Estudios originales
← vista completaPublicado el 16 de enero de 2026 | http://doi.org/10.5867/medwave.2026.01.3153
Frecuencia de paniculitis mesentérica en población oncológica: estudio multicéntrico comparativo con grupo control
Frequency of mesenteric panniculitis in an oncologic population: A multicenter comparative study with a control group
Abstract
Introduction Mesenteric panniculitis is a rare benign entity that affects the mesentery, often detected incidentally in an imaging examination. Its association with cancer is a controversial topic. The objective of the study was to determine the frequency of this condition in a known oncological population and compare it with that of a control population.
Methods Cross-sectional, retrospective study, comparative with a control group. Patients referred for PET/CT (Positron Emission Tomography/Computed Tomography) staging for recently diagnosed cancer, who had not been treated and had no history of other previous cancer, were selected. This oncological group was separated according to type of cancer. The control group included patients referred for multiple traumatic injuries to undergo computed tomography that included the abdomen and pelvis. Control patients with a history of cancer were excluded. In both cases, the images were reviewed in search of mesenteric panniculitis.
Results Of the oncological group (1911 patients), 5.2% presented mesenteric panniculitis. The types of cancer with the highest frequency of mesenteric panniculitis were non-Hodgkin lymphoma (16.1%) and prostate cancer (12.8%), followed by multiple myeloma (6.9%), urothelial carcinoma (6.2%), cancer of the head and neck (5.3%) and pancreatic cancer (5.2%). Hodgkin lymphoma and cancers exclusive to women (breast, cervix, uterus, ovary) presented a low frequency of mesenteric panniculitis, similar to the control population. The frequency of mesenteric panniculitis in the control population (1056 individual) was 0.6%. The Odds Ratio of the oncological population vs. control for mesenteric panniculitis exposure was 9.6 (95% CI4.2249 to 22.1015, p < 0,0001).
Conclusions The frequency of mesenteric panniculitis depends on the type of cancer, and it is high in non-Hodgkin lymphoma and prostate cancer, but low and similar to that of the control population in other neoplasms.
Main messages
- Mesenteric panniculitis is a rare imaging finding, and some publications have associated it with an increased likelihood of cancer, although others have found no association with neoplasia.
- This study includes as a control group patients who underwent CT scans for trauma in the absence of previous or recent neoplasia, which is an advantage of our research compared to other publications on the subject.
- The limitations of this study are its retrospective nature, typical of cross-sectional studies; the potential diagnostic bias implied by the fact that the evaluators know whether or not the population has cancer before assessing the existence of mesenteric panniculitis; and a potential selection bias in the cancer group.
Introduction
Mesenteric panniculitis is a rare radiological diagnosis and is relatively unknown in clinical practice [1]. It consists of an increase in mesenteric fat density, with mass effect on neighboring structures, often accompanied by small lymph nodes and a peripheral pseudocapsule [1,2]. It is usually an incidental finding on computed tomography or other abdominal imaging tests (ultrasound, magnetic resonance imaging) referred for the study of various clinical conditions [1]. By definition, it is a benign entity, which may be idiopathic or associated with inflammatory conditions [3] or neoplastic processes [1]. Its most common clinical manifestation is abdominal pain [1,4,5,6,7].
The prevalence of mesenteric panniculitis in the general population appears to be close to 0.6% [6,8] when studies use representative samples or samples close to a control or "normal" population. However, numerous publications report higher frequencies, with upper ranges reaching 6.9% [9,10,11]. These differences could be explained by various biases when selecting the study population. One of the most obvious is to search among CT scans performed in clinical practice, which, of course, includes examinations performed on "sick" patients who consult for a condition that may include abdominal pain, inflammatory states, recent surgery, or the concomitant existence of cancer.
On the other hand, the frequency of mesenteric panniculitis in the oncological population appears to range from 5.4% to 10.3% [10,11]. In a recent case series published by our group, we reported a 5.3% prevalence of this pathology in the newly diagnosed oncological population [12].
