Estudios originales
← vista completaPublicado el 24 de junio de 2026 | http://doi.org/10.5867/medwave.2026.05.3196
Estudio exploratorio para identificar facilitadores y barreras en implementación de una aplicación de comunicación multiplataforma para tamizaje prehospitalario y seguimiento de transferencia en accidente vascular cerebral agudo
Exploratory study to identify facilitators and barriers for implementing a multiplatform communication app for prehospital screening and transfer follow-up in acute stroke
Abstract
Introduction Early-stage stroke management is a complex, time-sensitive healthcare process requiring coordinated action and prompt decision-making. JOIN is a multiplatform communication application that streamlines and facilitates healthcare coordination. The objective of the study was to explore the process of implementing and using JOIN across a network of hospitals within the South-East Metropolitan Health Service to identify facilitators, barriers, and perceptions of its impact.
Methods A multiple-case study design was conducted based on a qualitative research framework. The process evaluation used purposive sampling to capture relevant experiences across diverse hospital contexts. Semi-structured interviews were conducted with individuals involved in implementing and using JOIN. Coding was performed using ATLAS.ti software, based on thematic analysis and an iterative procedure. The analysis was based on the components of process normalization theory and focused on evaluating key implementation outcomes.
Results During the interviews (n = 8), some of the facilitators identified ongoing training and the presence of a leader as factors in the use of JOIN. Overload of the emergency care system, resistance to change, and difficulties with technology use were among the barriers identified. Although the application's benefits (user-friendly and intuitive) were recognized, the implementation process posed significant challenges. Fidelity and feasibility were the most difficult implementation outcomes to achieve.
Conclusions The process evaluation highlights the importance of ongoing training and leadership for implementing new interventions within emergency healthcare settings. Furthermore, it emphasized the importance of achieving a comprehensive understanding of the context to improve implementation.
Main messages
- Acute stroke is a time-sensitive condition that requires effective coordination of emergency systems and rapid decision-making.
- JOIN is a multiplatform communication app that streamlines patient care efficiently by simplifying communication and collaboration among physicians.
- This study provides a contextualized understanding of the facilitators and barriers to care during the initial phase of stroke.
- Limitations of this evaluation include the uneven participation of primary care and prehospital personnel compared to neurologists at the involved hospitals, which restricts a comprehensive understanding of the healthcare network’s functioning; and the fact that it is not possible to assess its impact on clinical indicators or performance, as the results focus on participants’ perceptions regarding the use of JOIN.
Introduction
Stroke affects millions of people and is the second leading cause of death worldwide [1]. In Chile, according to the Global Burden of Disease (GBD) report, this condition was associated with 9.1% of all deaths in 2017 and was the third most common cause of combined death and disability [2]. Various strategies have been implemented in our country to reduce stroke-related morbidity and mortality. One of these has been the inclusion of ischemic stroke and subarachnoid hemorrhage secondary to ruptured cerebral aneurysms in the Explicit Health Guarantees (GES) program, ensuring diagnostic confirmation and treatment for these patients [3].
Clinically suspected stroke requires a prompt and thorough evaluation and diagnostic process in order to receive effective medical treatment that reduces the risk of disability and death [3]. In its initial (or hyperacute) stage, this management involves a complex, urgent healthcare process structured into a series of steps that require effective time management, rapid decision-making, and coordination among various healthcare providers [4]. International clinical guidelines recommend a stroke assessment system by first responders, advanced notification of a potential patient on route to ensure adequate resource mobilization, and an organized protocol in the emergency department [5]. Given that this is a time-sensitive medical emergency, all actions must be directed toward diagnostic evaluation and treatment and initiated within the first few hours after symptom onset to preserve the integrity of brain tissue that has not yet sustained irreversible damage [3]. Intravenous thrombolysis (the standard therapeutic intervention for patients with acute ischemic stroke) has been shown to be safe and effective [5,6]. However, in Chile, its use is still limited to a few hospitals. The Ministry of Health has established maximum time limits for the actions to be taken in cases of this condition, which are counted from the patient’s arrival at the emergency department. One of these is performing a computed tomography (CT) scan within 25 minutes and initiating intravenous thrombolysis within 60 minutes [7]. Additionally, the Stroke Action Plan was proposed, which outlines guidelines for comprehensive care. Its emphasis is on incorporating the concept of a neurological emergency and activating the stroke code, or “code stroke,” to facilitate timely diagnosis, access to treatment therapies, and the reorganization of hospitals into functional treatment units, among other measures [8].
