Estudios originales
← vista completaPublicado el 31 de marzo de 2014 | http://doi.org/10.5867/medwave.2014.02.5927
Factores de riesgo asociados a hábitos bucales deformantes en niños de 5 a 11 años: estudio de casos y controles
Risk factors associated with deforming oral habits in children aged 5 to 11: a case-control study
Abstract
INTRODUCTION Dental and maxillofacial anomalies have multiple and complex causes. Most frequent among these are poor oral habits. A large number of children present with oral malocclusions, most of which are caused by deforming oral habits. It is important to learn about risk factors for this condition in order to institute preventive measures, early detection and treatment, and identification of low- and high-risk groups.
OBJECTIVES To identify risk factors associated with deforming oral habits, which, if maintained over time, are responsible for occlusion defects, speech disorders, and can affect physical and emotional child development.
METHODS A case-control study of children presenting with deforming oral habits in the municipality of Manzanillo in Granma province was conducted between January and August 2013. 540 children aged 5 to 11 were included of which 180 had deforming oral habits and were asked to fill out a survey to identify specific type of habits leading to malocclusion. The case group was composed of children with deforming habits, and the remaining 360 children without poor oral habits were the control group. Each case was randomly matched to two control cases. The children’s mothers were also surveyed to gather supplemental information.
RESULTS Children with deforming oral habits were mostly female. At age 10, onychophagia was the predominant oral deforming habit. Risk factors detected for these habits were sociobiological maternal and child variables such as low and high birth weight, maternal breastfeeding inexperience, and discord in the family.
CONCLUSIONS The study identified likely risk factors associated with deforming oral habits. These are discord in the family, birth weight, and lack of breastfeeding experience.
Introduction and objectives
The causes of dentomaxillofacial anomalies are multiple and complex. Improper, deleterious, or deforming oral habits are among the most common [1].
Deforming oral habits are defined as a form of behavior that is picked-up due to its frequent repetition. They have no functional use nor are they necessary. Furthermore, they exert unnatural forces upon the teeth, which can lead to dentomaxillofacial alterations. These appear in 56% to 75% of children, and they can lead to alterations in neuromuscular balance, bone-tooth discrepancy, posterior and anterior crossbite, anterior open bite, as well as causing mandibular deviation [2],[3].
Each of the indicators for dentomaxillofacial anomalies affecting esthetics and child dentofacial function dropped by 50% with exclusive maternal breastfeeding [4],[5].
Identifying risk factors is a necessary step toward primary prevention. Likewise, recognizing risk markers can be extremely useful in identifying low- and high-risk groups, as well as for secondary prevention when the means for early detection and fast treatment are available [1],[6],[7],[8],[9].
Risk factors do not act isolated from one another, but rather as a whole and in an interlinked fashion. This often greatly augments their damaging effect on health. Calculations have been made on the combined action of the risk factors, revealing that the damage is always greater in concert vis-à-vis the sum of the relative risks. Consequently, assessing a risk factor will be scientifically more acceptable if not only the direct and isolated effects be taken into consideration, but also their combined effects with other variables of interest [1],[10],[11].
There are beneficial or functional habits such as chewing, swallowing and normal breathing, and there are also incorrect or deforming habits. Among the latter, mouth breathing, lip or nail biting, tongue thrusting, object chewing and finger-sucking, along with pacifier and baby-bottle use beyond the age of 3 years of age, since these habits are considered normal before then. Deforming habits can lead to occlusion alterations if they are maintained over long periods of time. Another negative effect from these habits are disorders in speech and in the child’s physical and emotional development [1],[12],[14].
The motivation behind carrying out this study was the amount of children that go to the doctor with malocclusions, which mostly arise due to deforming oral habits. We need to be aware of the risk factors in their incidence, in order to be able to reduce their occurrence as much as possible and avoid negative consequences.
Method
Medical bioethics
During the organization phase of the study, a meeting was convened with the Municipal Directorate and the Scientific Council to lay out the objectives of this research study. After been informed of the details of the study, voluntary consent was obtained from patients and their mothers in order to participate. They were explained that the study represents no risk or harm to their health, and that they must be mentally fit to participate (Annex 1).
General characteristics
A control case study was carried out on children affected by deforming oral habits, in order to identify the associated risk factors. The study involved participants from the township of Manzanillo during January to August 2013. A total of 540 children were selected out of all children aged five to eleven in the area. The 180 children who on examination presented deforming oral habits were surveyed in order to determine the kind of habits performed by the children. The children with deforming habits made up the case group, and the remaining 360 children, who were free of deforming oral habits, made up the control group. Each of the participants’ mothers was surveyed in order to obtain the remaining variables which were necessary for the study. One case was taken for every 2 in the control group, based on random sampling.
Diagnostic criteria for a child with a deforming oral habit: prior diagnosis by a stomatologist (authors).
Inclusion criteria: 5-11 year-old children falling under the Manzanillo Municipality health area. Consent to participate was required from the child, parents or guardian.
