Estudios originales
← vista completaPublicado el 8 de mayo de 2026 | http://doi.org/10.5867/medwave.2026.04.3176
Adaptación cultural al shawi y análisis psicométrico del Patient Health Questionnaire en adultos del Alto Amazonas, Perú
Cultural adaptation to Shawi and psychometric analysis of the Patient Health Questionnaire (PHQ-9) in adults from the Alto Amazonas, Peru
Abstract
Introduction Depression is currently one of the most impactful mental health conditions worldwide, with more than 280 million reported cases. However, there is a critical lack of data on Indigenous populations due to language barriers and the absence of culturally adapted assessment tools, limiting timely diagnosis and appropriate care. The aim of this work is to culturally and linguistically adapt the Patient Health Questionnaire-9 (PHQ-9) into the Shawi language and to evaluate its psychometric properties among Indigenous adults in Alto Amazonas, Peru.
Methods A rigorous cultural adaptation process was carried out, including translation by bilingual experts and back-translation. Validation involved expert technical review and a pilot phase conducted within the participating community. Content validity was assessed using Aiken’s V coefficient as a statistical indicator. The internal structure was evaluated using confirmatory factor analysis and structural equation modeling.
Results The sample consisted of 432 members of the Shawi community. The instrument showed excellent content validity (V = 0.90 to 1.00). Confirmatory factor analysis supported a unidimensional model with good fit (comparative fit index: 0.98; root mean square error of approximation: 0.06) and adequate internal consistency (α = 0.80; ω = 0.81). In addition, invariance of the PHQ-9 was demonstrated across age, sex, educational level, and marital status, supporting its applicability across different population subgroups.
Conclusions The Shawi version of the Patient Health Questionnaire-9 has proven to be a reliable and valid tool for detecting depressive symptoms in this Indigenous population. This advancement represents a significant contribution to reducing mental health disparities by facilitating culturally appropriate diagnoses and improving care in historically underserved Amazonian communities.
Main messages
- The study addresses the shortage of culturally adapted depression assessment tools for Indigenous peoples, a problem exacerbated by language barriers.
- Its contribution lies in being the first adaptation of the PHQ-9 into the Shawi language through a methodological process.
- A major limitation is that the findings are not yet generalizable.
- Despite this, the Shawi PHQ-9 exhibits excellent psychometric properties.
Introduction
Depression is a chronic, high-risk disorder that can lead to suicide as well as significant social and cognitive impairment [1,2]. The World Health Organization (WHO) indicates that depression manifests, among other symptoms, as persistent sadness, loss of interest in daily activities, feelings of guilt, and a negative self-perception [3], and these are often linked to psychosocial factors [4]. Globally, it is estimated that 5% of the population—that is, approximately 280 million people—suffers from depression [5,6]. In addition, the health crisis caused by COVID-19 led to an approximate 25% increase in the frequency of this disorder [5]. In Latin America, 3.35% of the population is affected by depression [7]. This situation makes it the leading cause associated with disability in the regional context, with people living in poverty being the most vulnerable [8,9]. Regarding Indigenous populations, a prevalence of anxiety of 14% has been reported in India [10]. In Bangladesh, 59.2% of individuals have high levels of anxiety and depression [11]. In Panama, 32% of the population reported depression and 22.9% suicidal ideation [12]. Similarly, in Brazil, the prevalence of depression is 7%, being higher among women [13].
In the Peruvian Amazon, the Instituto Especializado de Salud Mental “Honorio Delgado–Hideyo Noguchi” conducted a study that found that 43.2% of the population perceived having a mental health problem, while 85.7% had not received adequate treatment [14]. This situation more severely affects vulnerable population groups, such as Indigenous communities, women, and children [15]. This highlights the barriers they face in accessing mental health care in an equitable and intercultural manner [16].