Given that the primary barrier to timely treatment is the speed with which the prehospital system responds to suspected acute stroke, various initiatives have been implemented over the years. One such initiative is the use of technology [4,9,10,11]. The growing development of smartphones and artificial intelligence has demonstrated its potential to transform every step of care for this condition. Moreover, this has been one of the conditions that has benefited most from the digital health revolution [11]. An example of this is JOIN (Allm Inc.), a multi-platform communication app approved by the Food and Drug Administration (FDA) and used internationally, which streamlines and facilitates the coordination of healthcare [12]. Its main features include a customizable assessment and triage system, efficient patient transfer, and a proprietary transmission system for sending data sets. This enables fast, real-time information sharing while complying with all security standards. Among its most notable features are the creation and tracking of clinical cases, the sending and receiving of medical images in DICOM (Digital Imaging and Communications in Medicine) format [13] through integration with visual systems, and the option to organize group conversations with defined roles to facilitate shared decision-making [12].
The use of JOIN in the care of patients with acute stroke was incorporated as part of an academic research initiative at three public hospitals within the South-East Metropolitan Health Service in Santiago, the capital of Chile, in collaboration with their respective emergency primary care services. Our main objective was to determine the impact of implementing the “stroke code” using JOIN on standard performance measures (percentage of codes activated with and without JOIN, differences in door-to-needle and door-to-groin times, and percentage of thrombolysis coverage). In this context, we decided to conduct a process evaluation, which involves a systematic analysis of how an intervention is implemented. We aimed to explore the implementation mechanism of this application, identify facilitators, barriers, and perceptions of its impact on usage.
Methods
Study design
We conducted an exploratory multiple-case study design [14], following a qualitative paradigm. For this research, we defined the case study as the process of implementing and using the JOIN application for prehospital screening and follow-up of acute stroke by professionals and coordinators from hospitals and primary emergency care services within the South-East Metropolitan Health Service, based on process normalization theory [15]. We used the Standards for Reporting Qualitative Research (SRQR) [16] (online supplementary table 1).
Regarding the context in which this process evaluation was conducted, it was part of an academic research initiative that implemented JOIN Triage and JOIN across three public hospitals within the South-East Metropolitan Health Service of Santiago, Chile, as well as their corresponding primary emergency care centers. The study was carried out between December 25th, 2023, and March 9th, 2025. Secondary and/or tertiary care hospitals within the South-East Metropolitan Health Service that could benefit from this application during hyperacute medical care were considered for inclusion. Hospitals were selected based on serving a large population, having a high clinical workload, and requiring both internal and external coordination services. Eligible centers also needed to have emergency departments, on-call vascular neurologists, dedicated stroke units, and the capability to perform cerebral reperfusion procedures. Primary emergency care centers within the same health service network were also included. The study population consisted of adult patients with a probable diagnosis of acute ischemic stroke treated within this network, presenting within 4.5 hours of symptom onset and eligible for thrombolysis and/or thrombectomy within an extended therapeutic window of up to 24 hours. The JOIN application was made available to all healthcare professionals involved in the hyperacute management of this condition. Multiple training sessions were conducted before and throughout the implementation period. Hospitals were ensured to have the necessary technical infrastructure to properly use JOIN. An open communication channel between users and the technical support team was maintained throughout the implementation period to provide ongoing assistance. Training on data entry and the use of clinical scales was delivered continuously during the study. In addition, the local initiative leaders at each hospital met weekly to review progress and address day-to-day operational challenges. The flowchart of data collection for the process evaluation is presented in online supplementary figure 1.