Exclusion criteria: children or parents with any mental disorder that would impede gathering necessary data.
Evaluation criteria: two groups were formed in order to carry out this study, the study group and the control group:- Study group: made up of 180 children who exhibited a deforming oral habit and who fell under the aforementioned health area. They were selected at random with prior consent to participate in the study. The method that was used was the administration of a survey for the mother, an intra-oral examination, and a medical interview with the boy or girl.
- Control group: made up of 360 children belonging to the aforementioned health area and who did not present any deforming habit. They were selected at random with prior consent to participate in the study. The method used was the administration of a survey for the mother, an intra-oral examination, and a medical interview with the boy or girl.
Variables and their operationalization
The following aspects were documented with the survey:
Age of the children, expressed in years: the lower limit was 5 years of age, and 11 years the upper limit.
Age: 5 years, 6 years, 7 years, 8 years, 9 years, 10 years, 11 years of age.
Sex: They were separated into two biological categories (male or female).
Deforming habits: the following are considered under this category:
- Finger sucking: sucking on one or more fingers.
- Nail biting: biting nails or cutting them with the teeth.
- Protractile tongue: thrusting of the tongue between the two upper incisors when swallowing.
- Pacifier and baby-bottle use: sucking on a teat or being bottle-fed. These habits are considered normal under the age of 3.
Mouth breathing was not included, due to the necessary secondary level diagnosis.
Among the mothers’ and children’s sociobioligical variables associated with the presence of deforming oral habits, the following were taken into account:
Birth weight, classified in categories as proposed by Martinez Padron M. [15]:
• Low birth weight: any newborn who at birth weighs less than 2,500 grams.
• Normal birth weight: any newborn who at birth weighs over 2,500 grams.
• High birth weight: any newborn who at birth weighs over 3,800 grams.
Weight and excess weight were taken into account as risk factors.
Maternal breastfeeding period, classified in categories as:
- Positive: if the children received breast milk exclusively throughout the first four months of life.
- Negative: if the children were not exclusively breastfed, or if feeding was combined or multiple. This category was considered as a risk factor.
Family functionality, for which the aspects in this survey were the following:
- Family harmony: the child was brought-up in a harmonious family environment.
- Family arguments: the child was brought up in a hostile environment of parents arguing with each other, or with other relatives or even neighbors.
- Two-parent child upbringing: the child was raised by both parents, in a harmonious family environment.
- Child brought up by a single mother: the child was raised without the presence of a father.
- Child brought up by grandparents: the child was raised by both or one grandparent, regardless of whether or not the child lives with the mother.
Harmonious functionality was deemed to be present in a home where what prevails is compromise and agreement, and where the child was raised by both parents. On the other hand, children fell into non-harmonious functionalities if they were raised by a single mother or by grandparents, and if there were arguments within the household. The non-harmonious functionality was defined as a risk factor.
Techniques and procedures
Data gathering. A broad literature review with a high level of scientific validity in the areas in question was conducted at different centers (Information center, Libraries, Infomed and Google searches, etc.) in order to carry out this study.
In addition, the age, sex, and deforming oral habit variables were collected for each of the examined children. Finally, a survey was designed (Annex 2) for the mothers of each child, for gathering variables such as: birth weight, maternal breastfeeding period, and family functionality.
Processing and analysis. The data obtained from the observations was stored in records especially created for this purpose. This aided in the processing phase, which was performed using a Pentium IV personal microcomputer. Using this device, the Microsoft Office 2007 programs were used to draft the final report.
To identify the “risk” condition among the study variables associated with deforming oral habits, first the Chi-Square test was performed. Subsequently, after obtaining the ratios among the studied variables, the Odds Ratio was performed to determine the “risk” condition with regard to the different characteristics under study. The significance ratio used was ∝=0.05.
The results were presented using statistic tables, using absolute numbers and percentages. Analysis and results discussion was performed by making comparisons with other authors and drawing conclusions.
Results
It can be seen that the female sex was predominant in terms of finger sucking, with 44.3%. Males were predominantly nail biters, at 48.2%. Among the total of selected children, nail biting was the most prevalent overall at 42.8%.
 Full size
Full size When analyzing birth weight, normal birth weight was predominant in both groups at 61.1% for the case group and 96.1% for the control group.
 Full size
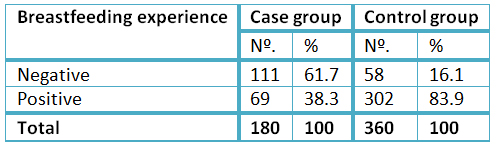
Full size Within the case group, a negative breastfeeding experience was the most common, at 61.7%. In the control group, a positive experience was predominant, at 83.9%.
 Full size
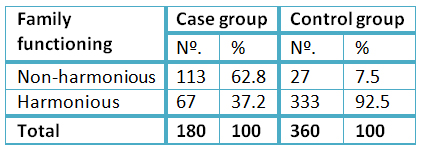
Full size Non-harmonious family functionality predominated within the case study group at 62.8%. Within the control group, the harmonious functionality was most common, tallying 92.5%.