In this sense, depression is an affective disorder characterized by persistent distress, anhedonia, and fatigue. These are accompanied by sleep and appetite disturbances, which severely limit daily functioning. It is a multifactorial condition with interrelated biological, psychological, and social roots, which explains its diverse clinical presentations, including marked self-criticism and persistent feelings of inadequacy and low self-esteem [17,18,19].
One of the most widely used instruments for detecting depressive symptoms is the Patient Health Questionnaire-9 (PHQ-9), which has been adapted and validated in multiple cultural contexts. For example, in South Korea, it was validated in 6022 adult participants, showing high reliability (α = 0.88) and a good balance between sensitivity (89.9%) and specificity (84.1%) [20]. In Mexico, the psychometric properties of the PHQ-9 were established in 163 patients with a history of cancer, yielding an α coefficient of 0.896 and explaining 54.8% of the variance [21]. In Latin America, it was adapted in Chile in 245 adolescents aged 15 to 19 years, obtaining an α of 0.78 (95% confidence interval: 0.71 to 0.84) [22]. In Peru, it was validated in 30 449 adults, achieving an internal consistency of α = 0.87 and ω = 0.87, with item-test correlations ranging from 0.62 to 0.77 [23]. Regarding cultural adaptations, the PHQ-9 has been adapted into three varieties of Quechua—Cuzco-Collao, Chanca, and Central Quechua—showing high reliability (α = 0.87 to 0.91; ω = 0.83 to 0.88) in 970 adult speakers [24]. It has also been adapted into Bolivian Quechua, with 397 adult participants, demonstrating reliability coefficients of α = 0.87 to 0.88 and ω = 0.87 to 0.89 [25].
Despite advances in intercultural psychological assessment, Amazonian communities such as the Shawi—who have more than 21 000 active speakers across the Paranapura, Carhuapanas, and Huallaga river basins, located between Loreto and San Martín—still lack psychometric instruments adapted to their cultural and linguistic context that allow for valid and reliable identification of depressive symptoms [26]. This population, which self-identifies as Shawi, maintains a vital language belonging to the Cahuapana family, with regional dialectal diversity [27]. However, the absence of culturally appropriate diagnostic tools limits timely access to mental health care, potentially leading to underdiagnosis and undertreatment of depression. In Peru, the prevalence of clinically relevant depressive symptoms in adults reaches 6.4% and may rise to 35% in individuals with chronic diseases [28,29]. All of this reinforces the need for inclusive adaptations in Indigenous populations.
From a theoretical perspective, this research contributes to the field of cross-cultural psychology and applied psychometrics by strengthening the understanding of how depression manifests in culturally diverse contexts. This is particularly evident in the methodological aspect, where the linguistic adaptation and psychometric validation of the PHQ-9 in the Shawi language are developed in accordance with rigorous criteria for semantic and conceptual equivalence. In doing so, the utility of this widely used instrument at the international level is extended [30,31], making it accessible to communities where Spanish is not the primary language. This version of the questionnaire will allow the detection of depressive symptoms through a brief, accessible, and easy-to-administer instrument for local personnel. Thus, it contributes to reducing inequalities in access to mental health care and to ensuring the right of Indigenous peoples to receive psychological care that respects their culture and language.
Overall, this study represents an important step toward more equitable and intercultural mental health care within the Peruvian health system. Therefore, the aim of this research is to obtain a culturally adapted and translated Shawi version of the Patient Health Questionnaire-9. Additionally, it seeks to examine evidence of validity based on internal structure through confirmatory factor analysis, as well as the reliability of the scale and measurement invariance in Indigenous Shawi adults from Alto Amazonas, Peru.
Methods
Design and context
This study followed a quantitative, cross-sectional, instrumental design [32]. This is because it aims to develop the translation and adaptation of the Patient Health Questionnaire-9 into the Shawi Indigenous language and to analyze the instrument’s internal structure, validity, reliability, and measurement invariance across versions of the adapted instrument [33].