Although it appears that the observed frequency of mesenteric panniculitis is higher in cancer patients than in individuals with no history of neoplasia, the direct association between this condition and cancer remains controversial [1,13]. Daskalogiannaki et al. report that 69% of individuals with mesenteric panniculitis detected by computed tomography had concomitant cancer [6]. A follow-up study by van Putte-Katier reports that 48% of patients with this disease had coexisting cancer, and that an additional 14% developed it during a five-year follow-up [7]. Similarly, Buchwald et al. found cancer in 43% of patients with mesenteric panniculitis [14]. However, there are also sufficient case series that do not find significant differences in cancer prevalence between patients with and without mesenteric panniculitis [8,9,15].
Biases in sample collection could partially explain the significant differences in results between these studies. In some cases, the control population includes symptomatic patients who visit a health center for a CT scan or even patients hospitalized for inflammatory or neoplastic conditions. On the other hand, most studies aim to demonstrate or rule out the presence of cancer in patients with mesenteric panniculitis, which would undoubtedly require thorough laboratory testing, imaging, and invasive procedures (endoscopy, biopsies), which are absent from the methodology of most publications. Some authors, in their attempt to unify the information in a meta-analysis, have only been able to conclude that the studies are too heterogeneous to be unified and obtain accurate information, deducing that no study reliably proves the association between cancer and mesenteric panniculitis [16,17] (but they have not proven the opposite either). Furthermore, the vast majority of studies do not include a comparative control population. This is a significant limitation if one wishes to establish an association between mesenteric panniculitis and any other medical condition. This limitation extends to our previous publication [12], which is why we now wanted to add a comparative control group, in addition to increasing the oncology group. This allowed us to double the sample size.
The objective of this study was to determine the frequency of mesenteric panniculitis in the oncology population and compare it with a control population without cancer. The aim was to establish whether any type of cancer is more associated with mesenteric panniculitis than others. We also sought to determine whether F-18 fluorodeoxyglucose (FDG) increased uptake visible on positron emission tomography/computed tomography (PET/CT) in mesenteric panniculitis was associated with any specific type of cancer.
Methods
This is a retrospective, multicenter, cross-sectional study with a comparative control group. We compared the frequency of mesenteric panniculitis in a newly diagnosed cancer population, consisting of groups with different histologically confirmed types of cancer, and a control population without cancer.
Cancer patients
From the PET/CT database of Clínica Las Condes (Center 1), positron emission tomography/computed tomography scans performed on cancer patients referred for staging studies were retrospectively selected. The sample covered the period between 2008 and 2023, including both pediatric and adult populations.
At the time of the scans, the clinical background, medical history, and histology of all patients were available. These data were recorded in the examination report and in the attached documents, which were reviewed retrospectively in all cases. Only patients with a confirmed histological diagnosis who had not received treatment for their underlying pathology, i.e., without surgery, radiotherapy, chemotherapy, or immunotherapy, were considered. Patients with a history of previous cancer or synchronous or metachronous malignant tumors were excluded.
All patients included had histological studies consistent with cancer. Cases of complex histology were agreed upon by two expert pathologists and simultaneously sent to a reference center for histopathological analysis (CDM Fletcher, MD, Brigham and Women’s Hospital).
Positron emission tomography/computed tomography scans plus contrast-enhanced whole-body scans were performed using GE Discovery ST 16-channel or GE Discovery MI 64-channel equipment, following intravenous injection of the radiotracer, which corresponded to F18-FDG (0.1-0.14 mCi/kg), Ga68-PSMA, F18-PSMA, or Ga68-DOTATATE, depending on the reference diagnosis. After PET/CT acquisition, a whole-body computed tomography scan (brain, neck, chest, abdomen, and pelvis) with intravenous iodinated contrast was performed in all patients, with venous-phase imaging throughout the body and arterial-phase imaging in the abdomen.
All contrast-enhanced full-body CT scans were reviewed by two radiologists specializing in oncological imaging and a highly experienced nuclear medicine physician for mesenteric panniculitis. This was defined by consensus according to the following imaging criteria [1,2]:
-
Increased density of adipose tissue at the root of the mesentery.
-
Increased volume of mesenteric adipose tissue with mass effect on adjacent structures.
-
Presence of small mesenteric nodules or lymph nodes.
Although a dense pseudocapsule or halo sign was present in most cases, it was not a condition for inclusion in this study.