 Full size
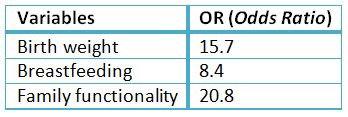
Full size In terms of the variables that behaved in a non homogeneous manner, an Odds Ratio test was performed and the degree of association between the risk factor and the disorder was measured. This indicated that this disorder is more common in the case group vis-a-vis the control group. A clear example is that within the family functionality categories, case study participants were up to 20.8 times more likely to present deforming oral habits in comparison to the control group.
 Full size
Full size Discussion and conclusions
The results are consistent with the study by Rodriguez Gonzales [5], where finger sucking was predominant, albeit in that study, age and not sex was taken into account. These results do not concur with those of the study by Claudino and Traebert [6], where it is shown that the most common habit was the use of pacifiers and baby-bottles, whereas in this study most frequent habits are among girls.
This study does not concur with the findings posted by Jimenez Ariosa [3], where the use of pacifiers and mouth breathing were predominant. The authors of that study are of the opinion that this is due to the fact that nowadays children are exposed to more violent physical games, as well as having access to violent computer games and horror movies, and that this subconsciously leads to nail biting or gnawing [9].
Among the case group, 38.9% of the children were within the low-weight or high-weight group, considered as risk factors for acquiring deforming oral habits. This percentage significantly differs from the 96.1% obtained in the control group, where the aforementioned deleterious oral habits are not manifest, and where the percentage of variables presented as risk factors was insignificant.
The results are consistent with the author’s previous study [1], albeit the sample was far smaller.
For the infant, natural feeding is the most important form of exchange with the outer world. The infant is not only nourished, but also derives a feeling of euphoria and wellbeing by satisfying the need for love and security, as well as establishing physical contact (through tactile, mouth contact, and sounds) which is gratifying for both mother and child. During breastfeeding, the child presses the tongue against the lactiferous ducts to obtain milk, but no effort is required for shaping the teat within the child’s mouth when they are bottle-fed. If the child suckles and regulates flow with the tongue, the normal stress reaction can give way to other habits such as atypical swallowing [1].
In Cuba, legislation in place for workers, providing up to one year of compensated leave after childbirth, coupled with the mother’s educational level and the constant rise in health awareness, serve to create favorable conditions for prolonging the breastfeeding period [1].
A negative breastfeeding experience prevailed in this study at 61.7%, due to the delay in milk reaching the breasts, since the mothers reported not having enough milk, along with their belief that they should be kept upright when not feeding. In this aspect, the authors consider the negative breastfeeding experience as a potential factor in the onset of deforming oral habits. This is consistent with the findings by Rodriguez and Ariosa [5],[3], with the existing link between premature weaning and the onset of this type of habits, which are apparently closely related to the duration of the breastfeeding period. In this regard, it can be affirmed that the habit of finger sucking that appears in the first weeks of breastfeeding is due to hunger or lack of satisfaction with suckling.
The children in this study who were breastfed longer presented less incorrect oral habits [13], on account of the positive breastfeeding experience that was most common among the control group, at 83.9%. Premature weaning contributes toward a higher rate of deforming oral habits in children [15].
Non-harmonious family functionality is another factor that has a significant impact on the development of deleterious habits in children within this age group. The explanation apparently lies in frequent arguments between parents, especially when the parents are separated and one parent lives far away from the child. This leads to the child being raised by only the mother or being overprotected by the grandparents. In the control group, harmonious family functionality was predominant, at 92.5%. Within this group, the children were seen to be more fulfilled in a pleasant environment, under less emotional pressure, leaving their imagination to run-free.
For the breastfeeding variables, birth weight and family functionality, the Chi-Square test was applied, beginning with the hypothesis of homogeneity between the two study groups (case and control). Subsequently, if they behaved in a non homogeneous manner, the Odds Ratio was calculated, with a view to measuring the degree of association between the risk factor and the disorder in question, namely deforming oral habits. This indicated that the event occurs more frequently among patients in the case group rather than in the control group.
Based on the study carried out on this population group, it can be concluded that among the children studied with deforming oral habits, females and children aged 10 were the most frequently affected. Nail biting was the predominant form of deforming oral habit. Harmonious family functionality, birth weight and the breastfeeding experience were identified as risk factors associated with deforming oral habits. Socio-biological variables for the mother and children such as low and high birth weight, not having an exclusive breastfeeding experience, and the lack of harmonious family functionality, were considered as conditions of risk in developing deforming oral habits.
Notes
Contributors
Dr. Roberto Gil Macias helped with style revision, critical appraisal, formatting, and literature search.
Potential conflicts of interest
All authors have completed the ICMJE uniform disclosure form translated into Spanish by Medwave and declare no relationships or activities that could appear to have influenced the submitted work.
Ethics
This study was approved by the Ethics Committee of the Faculty of Medical Sciences, Granma, Cuba. The approval certificate may be requested from the corresponding author or journal.