Participants
Sample size was calculated using a digital tool specifically designed for studies employing structural equation modeling, following the criteria proposed by Kim [34]. A statistical power of 90%, a significance level of 5%, and an anticipated attrition rate of 10% were established, resulting in a minimum required sample size of 313 participants. A total of 432 individuals were recruited through non-probability convenience sampling. Data collection was conducted in Shawi communities in the province of Alto Amazonas, including the districts of Yurimaguas and Balsapuerto, as well as their surrounding rural settlements in the Loreto region, Peru.
Participants aged 18 to 65 years, of both sexes, bilingual in Spanish and Shawi, with some level of formal education, and who voluntarily provided informed consent were included. A total of 18 participants were excluded due to partially completed surveys or health conditions that prevented coherent responses.
Instrument
The Patient Health Questionnaire-9 was used, originally developed by Spitzer, Kroenke, and Williams [35] and validated in the Peruvian population [23]. This unidimensional self-report Likert-type scale consists of nine items based on the diagnostic criteria for major depression in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR), and assesses depressive symptoms over the past two weeks.
The PHQ-9 includes four response options (0: not at all; 1: several days; 2: more than half the days; 3: nearly every day), with total scores ranging from 0 to 27. Regarding its psychometric properties, a standard confirmatory factor analysis showed that a unidimensional model presented adequate fit (comparative fit index = 0.93; root mean square error of approximation = 0.09; standardized root mean square residual = 0.04). In multigroup confirmatory factor analysis, all progressively constrained models showed Δ comparative fit index < 0.01 in most demographic groups. Reliability is high, with a coefficient α = 0.87, indicating strong internal consistency (α = 0.87; ω = 0.87).
Procedures
The study began with the cultural and linguistic adaptation of the PHQ-9 into the Shawi language, following the methodological guidelines proposed by Beaton et al. [36], which are widely used for the translation and validation of instruments in intercultural contexts. This approach ensures semantic, idiomatic, conceptual, and experiential equivalence between the original and adapted versions, preserving construct validity across culturally diverse populations [36,37,38].
Initially, two translators fluent in Peruvian Spanish and Shawi independently performed forward translations into Shawi. Subsequently, translators and researchers met to review discrepancies and produce a single reconciled version. The next step involved back-translation from Shawi into Spanish by two independent translators. A panel of experts then reviewed semantic and theoretical differences between the original Spanish version and the translated Shawi version. After addressing discrepancies and incorporating suggestions, the final Shawi version of the PHQ-9 was approved.
The next step consisted of evaluating the Shawi PHQ-9 by seven experts, including five psychologists, one physician, and one intercultural education specialist. All had at least one year of experience working with Shawi individuals presenting mental health conditions such as depression, and all were fluent in both Spanish and Shawi. Experts assessed the items and response options using a validation form based on clarity, representativeness, and relevance. Open-ended questions were also included to gather recommendations regarding cultural and semantic equivalence, particularly for expressions without direct equivalents in Shawi, such as “depression” or “hopelessness,” and for response options that became unclear when translated into a Likert scale format.
After each expert provided feedback, the research team incorporated the revisions and presented the improved version to each expert individually. Additional suggestions were reviewed and implemented iteratively until consensus approval was reached.
Subsequently, a focus group was conducted with 50 bilingual participants from the Shawi community who had previously provided informed consent. This stage aimed to assess the instrument’s clarity and comprehensibility. A moderator (a psychologist fluent in Shawi) asked participants to read and respond to the Shawi version of the PHQ-9. After completion, participants were asked:
-
Did you encounter any words that were unclear or unfamiliar?
-
Did you find any questions unclear or difficult to understand?
Participants shared their feedback and recommendations, which the research team recorded in writing. This final stage resulted in a Shawi version of the PHQ-9 ready for psychometric evaluation.
Three bilingual interviewers visited communities in Alto Amazonas province, including rural settlements in the districts of Yurimaguas and Balsapuerto. Interviewers were previously trained in face-to-face data collection using paper-based surveys. After obtaining permission from local authorities (e.g., community leaders), interviewers conducted door-to-door visits accompanied by at least one local community member to foster trust.