The frequency of mesenteric panniculitis was estimated according to the type of cancer.
A third radiologist specializing in the abdomen/pelvis reviewed all cases with mesenteric panniculitis and a group of doubtful cases. The latter were discussed among the three observers, who reached a consensus.
The intensity of radiotracer uptake in mesenteric panniculitis nodules and the liver was quantified only in studies performed with F18-FDG, using the standardized uptake value maximum (SUVmax). Mesenteric panniculitis was considered "hyper-uptake"hypermetabolic if it had an SUVmax equal to or greater than that of the liver.
In studies using radiotracers other than F18-FDG, no comparison with liver uptake was made, given the high variability in hepatic uptake across radiotracers (Ga68-PSMA, F18-PSMA, Ga60-DOTATATE). For this reason, only a visual assessment of mesenteric panniculitis uptake was performed, without calculating SUVmax.
Control group
For the selection of the control group, all CT scans performed on patients referred for trauma or polytrauma at the San Juan de Dios Hospital (Center 2) between 2016 and 2023 were reviewed. These patients often undergo a variety of CT scans to look for traumatic injuries to the trunk or extremities. Abdominal-pelvic CT scans were retrospectively reviewed for mesenteric panniculitis, and brain, neck, and chest CT scans were reviewed for incidental tumors or cancer.
Patients with a history of treated cancer, those with cancer undergoing treatment, and those whose images at the time of trauma showed tumors or suspicious lesions for cancer were excluded. Patients with findings consistent with mesenteric panniculitis were specifically investigated for a history of such symptoms by reviewing the institution’s medical records. Consequently, those with a history of cancer and recent surgery were excluded from the study.
Computed tomography scans were performed on a Siemens Somatom Definition AS 64. Intravenous iodinated contrast medium was injected in all examinations.
Computed tomography scans of the brain, neck, chest, abdomen, and pelvis were reviewed by two trained observers for mesenteric panniculitis, and cases with signs of this pathology were recorded according to the same criteria used for the oncology group. Positive and doubtful cases were reviewed by two expert subspecialist radiologists and a third radiologist subspecialist in the abdomen/pelvis area, who reached a consensus on the results.
The frequency of mesenteric panniculitis was estimated in the entire patient group. Because the control group was smaller and significantly younger and more male than the oncology group, it was not possible to perform a paired analysis with the oncology group.
Statistical analysis
The frequency of mesenteric panniculitis was calculated for each group and expressed as a percentage. The Chi-square test was used to compare the frequency of mesenteric panniculitis between the oncology and control groups, using MedCalc software version 18.10.2 (MedCalc Software Ltd., Seoul, Republic of Korea). The odds ratio was calculated using the same software.
Ethics
The authors obtained approval from the Ethics Committees of both centers involved in the study (Las Condes Clinic and San Juan de Dios Hospital). In addition, we obtained informed consent from the patients and/or subjects referred to in the article, or, failing that, a waiver from the Ethics Committee.
Results
Cancer patients
Eighteen patients with incidental synchronous tumors detected by positron emission tomography/computed tomography were excluded from the oncology group. That is, two coexisting neoplasms in different organs of the body. The final oncology population consisted of 1911 patients (median age 63 years, range 3 to 94 years, 55% men).
After the three observers reached a consensus on the presence of mesenteric panniculitis, only one case remained in dispute. This was a case of prostate cancer that was evaluated as positive by two observers and doubtful by a third, which was ultimately considered to be mesenteric panniculitis. The prevalence of mesenteric panniculitis in the oncology group was 5.2% (100/1911). The most common neoplasm associated with this pathology was non-Hodgkin lymphoma, with 16.1% (34/211), 56% of which were of the follicular subtype. One of these cases is shown in Figure 1.
42-year-old man with grade I-II follicular NHL with Ki67: 20%. On the left, axial CT slices and PET/CT fusion show signs of mesenteric panniculitis with hyperactive lymph nodes (SUVmax 7.3), which are more active than the liver (SUVmax 2.7). The central image shows CT demonstrating increased mesenteric fat density and volume. Right image: MIP of PET showing only mesenteric involvement.
