Research papers
← vista completaPublished on August 8, 2016 | http://doi.org/10.5867/medwave.2016.07.6510
Spanish version of the Kidney Disease Knowledge Survey (KiKS) in Peru: cross-cultural adaptation and validation
Versión en español, del “Kidney Disease Knowledge Survey” (KiKS) en Perú: adaptación cultural y validación
Abstract
INTRODUCTION Chronic kidney disease (CKD) affects 50 million people globally. Several studies show the importance of implementing interventions that enhance patients’ knowledge about their disease. In 2011 the Kidney Disease Knowledge Survey (KiKS) was developed: a questionnaire that assesses the specific knowledge about chronic kidney disease in pre-dialysis patients.
OBJECTIVE To translate to Spanish, culturally adapt and validate the Kidney Disease Knowledge Survey questionnaire in a population of patients with pre-dialysis chronic kidney disease.
METHODS We carried out a Spanish translation and cross-cultural adaptation of the Kidney Disease Knowledge Survey questionnaire. Subsequently, we determined its validity and reliability. We determined the validity through construct validity; and reliability by evaluating its internal consistency and its intra-observer reliability (test-retest).
RESULTS We found a good internal consistency (Kuder-Richardson = 0.85). The intra-observer reliability was measured by the intra-class correlation coefficient that yielded a value of 0.78 (95% CI: 0.5-1.0). This value indicated a good reproducibility; also, the mean difference of -1.1 test-retest SD 6.0 (p = 0.369) confirms this finding.
CONCLUSION The translated Spanish version of the Kidney Disease Knowledge Survey is acceptable and equivalent to the original version; it also has a good reliability, validity and reproducibility. Therefore, it can be used in a population of patients with pre-dialysis chronic kidney disease.
Introduction
Chronic kidney disease (CKD) affects 50 million people globally [1]. The management of chronic kidney disease should be multidisciplinary in order to delay disease progression to end-stage renal disease, reduce associated complications and/or allow patients to start renal replacement with a better prognosis [1],[2].
Several studies have emphasized the importance of developing interventions to improve patients´ knowledge regarding their disease [3],[4]. A higher level of knowledge would allow patients to better comply and manage their own care by eliciting behaviors such as avoiding nephrotoxic agents, maintaining a healthy diet, achieving blood pressure targets and greater adherence to treatment [3],[4].
Several questionnaires have been developed with the aim to assess hemodialysis patients´ knowledge about their disease; however, only a few studies have proposed to measure knowledge of patients in stages 1-5 who have never been on dialysis [5],[6]. In 2011, the Kidney Disease Knowledge Survey (KiKS) was developed in the United States as a questionnaire to assess chronic kidney disease specific knowledge in patients who do not yet require renal replacement therapy [7].
The objective of this study is to translate to Spanish, and culturally adapt and validate the questionnaire Kidney Disease Knowledge Survey in patients with pre-dialysis chronic kidney disease.
Methods
This validation study was developed in three phases: translation/back translation, cultural adaptation and validation of the questionnaire from July 2014 to December 2014. Ethical approval was granted by the Ethics Committee of the Universidad Peruana de Ciencias Aplicadas (UPC) and Hospital Nacional Guillermo Almenara Irigoyen (HNGAI).
Survey description
The Kidney Disease Knowledge Survey (KiKS) was generated in English to assess chronic kidney disease specific knowledge in patients with chronic kidney disease (pre-dialysis stages 1-5) in order to understand patients’ level of knowledge regarding their condition. The questions are directed at knowledge in the areas of renal function, treatment alternatives for renal failure, signs and symptoms of disease progression, potentially beneficial or toxic medications, blood pressure targets and other important topics to preserve kidney function. The survey includes 28 questions, five multiple choice type questions and 23 Yes-No questions; none of the questions included an "I don´t know" option. To assess the survey score, one point was given to each correct answer and zero to each wrong one. The questionnaire doesn’t have domains, and the total score was calculated as the sum of the correct responses to each question divided by the total number of questions, which results in values from 0 to 1 where 1 means the highest level of knowledge. The Kuder Richardson coefficient (internal consistency) was 0.72 with an average score of 0.66 in the original study [7].