Initially, the interviewer introduced the study and explained the informed consent process. Only those who voluntarily agreed to participate completed the survey. Data collection took place over a three-month period, from September to December 2024.
Statistical analysis
First, based on a quantitative evaluation by seven experts using a 0 to 3 rating scale for each item, Aiken’s V coefficient was calculated, with values > 0.70 considered acceptable for relevance, representativeness, and clarity.
Subsequently, descriptive analysis included absolute and relative frequencies for categorical variables and means with standard deviations for continuous variables. Item distribution was assessed using skewness and kurtosis coefficients, with values within ± 1.5 considered indicative of normality [39]. To assess internal consistency, Cronbach’s α and McDonald’s ω coefficients were calculated, with values ≥ 0.70 considered acceptable [40].
Model validation was performed using confirmatory factor analysis with the Weighted Least Squares Mean and Variance Adjusted (WLSMV) estimator, appropriate for ordinal Likert-type items. Standardized factor loadings (β) and model fit indices were reported. Adequate fit was defined as χ²/df < 3, comparative fit index and Tucker–Lewis index > 0.90, and root mean square error of approximation and standardized root mean square residual ≤ 0.08 [41]. A multigroup confirmatory factor analysis was also conducted to assess measurement invariance across demographic characteristics, evaluating configural, metric, and scalar levels of equivalence [42,43]. Finally, a structural equation model using the Weighted Least Squares Mean and Variance Adjusted estimator was applied to analyze relationships between items and latent factors of the adapted PHQ-9, reporting factor loadings, explained variance, and standard errors. All analyses were performed using Jamovi (version 2.5) and JASP (version 0.18).
Ethical considerations
The study was reviewed and approved by the Ethics Committee of the Graduate School of Universidad Peruana Unión (Report No. 2024-CEEPG-00139). In addition, the study adhered to the ethical principles established in the Declaration of Helsinki for research involving human subjects [44]. This included respect for autonomy through informed consent, data confidentiality to protect participant privacy, and the principle of justice by minimizing risks to participants.
Results
Based on the recommendations from experts and the focus group regarding certain words that do not exist in Shawi, such as “depression,” the term na’kun sehterawe was suggested, which translates into Spanish as “estar muy triste” (“to feel very sad”). Experts recommended this term because, in Indigenous communities, profound sadness has been associated with the diagnosis of depression [45]. Similarly, the expression “hopeless” was adapted as ku nanpichinachin kankanterawe, which in Spanish means “sin ganas de vivir” (“without the will to live”). Finally, regarding the response options that became confusing when translated and did not reflect a Likert scale, both experts and focus group participants agreed on the following scale:
-
Kahpa: not at all.
-
A’nahken taweri: some days.
-
Wa’ki taweriru’sake: several days.
-
Nani taweri: nearly every day.
From a sample of 432 adults from Shawi communities, the majority (252; 58.3%) were aged 18 to 29 years. Additionally, 246 (56.9%) were female, 197 (45.6%) had primary education, 269 (62.3%) were single, divorced, or widowed, and 404 (93.5%) lived in rural areas of the Peruvian Amazon (Table 1).
The descriptive analysis of the Shawi PHQ-9 items showed means ranging from 0.71 (item 9) to 0.98 (item 3), with standard deviations ranging from 0.72 to 1.08. Skewness and kurtosis indicated a normal distribution (± 1.5), while Aiken’s V coefficient for relevance, representativeness, and clarity was excellent across all items, with values ranging from 0.90 to 1.00 and 95% confidence intervals within the acceptable range (0.79 to 1.00). This supports the instrument’s content validity in this population (Table 2).
