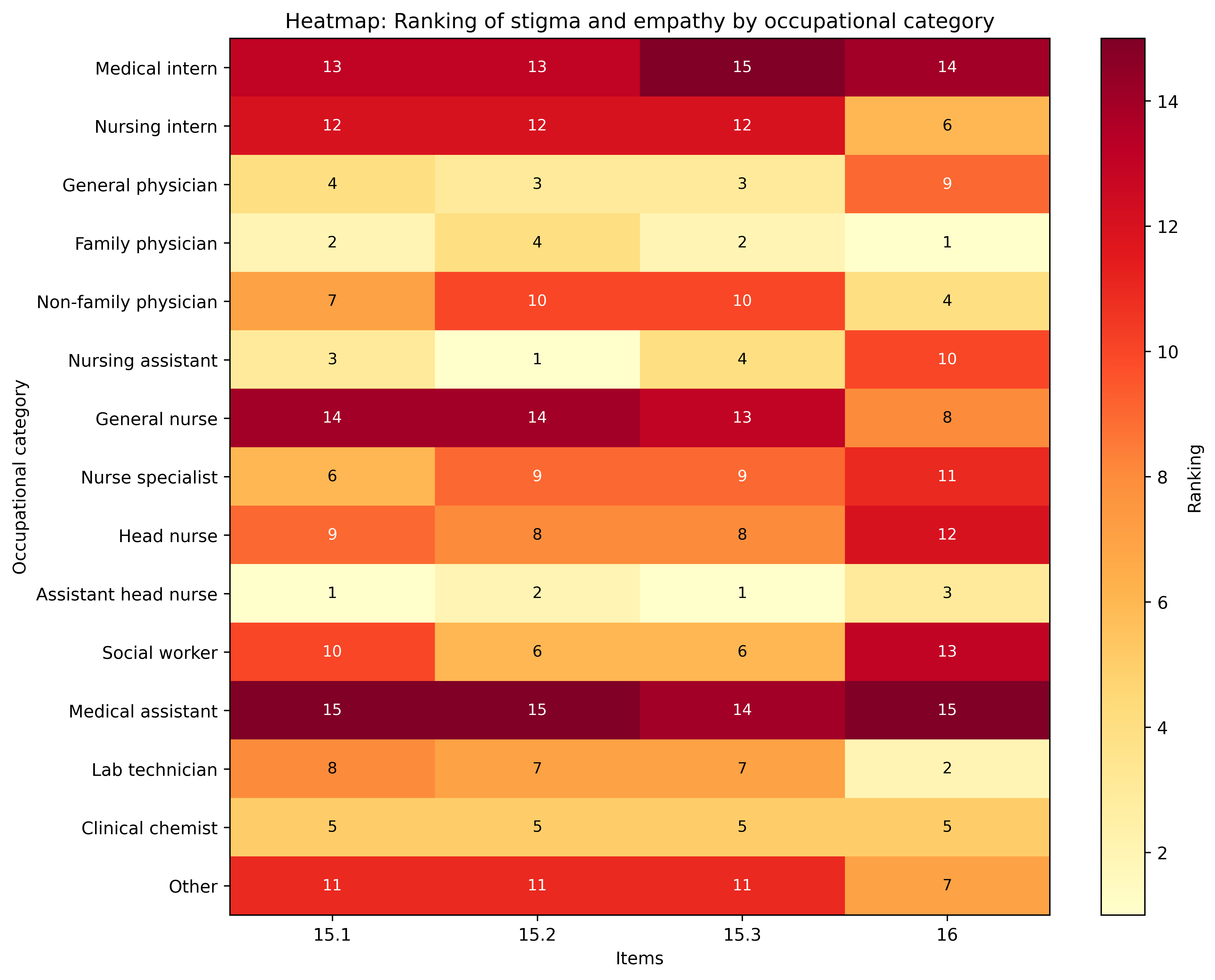
15.1 “Most people with HIV don’t care if they infect others.”
15.2 “People living with HIV should feel ashamed.”
15.3 “People become infected with HIV because they engage in irresponsible behavior.”
16 “Women living with HIV should become pregnant and have children if they wish.”
Source: Prepared by the authors based on the study results.
Discussion
In this study, 22.5% of healthcare workers reported having witnessed acts of rejection toward people living with HIV. In addition, 30.1% observed that these individuals received lower-quality care due to their HIV status. These discriminatory behaviors reflect a persistent problem in clinical practice that undermines both the quality of care and the dignity of people living with HIV.
The global AIDS update published by UNAIDS in 2024 confirms that this situation is not unique to the Mexican context. In an analysis of 42 countries, nearly 47% of the population expressed discriminatory attitudes toward people living with HIV, and one in four individuals reported facing stigma when seeking medical care for reasons unrelated to their diagnosis [14]. These data align with those reported in the 2020 edition of the same report, where up to 21% of people living with HIV were rejected or denied care in the previous year [6].