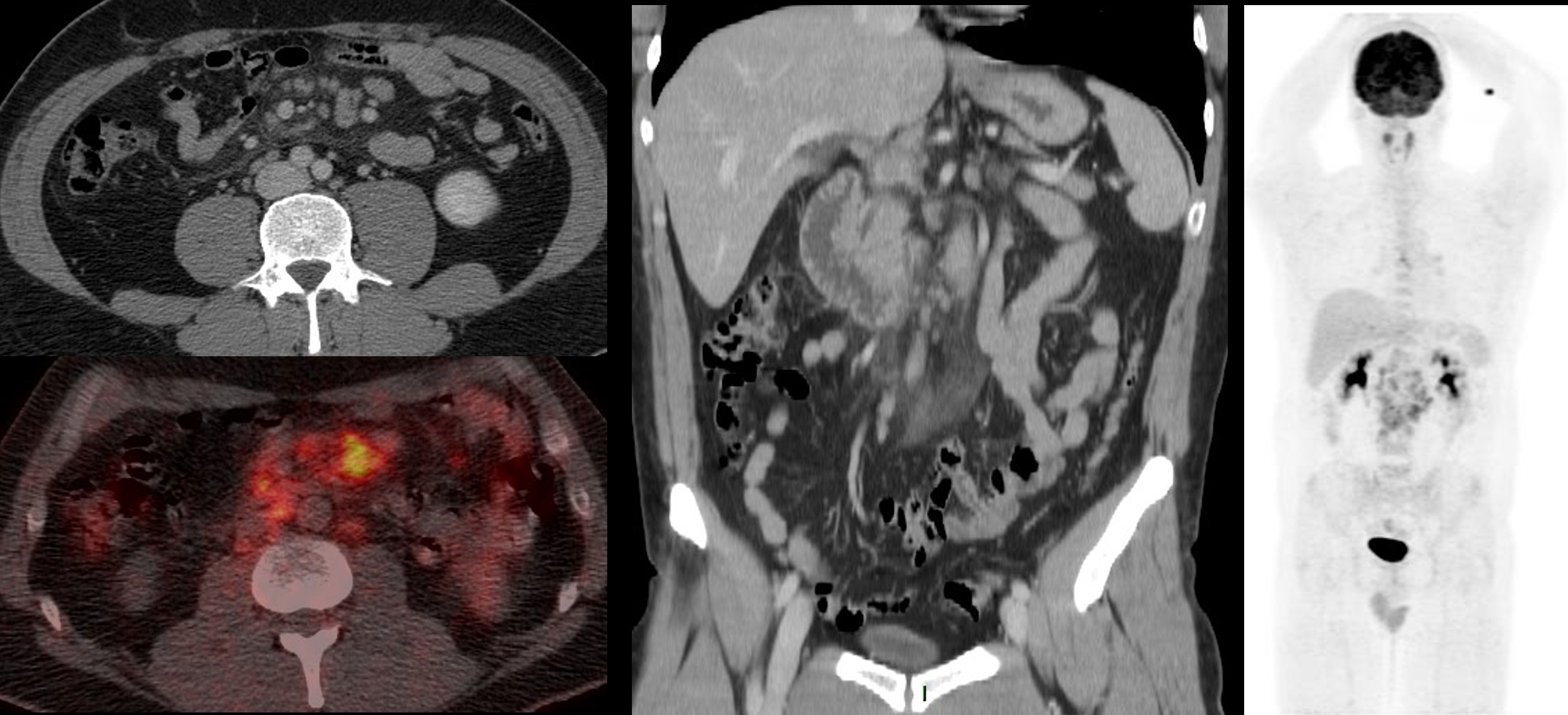
Source: Prepared by the authors based on a case included in the case series.
It was followed in frequency by prostate adenocarcinoma with 12.8% (20/156), multiple myeloma with 6.9% (5/72), urothelial carcinomas with 6.2% (4/65), head and neck carcinomas with 5.3% (6/114), pancreatic adenocarcinoma with 5.2% (6/115), sarcomas with 4.3% (2/46), and others with 3% or less of mesenteric panniculitis (see Table 1).
By grouping cancer types according to the frequency of mesenteric panniculitis, three subgroups were arbitrarily formed: oncological group I with a high frequency of mesenteric panniculitis (equal to or greater than 10%), oncological group II with an intermediate frequency (equal to or greater than 4% but less than 10%), and oncological group III with low frequency (less than 4%), as shown in Table 1 and Figure 2.