The process evaluation, an essential and systematic component of the design and assessment of complex interventions, was guided by the Medical Research Council. Its key domains of implementation, mechanisms of impact, and context were all incorporated as central elements of the analysis [17,18] (online supplementary figure 2). The theory of normalization process provided the conceptual framework for the process evaluation. It was also used to identify the factors that facilitated or hindered the integration of the JOIN application into routine clinical practice, as well as the work undertaken by individuals to achieve this integration [15]. The four core constructs of normalization process theory are:
-
Coherence: the meaning and sense-making attributed to the intervention by participants.
-
Cognitive participation: the commitment and engagement of participants in the intervention.
-
Collective action: the work that individuals must undertake to ensure the intervention functions effectively.
-
Reflexive monitoring: the appraisal and evaluation of the intervention by participants.
These four constructs were used to develop the interview guide (online supplementary table 2) to characterize the implementation process and explore the dynamic interactions among individuals, groups, and organizational contexts during the integration of the JOIN application into routine practice.
Participant selection and recruitment process
For the process evaluation, we used a purposive sampling strategy to capture relevant experiences in diverse contexts and gain a comprehensive understanding of the phenomenon under study. For the sampling units, we considered professionals or coordinators who had actively participated in implementing and using the JOIN app for managing acute stroke, both in the aforementioned hospitals and in primary emergency care services. In the snowball recruitment strategy, we included an email invitation to participate that provided all the study information. The interviews were conducted between October and December 2024.
Context and data collection
Following the informed consent process (completed electronically via the REDCap database [19]), semi-structured interviews were conducted with the participants. These were led by FG and conducted individually via video conferencing on Teams, each lasting approximately 45 minutes. The interviews followed a predefined yet flexible script consisting of open-ended questions. We began with an introduction of the interviewer, her role, and the purpose of the interview. Initially, we encountered some difficulties with internet connections in noisy or work environments, which caused some interruptions. To address this and ensure a better experience, we asked subsequent participants to choose more comfortable and quieter spaces. Audio recordings were made of all interviews, and we took field notes during the sessions. We then transcribed the interviews in full into Word and assigned a unique code to each participant to ensure the security and confidentiality of the interviewees. The interviews continued until data saturation was reached. This occurred when no new information emerged, indicating that the sample was sufficient to capture the participants’ experiences regarding this topic.
Data analysis
Through an iterative and reflective process, two authors (FG and ADR), with training in qualitative analysis, participated in data coding. Using deductive thematic analysis and following the approach proposed by Braun and Clarke [20], we identified, analyzed, and reported the emerging themes within each construct. We organized the information based on the four components of process normalization theory, which served as the initial framework for coding. The round of establishing these codes allowed us to organize the data into broader categories. For the data coding process, we used the ATLAS.ti25 software. We conducted the data analysis by consensus, with an emphasis on identifying barriers and facilitators to using the JOIN app. We also highlighted the key implementation outcomes: adoption (initial intention to try an innovation), acceptability (satisfaction), suitability (relevance), fidelity (adherence), and feasibility of use [21]. We employed various measures to ensure the quality and rigor of the data collection process. The researchers’ reflexivity was a key factor in this study, achieved through ongoing self-reflection throughout the data collection and analysis processes, as well as in addressing personal assumptions. We held regular discussion meetings to conduct a critical evaluation and minimize potential biases during the analysis.
Results
The characteristics of the participants (n = 8) and their respective workplaces are presented in Table 1. Notably, the majority of participants were medical professionals (neurologists) from secondary- and tertiary-care hospitals and urban areas of Santiago.
Participants identified three main categories related to factors that facilitate the use of the JOIN app:
-
User-friendly and intuitive app.
-
Training and ongoing feedback.
-
Team leader.
JOIN was highlighted as a well-known, intuitive, and standardized tool that streamlines processes and reduces response times. Many interviewees acknowledged having used it previously in hospitals in other countries, noting its daily use and significant support in the routine management of acute stroke. Meanwhile, the training sessions conducted throughout the period leading up to activation and during its implementation were perceived as essential for using JOIN. The prompt feedback received in response to questions and the ongoing training were also mentioned as key factors in continuing its use. In addition, having a team leader who provides direction and an action plan to the rest of the members was recognized as an important facilitator (see quotes #1, #2, and #3 in Table 2).