Translation and back translation
Step 1: Translation to Spanish. Two Peruvian translators translated the questionnaire to Spanish. Each translation was done independently and the difficulties during the process were reported to the investigators (understanding of medical terminology, adaptation of terms, etcetera) [8].
Step 2: Expert Committee. This committee consisting of an expert in methodology, two nephrologists and the investigators reviewed both translations and elaborated a single version in Spanish. This was forwarded to the translators to approve the new version [8].
Step 3: Translation to English. Two translators whose mother tongue is English, unfamiliar with medical terminology, translated the English version of the questionnaire made in step 2 to Spanish. Each translation was done independently and the difficulties were reported to the investigators [8].
Step 4: Expert Committee. The committee reviewed both translations and elaborated a single English version. This was forwarded to the translators to obtain their approval. Subsequently, the questionnaire obtained in English was forwarded to the authors of the questionnaire Kidney Disease Knowledge Survey to evaluate the equivalence of the original instrument to the final translated version.
Cross-cultural adaptation
This process was conducted in two phases: Pilot testing: The pilot study was conducted with the Spanish version of the questionnaire. The questionnaire was applied to 15 patients hospitalized in the Nephrology Department of Hospital Nacional Guillermo Almenara Irigoyen in order to determine whether there was any difficulty in answering the questionnaire [9]. Expert committee: The expert committee evaluated the results of the pilot study in order to modify the questionnaire items regarding the difficulties encountered during its application such as lack of understanding of any questions or possible responses.
Validation
The validity and reliability of the instrument were evaluated [10],[11],[12]. Reliability was assessed using two indicators, internal consistency and stability. Internal consistency was tested using the Kuder-Richardson coefficient, a value >0.70 was considered acceptable, this was assessed with the total population for construct validity. The stability of the questionnaire was evaluated by using the test-retest method in 30 patients of the Hemodialysis Unit of Hospital Nacional Guillermo Almenara Irigoyen on two occasions one week apart under similar conditions. The overall stability of the instrument was assessed by the intraclass correlation coefficient, a value >0.40 was considered as moderate agreement. In addition, the stability of each item was evaluated by Kappa coefficient and McNemar test. A Kappa value should be at least >0.4 to represent a moderate agreement, and the McNemar test >0.05 to determine that there was no variation between responses [13].
The validity of the questionnaire was measured by construct validity. This was assessed using the method of difference between known groups [10]. A comparison of the level of knowledge was performed between physicians and residents of the specialties of nephrology and internal medicine from Hospital Nacional Guillermo Almenara Irigoyen and Hospital Nacional Edgardo Rebagliati Martins, and a group of patients with chronic kidney disease in pre-dialytic stages, considering the first group as the expert one. To calculate the sample size, a difference greater than 20% of the score between the expert and non-expert group was procured. For this purpose, the formula of difference between two means (independent groups) was used, considering the mean and standard deviation (0.66 and 0.15 respectively) of the score of patients from the original study [7], a statistical power of 90% and a confidence interval of 95%. A minimum of 28 participants was determined for each group, eventually enrolling 30 people per group. We excluded those who didn’t answer all the questions in the survey.
Data analysis
Data was double keyed and entered into Microsoft Excel 2010®. After quality control, data was exported to the software STATA 14.0® for its statistical analysis p <0.05 was considered as significant. Categorical variables with absolute and relative frequency were described as well as numeric variables with mean and standard deviation prior verification of normal distribution by the Shapiro Wilk test. The mean difference between the expert and non-expert groups was calculated by the Student t- test for independent samples. The intraclass correlation coefficient was calculated for the entire instrument as well as Kappa values and McNemar test for stability. The difference between the overall pretest and post-test scores was also determined using the paired Student t- test. Kuder Richardson was calculated for internal consistency.
Results
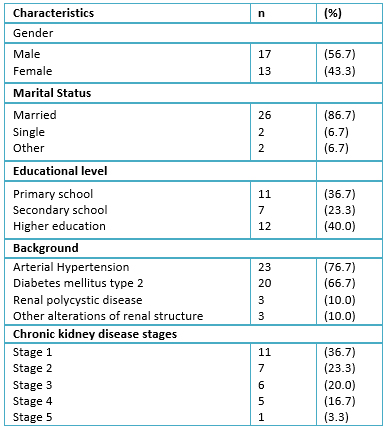
The characteristics of patients with chronic kidney disease in pre-dialytic stages are presented in Table 1.