Box-and-whisker plot showing the frequency of mesenteric panniculitis by cancer group and in control individuals.
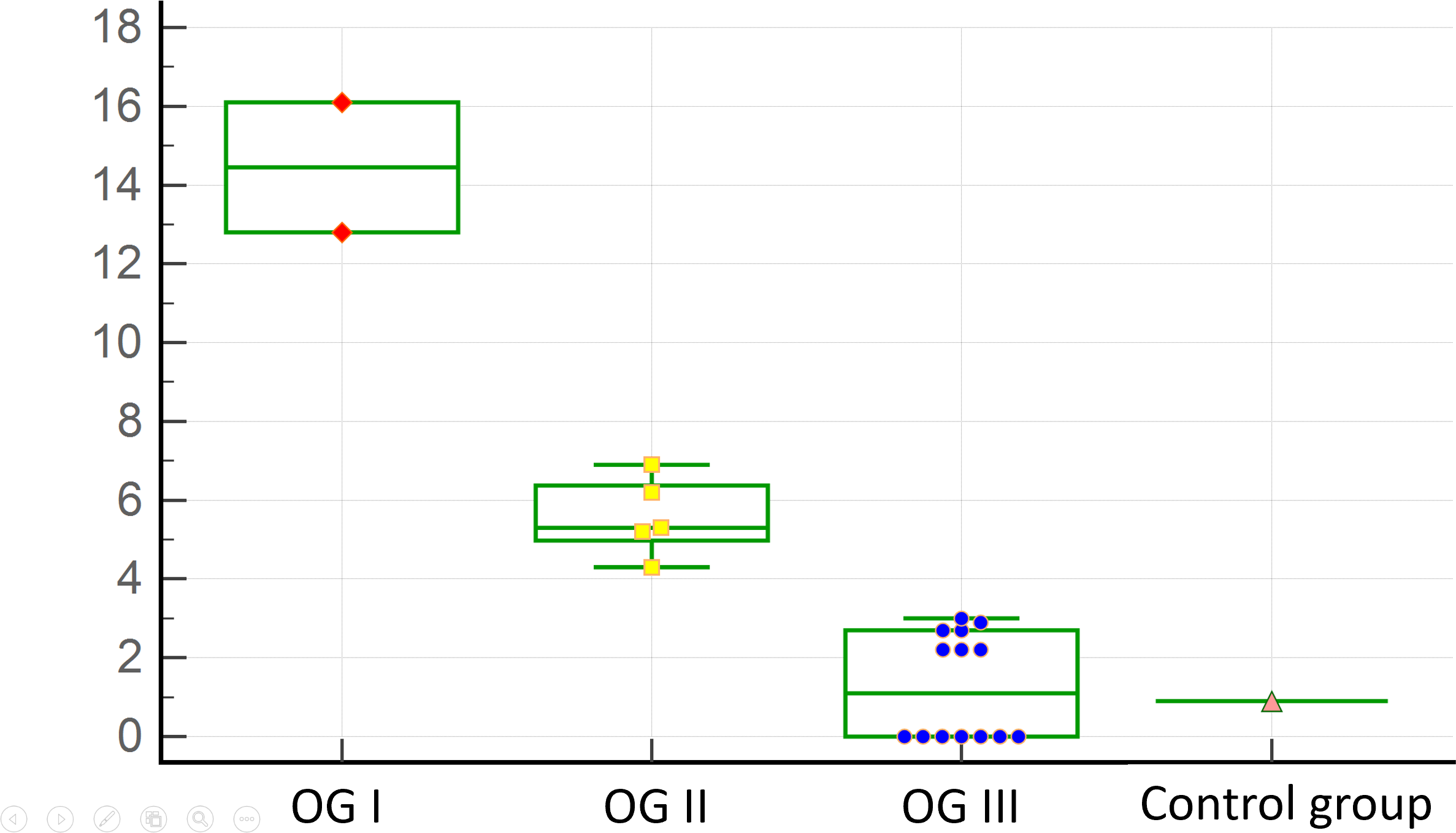
Source: Prepared by the authors based on the study results.