Regarding the difficulties and barriers to the effective implementation of JOIN in the hyperacute care of stroke patients, the following categories were identified:
-
Overburdening of the emergency care system.
-
General resistance to change.
-
Difficulties in using the technology.
Regarding the first category, users reported that hospital emergency departments had teams with heavy workloads and a constant turnover of professionals and technicians, making it difficult to incorporate new care management tools and leading to low user motivation to use them. In addition, we identified resistance to changing the processes to which the teams were already accustomed in their daily work. They mentioned having little time to attend training sessions and not having enough time to enter data into the application during their shifts. Difficulties with new technology and technical enablers were also perceived as barriers to implementation and use, with reports of connectivity issues in the area and lost activation access codes (see quotes #4, #5, and #6 in Table 2).
The interviewees unanimously recognized the importance and benefits of having new tools to improve care processes during the initial phase of a stroke. They emphasized the need to improve communication among the various stakeholders, including ambulance services, emergency departments, and primary care emergency services. The JOIN app was perceived as an easy-to-use, user-friendly tool, and most professionals were familiar with it and had previously used it at other institutions. However, despite the initial acceptance and adoption by most of the interviewees, the implementation process itself presented difficulties, and limited use was reported. Partial use of its functions was observed, along with limited suitability in the emergency context within this network. Greater participation was observed among the neurology teams across the three hospitals, whereas other involved physicians and primary emergency care staff showed lower motivation. The definitions of the components of the implementation outcome assessment, along with the most representative citations, are presented in Table 3. In addition, we present a summary of the findings according to the logical framework for the implementation research in Figure 1.
Summary of findings based on guidelines from the Medical Research Council.
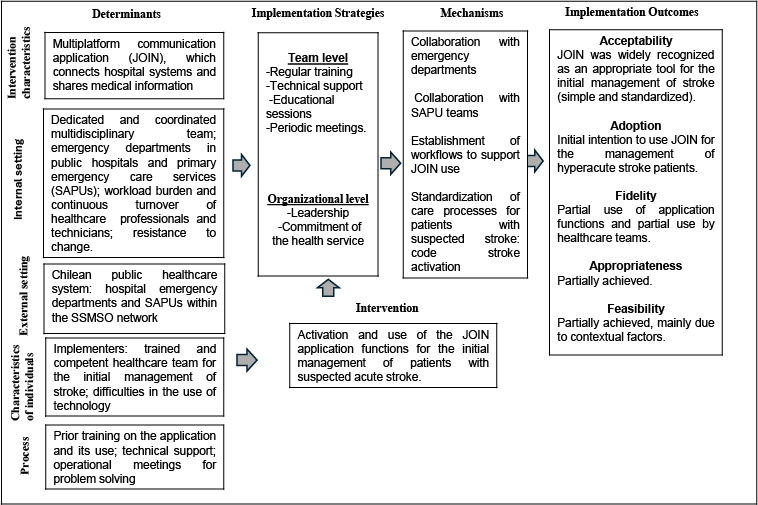
Source: Prepared by the authors.
Discussion
In this study, we explored the process of implementing and using the JOIN app for the management of acute stroke within a network of hospitals and primary emergency care services of the South-East Metropolitan Health Service in Santiago, Chile. The aim was to identify the main facilitators, barriers, and perceptions of the app’s impact on its use. The findings revealed that, although the app was perceived as a user-friendly tool with the potential to improve coordination and communication in patient management, its effective implementation was limited by various organizational, structural, and contextual factors. In this regard, these results highlight a gap between the initial acceptability of a digital tool and its effective implementation in complex healthcare settings. This is inconsistent with previous studies that have successfully used JOIN in their acute stroke care processes, achieving positive workflow outcomes and reducing care times [22,23].