 Full size
Full size Translation and back translation
During the translation of the instrument, some difficulties were encountered. In question number 6 "What does “GFR” stand for?", the expert committee elaborated four new statements that matched the acronym GFR and that were related to this question, because an acronym only applies to the original language. During the back translation of the survey from Spanish to English, no difficulties were encountered. The English version was obtained, its equivalence to the original questionnaire was determined by decision of the expert committee and the approval of the authors of the Kidney Disease Knowledge Survey.
Cross-cultural adaptation
In question number 1: "On average, your blood pressure should be”, the answer "lower than 130/80" was replaced by "lower than 140/90", because according to the latest report of the Eighth Joint National Committee (JNC8) the ideal blood pressure in patients with chronic kidney disease should be lower than 140/90 [14]. Similarly, in question number 4: "Select the one medication from the list below that a person with chronic kidney disease should avoid", the expert committee proposed that the lisinopril answer should be replaced by enalapril because patients were more familiar with this drug name. They also suggested to replace the Motrin/Ibuprofen option by just Ibuprofen because drugs are not usually prescribed by their brand names in Peru. Moreover, after performing the pilot study, most patients didn´t understand the term “Estadios” in Question 7 "¿Hay estadios en la enfermedad renal crónica?"; however, they understood the term “Etapas”, for this reason the expert committee decided to add this term to the question. The modifications mentioned were approved by the authors of the original questionnaire.
Validation
Construct validity of Kidney Disease Knowledge Survey was obtained by comparing the mean of knowledge of the group of doctors whose value was 0.82 ± 0.10 with the mean of knowledge of patients with chronic kidney disease in pre- dialytic stages whose value was 0.49 ± 0.17 (p <0.001).
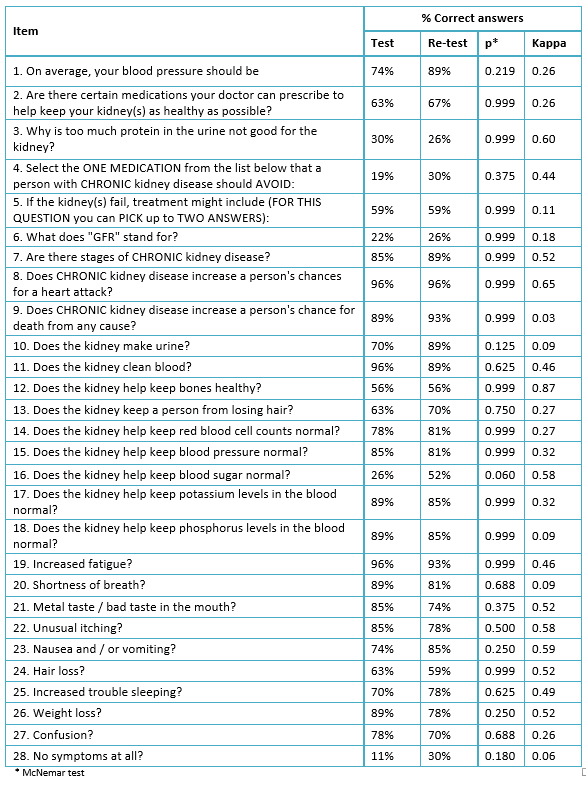
Regarding the reliability of the questionnaire, a good internal consistency was found with a Kuder-Richardson coefficient of 0.85. Regarding the overall stability of Kidney Disease Knowledge Survey, good reproducibility was found with an intraclass correlation coefficient of 0.78 (95% CI 0.5-1.0), which is supported by having no score differences before and after the paired Student t test (p = 0.369) However, there was no evidence of a good stability by items. One question showed a p<0.100 with the McNemar test, and ranges of kappa varied between 0.03 and 0.87, half of the items (14/28) showed kappa values of <0.40 (Table 2). The annex shows the final version of the instrument in Spanish.