Some types of cancer did not present mesenteric panniculitis, such as Hodgkin’s lymphoma, cervical cancer, endometrial cancer, esophageal cancer, cholangiocarcinoma, gallbladder cancer, and hepatocellular carcinoma, which were included in the low-frequency mesenteric panniculitis group (oncological group III).
The only patients who showed increased uptake of F18-FDG in mesenteric panniculitis were those with non-Hodgkin lymphoma. In fact, half of the patients with non-Hodgkin lymphoma who presented with mesenteric panniculitis had nodules/lymph nodes with SUVmax equal to or greater than that of the liver (SUVmax: 10.9 ± 8.6). In the other half of patients with non-Hodgkin lymphoma, and in the rest of the oncology population, mesenteric panniculitis did not show significant FDG uptake (SUVmax: 1.3 ± 0.7). Liver uptake in the total patient group was 3.0 ± 0.8 SUVmax.
In the visual assessment, mesenteric panniculitis did not show significant uptake of Ga68/F18-PSMA or Ga68-DOTATATE in the population with prostate cancer and neuroendocrine neoplasms, respectively.
Control patients
Eight patients in the control group were excluded because computed tomography detected a tumor lesion suspicious for cancer (lung, gastric, colorectal). The final "control" population consisted of 1056 patients (median age 45 years, range 15 to 97 years, 72% men), of whom 6 had mesenteric panniculitis (0.6%).
Comparison of the cancer population versus control
Patients with cancer (n = 1911) had a significantly higher frequency (p < 0.0001) of mesenteric panniculitis than the control population (n = 1056) when using a proportion comparison test (chi-square).
The odds ratio for "mesenteric panniculitis exposure" in the cancer population versus the control population was 9.6 (95% confidence interval 4.2249 to 22.1015; p < 0.0001), as shown in Table 2.
Discussion
In our study, we found a high frequency of mesenteric panniculitis in certain neoplasms, such as non-Hodgkin lymphoma and prostate cancer, along with a low frequency in other types of cancer, with a refined sample of oncology patients. In the sample, special care was taken to exclude post-surgical causes of mesenteric panniculitis and patients with other synchronous and/or metachronous neoplasms. The use of positron emission tomography/computed tomography in all oncological cases would increase diagnostic accuracy by allowing the exclusion of patients with inflammatory pathology or incidentally detected synchronous cancer.
The high frequency of mesenteric panniculitis in non-Hodgkin lymphoma reported in our study is consistent with the literature, especially the findings of Ehrenpreis et al. [16] and Scheer et al. [11], including the apparent predominance of the follicular histological subtype. On the other hand, non-Hodgkin lymphoma was the only neoplasm that showed significant FDG increased uptake in the lymph nodes within mesenteric panniculitis. This would further increase the diagnostic suspicion of non-Hodgkin lymphoma in cases of hypermetabolic mesenteric panniculitis.
The high prevalence of mesenteric panniculitis in prostate cancer does not fare as well, as its relationship with this pathology has been mentioned by only a few authors [7,18]. However, the articles reviewed do not indicate whether patients with mesenteric panniculitis underwent any targeted screening for its detection.
The assertion that a patient with mesenteric panniculitis does not have a coexisting neoplasm warrants separate analysis, as it would require more than computed tomography to confirm. Given that we know that non-Hodgkin lymphoma and prostate cancer are the neoplasms most associated with mesenteric panniculitis in this sample, we must admit that both are difficult to diagnose by computed tomography. Prostate cancer is often invisible on computed tomography [18], and its diagnosis by imaging requires specific tests such as prostate magnetic resonance imaging and positron emission tomography/computed tomography with PSMA [19], in addition to blood tests such as prostate-specific membrane antigen. The same is true for extranodal lymphoma involvement, especially in the bone marrow, which is highly frequent in non-Hodgkin lymphoma and is only detectable with bone marrow magnetic resonance imaging or 18F-FDG positron emission tomography/computed tomography [20]. In other words, with computed tomography, we can see the patient’s mesenteric panniculitis but cannot rule out these coexisting neoplasms with certainty. The same can occur with small carcinomas of the head and neck and the intestinal tract. The lower computed tomography (CT) capacity compared with PET/CT for detecting these neoplasms may constitute a technological bias in previous publications. At the same time, it corresponds to a comparative advantage of our study.