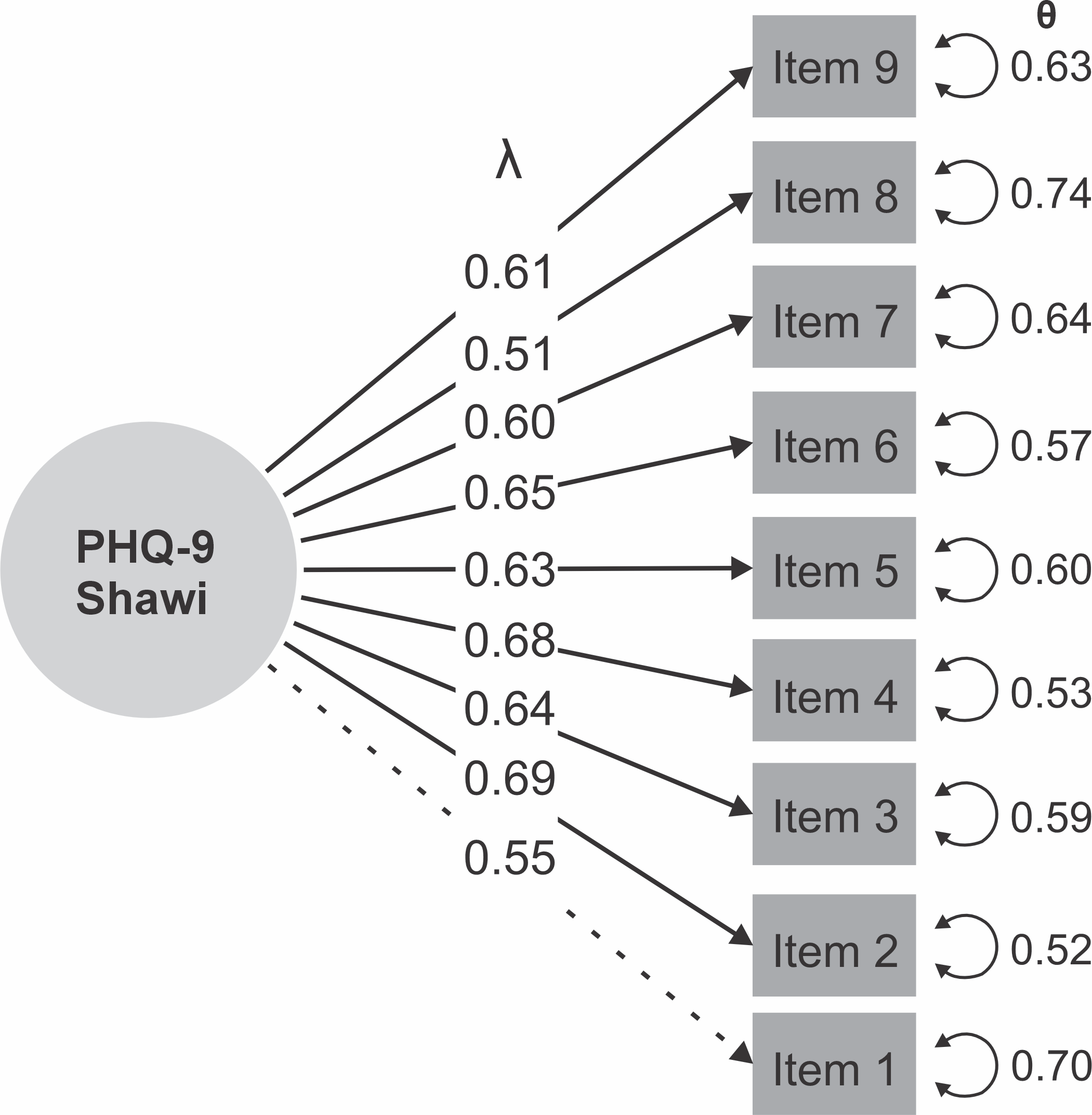
In the structural analysis, a unidimensional model showed adequate goodness-of-fit indices (comparative fit index = 0.98; Tucker–Lewis index = 0.80; standardized root mean square residual = 0.062; root mean square error of approximation = 0.06) (Table 3). Additionally, the Shawi PHQ-9 items showed factor loadings ranging from λ = 0.51 (item 8) to λ = 0.69 (item 2), all above 0.40, which are considered acceptable (Figure 1).