 Full size
Full size Discussion
The questionnaire obtained in this study has shown to be valid in measuring knowledge in patients with chronic kidney disease in pre-dialytic stages after accomplishing the process of translation, cultural adaptation and validation in a Peruvian population. Regarding the process of translation/back translation, no major problems were encountered except for the question of GFR that was resolved as mentioned above. During the cultural adaptation, several changes that allowed a better semantic and conceptual understanding of the instrument were performed. Regarding the validity, when determining the reliability of the survey a good internal consistency was found by a Kuder-Richardson coefficient of 0.85, which was higher than the one found in the development of Kidney Disease Knowledge original Survey (0.72) as well as other validation studies [7]. In regards to the stability of the questionnaire, it has proven to be reliable and reproducible as a whole, although individually some items have shown less reproducibility. This may be because the instrument doesn’t include the option "I don’t know", which was proposed to the original authors who requested not to add this option if the survey was intended to be consistent from the original. However, adding this option might have an impact on the stability of the items as well as the overall score, making it lower; future studies could evaluate this change. Finally, the questionnaire is able to discriminate between the highest and lowest level of knowledge among populations as it has been proven by the score difference between physicians and patients.
The mean of knowledge of the target population was 0.49, which was lower than the found in the original study of Kidney Disease Knowledge Survey (0.66) [7]. Also, some important topic areas are not well understood by patients. For example, reducing the presence of protein in urine is a mainstay in chronic kidney disease management; [15] however, 70% did not know that proteinuria is not only a sign of kidney damage, but it can also affect the kidneys. Additionally, patients should avoid taking non-steroidal anti-inflammatory drugs because of potential nephrotoxicity; [16] however, 77% didn’t identify ibuprofen as a drug they should avoid. As well, chronic kidney disease can progress to advanced stages even in the absence of symptoms; [17] however, only 33% believed that chronic kidney disease may progress even without symptoms. On the other hand, a higher knowledge was found concerning areas of basic kidney information and mortality associated with chronic kidney disease. 70% identified that the kidneys produce urine and 93.3% that kidneys have a role in waste clearance. 93% and 83% considered chronic kidney disease as a risk factor for increased mortality from heart attacks, and from any cause respectively.
This study has some limitations. First of all, given the cultural and socioeconomic differences among Spanish-speaking countries, it is necessary to evaluate whether the terms of the instrument are understandable by patients in other countries. In case some adjustments need to be made, at least a cultural adaptation and reliability process should be assessing before it can be used. On the other hand, hemodialysis patients were enrolled for evaluating test-retest, because of the ease of finding them; however, the instrument was made for pre-dialysis patients. Nevertheless, this difference didn´t affect the results obtained which is the reproducibility of the instrument at different times. Finally, no specific sample size was calculated for measuring the stability of the questionnaire by items (Kappa and McNemar test), so it may be possible that the statistical power for these tests is lower than 80%.
Conclusions
In conclusion, translation, cultural adaptation and validation of the questionnaire Kidney Disease Knowledge Survey was performed in a population of patients with chronic kidney disease in pre-dialytic stages. The Spanish version obtained is equivalent to the original version of the instrument, and thus can be used to measure knowledge about this disease. It is recommended that more studies validate this questionnaire in other Spanish-speaking countries, as well as evaluate possible associated factors with chronic kidney disease level of knowledge and the potential clinical outcome after educational interventions.
Notes
Annex: Cuestionario validado sobre conocimientos de enfermedad renal crónica.
From the editor
The authors originally submitted this article in Spanish and was translated into English by the authors. The Journal has not copyedited the English version.
Ethical aspects
The Journal is aware that the scientific ethics committee of the School of Medicine, Universidad Peruana de Ciencias Aplicadas, was informed about this study and its possible publication in a journal of biomedical diffusion.
Conflicts of interest
The authors completed the ICMJE conflict of interest declaration form, translated to Spanish by Medwave, and declare not having received funding for the preparation of this report, not having any financial relationships with organizations that could have interests in the published article in the last three years, and not having other relations or activities that might influence the article´s content. Forms can be requested to the responsible author or the editorial direction of the Journal.
Funding
The authors declare that there was no funding coming from external sources.