One noteworthy aspect is that in our case series, the incidence of colorectal cancer in the population with mesenteric panniculitis was quite low. This finding is inconsistent with the literature, which reports that this neoplasm ranks among the most common [8,9,10].
The low frequency of mesenteric panniculitis in female cancers in this sample warrants special mention, consistent with the literature [11,16]. This low occurrence of mesenteric panniculitis seems clear for neoplasms such as breast cancer, which has a sufficient sample size (185 individuals), but must be qualified in cases with smaller samples: ovarian cancer (46 patients), endometrial cancer (48 patients), and cervical cancer (47 patients).
The prevalence of mesenteric panniculitis in the control group of our case series was 0.6%, similar to that described by Daskalogiannaki et al. [6] and Gögebakan et al. [8], confirming that it is a rare condition. Given that it appears particularly difficult to estimate the frequency of mesenteric panniculitis in this specific group, we attempted to refine the sample as much as possible, excluding patients with known oncological pathology or recent abdominal surgery. The inclusion of only patients who consulted for trauma and the verification of the patients' oncological history pointed in this direction.
A comparison of cancer patients with a matched control population remains pending. This was not possible due to the smaller number of cases and controls and the substantial heterogeneity in gender and age within the cancer population, which was considerably older and had a significantly higher proportion of females than the control group.
One limitation of our study is its retrospective design, which is typical of cross-sectional studies. However, the relatively high number of cancer patients analyzed ensures adequate validity of the results. Another disadvantage is the potential diagnostic bias introduced by evaluators knowing whether the population is oncological or non-oncological before assessing for mesenteric panniculitis. Given the study design, this is not easy to avoid. However, the consensus of three expert observers in all cases would partially avoid this problem. There is also potential selection bias in the cancer group, simply because they all underwent PET/CT. This test has its indications and, in theory, is not performed across the board on all cancer patients.
The association between mesenteric panniculitis and abdominal pain was not evaluated in this study, as obtaining this data would probably require a prospective study design that would allow a patient survey to be conducted at the same time as the imaging examination.
When selecting the control population, we sought to minimize selection bias, which is a likely cause of overestimation of mesenteric panniculitis when including unknown (or known but unconsidered) oncology patients. To this end, we only included patients who underwent CT scans due to trauma, while also reviewing their medical histories to ensure the absence of previous neoplasia that had been treated or was currently being treated. This constitutes an advantage of our study over other publications on the subject. However, even with these safeguards in place, it cannot be guaranteed that this group represents a control population.
Another advantage is the use of odds ratios, which are rarely used in the literature to analyze the association between mesenteric panniculitis and cancer. This estimator quantifies our results and makes them more objective. An odds ratio of 9.6 can be interpreted as meaning that the odds of having cancer, compared to not having it, are 9.6 times those observed in patients without mesenteric panniculitis. However, it should be clarified that the use of the odds ratio in our cross-sectional study refers to a measure of prevalence ratios in this context (cross-sectional), not of future relative risk.
Conclusions
Mesenteric panniculitis is a rare entity in the healthy population and varies in frequency in cancer patients, being more common in some neoplasms than in others. The malignancies most associated with this pathology in our sample were non-Hodgkin’s lymphoma and prostate cancer. In addition, mesenteric panniculitis with avid F18-FDG uptake would be highly suggestive of non-Hodgkin lymphoma. On the other hand, a significant number of cancer types showed no clear association with mesenteric panniculitis. However, in several neoplastic groups, the sample size needs to be increased to confirm this. Ideally, this should be done through a comparative study against a matched control group.
Likewise, mesenteric panniculitis could serve as a "marker" for detecting certain neoplasms. In addition, the incidental finding of this entity should require a reasonable and prudent effort to rule out certain malignancies, including a targeted and limited search for the specific neoplasms most commonly associated with it.
A prospective follow-up study of patients with mesenteric panniculitis will be needed in the future to determine its true implications in the development of neoplasms and to estimate the relative risk of their occurrence. This is proposed as a research idea for this area.’