Graphical model of the factor structure of the Shawi PHQ-9. PHQ-9: Patient Health Questionnaire-9; λ: standardized factor loadings; θ: residual variance (unique error) of a latent variable.
Internal consistency of the adapted version, assessed using Cronbach’s α (α = 0.80) and McDonald’s ω (ω = 0.81), showed optimal values (Table 3).
The Shawi PHQ-9 demonstrated measurement invariance across age, sex, educational level, and marital status, as goodness-of-fit indices (comparative fit index) for all levels of invariance were > 0.95 and RMSEA values were ≤ 0.07. Likewise, absolute values of Δ comparative fit index and/or Δ RMSEA were < 0.01 (Table 4).
Discussion
This study represents the first effort to culturally and linguistically adapt and psychometrically validate the PHQ-9 in the Shawi language, an Indigenous Amazonian population in Peru. The sample, composed predominantly of young adults aged 18 to 29 years (58.3%), women (56.9%), and individuals with primary education (45.6%), reflects the typical demographic structure of rural communities [24,25,46]. These data underscore the importance of having validated psychological tools in contexts where Spanish is not the primary language and where access to mental healthcare services is limited [47].
The cultural adaptation process, which involved expert review and a focus group of adult speakers from the community, showed that depression is not primarily conceptualized as a biomedical category as in Hispanic or Western contexts, but rather as a relational and morally situated experience, expressed through local notions such as nukun kankantawa (deep sadness) and nukun kankantawa taweri (persistent thoughts of death). This aligns with anthropological literature indicating that mental disorders are often expressed using culturally specific terms [48]. The adaptation of response options into a temporal scale understandable for the Shawi population reinforces the semantic validity of the instrument and avoids distortions inherent to Western Likert scales [49]. Overall, these findings support the need to integrate anthropological approaches into the assessment of depression in Indigenous contexts, enabling differentiation between culturally grounded meanings of suffering and epidemiological realities, thereby avoiding overdiagnosis and promoting culturally safe interpretations.
The adapted version showed no sufficient evidence to reject the assumption of normality across all items, with means ranging from 0.71 to 0.98, supporting the use of factor analysis. Aiken’s V coefficient for relevance, representativeness, and clarity was excellent (0.90 to 1.00) [50], with adequate confidence intervals, confirming the content validity of the adapted instrument [51]. This finding supports the rigorous translation and back-translation process, ensuring semantic and conceptual equivalence, as recommended by international standards in cross-cultural research [36].
Confirmatory factor analysis demonstrated that the Shawi version of the PHQ-9 retains a unidimensional structure consistent with the original model [35]. Similar findings have been reported in nationally representative samples [52] and in systematic reviews that provide robust evidence of unidimensionality [53,54,55]. Model fit indices were satisfactory (comparative fit index = 0.98; Tucker–Lewis index = 0.98; root mean square error of approximation = 0.06), and all standardized factor loadings ranged from λ = 0.51 to 0.69, confirming that each item contributes significantly to the depression construct. Internal consistency was also adequate (α = 0.80; ω = 0.81), comparable to values reported in other cultural and linguistic contexts [20,24,25,56,57].