Recognizing the application as a useful, standardized tool demonstrated a high degree of coherence between JOIN’s purpose and the clinical team’s needs. Previous familiarity with JOIN in other hospital settings strengthened its acceptability, while training sessions and continuous feedback served as mechanisms for reflexive monitoring, enabling the resolution of challenges and the progressive refinement of its use. The presence of committed clinical leaders emerged as a decisive factor in guiding and mobilizing team engagement. This finding is consistent with previous studies highlighting the role of leadership and internal communication as key determinants in creating an environment conducive to innovation [24].
Conversely, the heavy workload in the emergency departments of participating hospitals and the high turnover of healthcare staff were identified as major barriers to successful implementation. This phenomenon relates to the collective action component of Normalization Process Theory, revealing significant practical challenges during implementation. In particular, participants reported limited time to attend training sessions, activate the application, and complete data entry. These factors reflect structural constraints within the healthcare system that influence implementation beyond the intervention’s intrinsic characteristics. Resistance to change among some teams, particularly regarding the incorporation of technology into clinical workflows, was also observed, reflecting low levels of cognitive participation. Such resistance underscores the importance of behavioral and organizational change processes as essential elements of successful implementation, extending beyond the mere availability or acceptability of the innovation itself [25].
Regarding the key implementation outcomes, the process evaluation demonstrated a high level of initial acceptability of JOIN. However, we identified only partial use of the platform’s functionalities, participation limited to certain healthcare professionals or care coordinators, and limited feasibility for its use within this specific context. These findings clearly illustrate that initial acceptability does not necessarily guarantee successful implementation. They are consistent with the existing literature, which indicates that technological innovations in healthcare remain a significant challenge and are more likely to become established when supported by a robust implementation strategy that incorporates leadership, financial, organizational, and human resources, as well as an infrastructure capable of facilitating their integration [26].
The findings of this process evaluation provide evidence of the practical challenges involved in implementing digital applications in healthcare settings with high operational demands. Existing evidence suggests that the main facilitators of high-quality acute care delivery are closely linked to training, innovation, and effective healthcare networks [1]. However, this experience demonstrates that the successful integration of tools such as JOIN requires a multi-component approach that encompasses continuous training, ongoing technical support, visible clinical leadership, and alignment with institutional priorities. Finally, the authors emphasize the importance of strengthening communication and feedback channels across levels of care to maximize the potential of these technologies to improve response times and enhance interhospital coordination.
Strengths and limitations
This multiple case study design, employing a qualitative methodology, enabled an in-depth exploration of the perceptions of the key stakeholders involved in the activation and use of the JOIN application for the management of acute stroke. The study provided a contextualized understanding of the facilitators and barriers affecting care delivery during the initial phase of stroke management. The use of Normalization Process Theory as an established analytical framework allowed for a systematic examination of how the intervention was, or was not, integrated into routine clinical practice, while accounting for the dynamic interactions between individuals and organizational contexts. Furthermore, the qualitative approach facilitated the identification of the unique dynamics and tensions inherent to high-demand healthcare settings, which are generally difficult to capture with the same level of depth in quantitative studies.
However, this study has several limitations that should be considered. First, the study sample consisted primarily of hospital-based physicians, particularly neurologists, with relatively limited participation from primary care and prehospital providers. This distribution may have influenced the interpretation of the findings and limited a more comprehensive understanding of the broader healthcare network’s functioning. Consequently, the results should be interpreted with caution regarding their transferability to other settings or stakeholders within the healthcare system. Secondly, the findings focus on participants' perceptions of JOIN use and therefore do not permit an assessment of its impact on clinical outcomes or performance indicators.
This process evaluation was conducted during a relatively late stage of the implementation of JOIN by the healthcare teams. Future studies would benefit from conducting similar evaluations at earlier stages of implementation, as this could facilitate the identification of potential areas for improvement and enable timely modifications to the implementation process when necessary.
Conclusions
The process evaluation provided valuable insights into the challenges of implementing new processes in emergency care settings and other high-demand healthcare contexts. Specifically, these challenges relate to the integration of new innovations.
Despite technological advances and individuals’ recognition of their benefits, there is currently a gap in the adoption of these innovations in more complex settings, which require a more comprehensive understanding to achieve successful implementation.
In summary, the results reinforce the need to consider the healthcare context and team dynamics when implementing digital innovations.
Metadata