Against this international backdrop, local figures are even more concerning, as they exceed the threshold set by the 10-10-10 targets: reducing both experiences of stigma among people living with HIV and negative attitudes among healthcare workers to less than 10% [5]. With just a few months remaining until 2025—the year set to achieve these goals—the data indicate that, without immediate institutional strategies for training, awareness-raising, and cultural reform in the health sector, reversing this situation will be difficult [14].
A significant association was identified between knowing someone with an HIV diagnosis and more empathetic attitudes. Those who had such contact showed greater agreement with the right of women with HIV to become pregnant (p = 0.047). This finding can be interpreted through the contact model developed by Pettigrew and Tropp. This model posits that direct and meaningful interaction with people from marginalized groups tends to reduce prejudice, even in contexts where not all ideal conditions are met [15].
In the hospital setting, previous contact with people living with HIV appears to foster empathy and recognition of their rights, counteracting discriminatory attitudes that have historically limited their reproductive autonomy. Although this variable did not account for all the domains assessed, its impact on the recognition of rights reinforces its usefulness for designing institutional strategies. For example, UNAIDS has emphasized that the active involvement of HIV-positive individuals themselves in training and awareness-raising processes is essential for building more inclusive clinical environments with less stigmatizing burdens [5].
The analysis by job category revealed notable differences in the levels of stigma expressed. The most stigmatizing and discriminatory attitudes were concentrated among medical assistants and clinical interns, while family physicians and head nurses demonstrated more empathetic responses. Although this study did not specifically evaluate institutional hierarchy as an independent variable, the trend observed across job categories is consistent with the findings reported by Jordans et al. They found that younger, lower-ranking staff in hospitals in the Netherlands more frequently exhibited stigmatizing attitudes [16].
Similarly, the study by Hierrezuelo Rojas in Cuba found that 80% of male healthcare workers held negative beliefs about HIV, reinforcing the notion that age, gender, and professional role are key determinants in the perpetuation of stigma [9].
Studies that have used the same measurement instrument are scarce. One of the few is that of Nyblade et al., who, although they used the same baseline scale, focused on validating its general applicability in multicenter contexts, without breaking down the items individually. Even so, they reported that up to 25% of healthcare workers acknowledged having heard or used stigmatizing language toward seropositive people. This finding is consistent with our results, as 22.5% of staff reported having witnessed acts of rejection [13].
Unlike Nyblade et al., studies such as Tamayo-Zuluaga’s in Colombia used different scales but explored conceptually similar variables among medical professionals and students. In their analysis, 44.6% of participants agreed that people living with HIV were responsible for contracting the virus, and 30.2% believed they should feel guilty. These findings align with our opinion indicators, where 32.9% of staff considered seropositive individuals to be irresponsible and 30.4% believed that “they do not care about infecting others” [13,17].
Among the study’s main limitations is the potential for social desirability bias; given the sensitive nature of the topic, some participants may have responded based on what is socially acceptable rather than on their actual beliefs. Furthermore, the questionnaire did not include a specific question regarding direct care for people living with HIV, which prevented us from correlating the level of clinical contact with the reported attitudes. Although nonparametric tests were used for intergroup comparisons, it was not possible to estimate confidence intervals for the difference in medians due to limitations of the software used; therefore, the comparative results were interpreted primarily based on p values and the consistency of the observed patterns.
Overall, the results highlight the need to strengthen institutional policies to eliminate stigma in healthcare services. The negative attitudes observed among certain occupational groups, along with the perception of unequal treatment of seropositive individuals, underscore the urgency of implementing ongoing training programs that incorporate content on human rights, sexual diversity, and the latest clinical developments regarding HIV. Promoting opportunities for direct interaction between healthcare staff and people living with HIV, as well as including the latter in training and awareness-raising activities, can help reduce prejudice, foster empathy, and improve the quality of care.
Looking ahead, future research is encouraged to conduct multicenter, longitudinal studies that assess the impact of educational interventions over time and across different institutional contexts. Complementing the quantitative approach with qualitative methodologies (such as interviews or focus groups) would help elucidate the institutional and cultural mechanisms that perpetuate stigmatizing attitudes and facilitate the validation of abbreviated or adapted versions of the instrument used, which would be useful for periodically assessing the workplace climate and the quality of treatment toward seropositive individuals.
Conclusions
The findings of this study confirm that stigma and discrimination against people living with HIV persist in the healthcare setting, with negative attitudes identified among staff at various levels and significant differences observed across job categories. These results underscore the importance of strengthening institutional strategies aimed at reducing stigmatizing behaviors through ongoing training, protocol reviews, and improvements to the work environment.
Likewise, the observed association between prior contact with seropositive individuals and more favorable attitudes suggests that informed and structured awareness-raising initiatives could help reduce misconceptions, myths, and unfounded fears related to HIV. A proper understanding of the experiences and needs of people living with HIV is a central component of improving the quality of care and can be fostered through clear information, the development of communication skills, and an environment of respect and dignified treatment.
Moving toward more inclusive clinical settings depends not only on structural changes but also on training processes that foster empathy, accurate information, and an understanding of the diversity of experiences related to HIV. These findings provide useful evidence to guide future interventions and the design of institutional programs aimed at reducing stigma in healthcare settings.