Measurement invariance confirmed that the Shawi PHQ-9 is invariant at the configural, metric, strong, and strict levels across age, sex, educational level, and marital status. Fit indices (comparative fit index > 0.95; root mean square error of approximation ≤ 0.07) and differences (Δ comparative fit index and Δ root mean square error of approximation < 0.01) met the recommended criteria for assuming factorial equivalence. These criteria follow the guidelines established by Putnick and Bornstein [58] for supporting measurement invariance. These findings are consistent with previous research reporting PHQ-9 invariance across different cultural contexts, including studies by Harry et al. [59] in Latin American populations and Kim et al. [20] in Asian settings. This supports the use of the instrument to compare groups within the Shawi population without measurement bias due to sociodemographic variables. This is particularly important in intercultural contexts, as highlighted by Boer et al. [60] and Huey et al. [61]. Consequently, these results reinforce the utility of the Shawi PHQ-9 as a reliable and valid tool for detecting depressive symptoms in Indigenous populations, facilitating the identification of care needs without cultural or demographic distortions.
The validation of the PHQ-9 in the Shawi language represents a significant advancement for mental health care in Indigenous communities of the Peruvian Amazon. The adaptation of psychological instruments to specific cultural contexts not only improves the identification of depressive symptoms but also enables more personalized and culturally sensitive clinical interventions [62,63]. Previous studies have emphasized the importance of validated tools in Indigenous languages to strengthen the integration of mental health into public health services and promote a more inclusive and equitable approach [16,64].
Compared with previous validation studies of the PHQ-9 in Peru, such as those by Remes et al. [19] and in Quechua-speaking populations [24], this research contributes valuable insights to Indigenous mental health by addressing the linguistic and cultural specificities of the Shawi community. The findings suggest that the adapted PHQ-9 is a reliable and valid tool for detecting depressive disorders across diverse cultural and linguistic settings, consistent with adaptations in Australian Indigenous populations [65] and rural African communities [66].
The validation of the PHQ-9 in Shawi has important implications for public policy and mental health programs in rural areas of Peru. The availability of a validated and culturally sensitive tool enables health professionals to more accurately detect depression, reduce underdiagnosis, and ensure appropriate treatment. Furthermore, it supports the development of care approaches that respect cultural diversity within these communities [24,25,67].
Among the study limitations, the sample size should be noted. Although confirmatory factor analysis and fit indices support the instrument’s structure, larger samples, particularly within age subgroups, could provide more robust estimates and enable more detailed invariance analyses. Additionally, administering the PHQ-9 in a survey context may have influenced responses, as social factors and scale comprehension can affect response validity [30]. Moreover, the absence of a clinical reference interview prevented the estimation of sensitivity, specificity, and diagnostic cut-off points for the Shawi population, which should be addressed in future studies. Another limitation is that the adaptation was based on the Spanish version rather than the original language. However, the Spanish version assesses the same DSM-5 criteria for major depression as the original [23,25,35]. Nonetheless, this may have affected the conceptual and semantic equivalence of some items, and results should therefore be interpreted with caution. Additionally, the study included bilingual participants rather than monolingual Shawi speakers. This is because Shawi is primarily an oral language, and most native speakers do not read or write in it, limiting the use of written instruments. Future research should consider audio-based versions with AI-supported response recording systems to assess monolingual populations.
A key strength of the study is the rigorous linguistic and cultural adaptation process of the PHQ-9 into Shawi. The inclusion of native translators and the use of back-translation ensured conceptual equivalence, a critical aspect in cross-cultural research [36]. Furthermore, its application in a community with limited access to psychological assessment contributes significantly to mental health equity in Indigenous populations.
Conclusions
The adaptation of the PHQ-9 into the Shawi language is reliable and valid for assessing depressive symptoms in this Indigenous population. This is supported by the instrument’s internal consistency (Cronbach’s α = 0.80; McDonald’s ω = 0.81) and confirmatory factor analysis, which demonstrated unidimensional validity with good fit indices (comparative fit index > 0.95; root mean square error of approximation ≤ 0.07). This represents a significant advancement in mental health care for Indigenous communities in the Peruvian Amazon.
Training health personnel in the use of the Shawi-language instrument is recommended to ensure proper interpretation of results. Finally, the adapted PHQ-9 should be implemented in both clinical and community settings as part of screening programs within intercultural health services.
