Research papers
← vista completaPublished on August 30, 2017 | http://doi.org/10.5867/medwave.2017.07.7035
Mortality trend of gallbladder cancer in Araucanía Region, Chile, 2004-2014
Tendencia de la mortalidad por cáncer de vesícula en la Región de la Araucanía, Chile, 2004-2014
Abstract
BACKGROUND Chile has the highest mortality rate for gallbladder cancer in the Andean region. The areas most affected by this cancer are found in southern Chile.
OBJECTIVE To describe the mortality rate trends for gallbladder cancer in the Araucanía region between 2004 and 2014.
METHODS Ecological observational descriptive study. The cases were identified by the codes ICD-10: C-23. The population at risk was obtained from the projections of the National Institute of Statistics of Chile. The mortality rate was modeled using the Poisson regression method, including age, time, and interaction between the two variables. The annual percentage change (APC) was used as a summary measure.
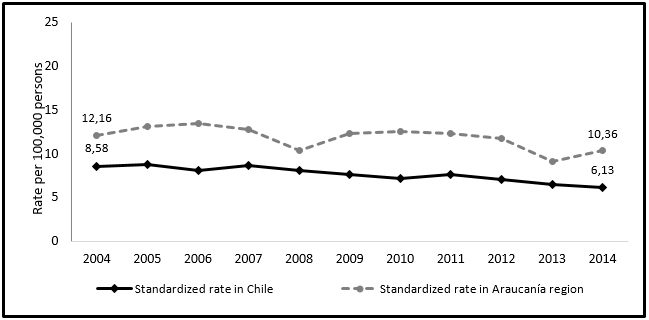
RESULTS In 2014, the Araucanía region had a standardized mortality rate of 10.36 per 100,000 inhabitants, while in the country it was 6.13 per 100,000. At the country level, the temporal evolution of mortality due to gallbladder cancer presented an annual percentage change of 9.1% (incidence rate ratio = 0.91 p-value <0.05), while in Araucanía the decrease was 7 % (incidence rate ratio = 0.93 p-value= 0.16), which is not statistically significant. The mortality rate was 2.68 times higher in women than in Araucanía men (p-value <0.05), a result similar to that of the country. At the national level, the trend according to age group shows a decrease for all groups, being the one of greater magnitude in those people from 45 to 54 years with an annual percent change of -5.36%, these results are not observed in the Araucanía.
CONCLUSIONS Mortality from gallbladder cancer shows a decreasing trend in the period studied for the whole country; however, this is not so for the Araucanía region, which maintains a higher mortality rate than that of the country.
Introduction
Gallbladder cancer has a low incidence at a global level [1]. Chile has the highest incidence rate in the world, as well as of mortality [2]. Between 1998 and 2002 the incidence showed mortality rates of 27.3 per 100,000 inhabitants in women and 12.3 by 100,000 inhabitants in men [3]. According to the first report of population registers of cancer in Chile, in a five-year period, from 2003-2007, the incidence of gallbladder and bile duct cancer in Los Rios region was 10.7 and 32.0 for men and women respectively. In the region of Antofagasta incidence rates were 3.9 and 9.5, and for the province of Biobío these rates were 12.4 and 28.0 per 100,000 inhabitants, men and women respectively. The three regions included in this report, show an incidence rate almost three times higher in women than in men.
On the other hand, the most affected regions are in the south of the country, highlighting the region of the Biobío where the incidence increases in women at 45 years of age and in men at 55 years. In the Los Rios region the risk for women increases in the group of 50 to 54 years and in men at more advanced ages, between 60 to 64 years [4].
Regarding mortality from this cancer, Chile showed a decrease in this specific rate for both sexes from 12.0 to 10.6 per 100,000 inhabitants, between the years 2000 and 2011. Mean standardized rate average for men was 6.2 and for women 16.1 deaths per 100,000 inhabitants, which stands for greater mortality in women than in men [5].
Considering the high mortality and incidence of this cancer in Chile, preventive cholecystectomy of gallbladder cancer is included for symptomatic persons aged 35 to 49 years, within the system of Explicit Health Guarantees (GES) since 2006 [6]. This measure ensures early diagnosis and timely treatment of this condition for this specific age group and beneficiaries of the National Health Fund (FONASA) and the Private Health Institutions (Isapres) of the country. However, according to the literature review, these ages are not the most affected by cancer and its impact would be reflected around 2020, when the beneficiaries meet the age associated with the incidence of the disease [7],[8]. According to the data provided by the National Health Survey (ENS) from 2009-2010, the Region of La Araucanía has the lowest prevalence of abdominal ultrasounds in relation to the Metropolitan Region. A gap is estimated at the country level on potential non-covered demand of 661,217, for the total population (GES beneficiary and non-beneficiary), and in relation to cholecystectomies, non-covered demand would amount to 176,000 people [9].
The greatest concentration of incidental and fatal cases occur in the least developed regions of the world [2]. The main risk factor for this cancer is the presence of gallstones [10]. Herrera et al., showed a greater number of cases of cancer deaths in the population with lower educational level in 2015. This difference was more pronounced for gallbladder cancer [11].
Obesity is another risk factor; Chile has a prevalence of obesity close to or even greater than developed countries like the United States. Obesity contributes through its association with gallstones, increase of endogenous estrogens or its association with fatty cells [12]. Other factors correspond to being from the Mapuche ethnic group, poverty and having had typhoid fever, which are complemented by difficulties of access to hospital care and surgical interventions [13].
This cancer is a silent pathology that only manifests symptoms in advanced stages of the disease; in general its diagnosis in early stages are an incidental finding during the surgical intervention. Survival increases in the earliest stages of the disease, when it has no symptoms, suggesting that prevention of this pathology may be done through preventive cholecystectomy [14].
In Chile, the highest mortality rates are observed in the southern regions, especially in areas with high poverty, large indigenous Mapuche population and insufficient access to health services, including access to surgery for gallbladder diseases [13], factors associated with the Araucanía region.
Due to previous antecedents and its natural history which describes the presence of cholelithiasis as the main risk factor [15] and the low coverage in performing abdominal ultrasounds, which could determine a sub-diagnosis of biliary pathology in the region of the Araucanía, a need arose to perform a study whose purpose is to describe the temporal trend of mortality rate for this cancer in the period 2004-2014.
Methods
A descriptive, ecological observational study was conducted, with the information of mortality by gallbladder cancer between 2004 and 2014, obtained from the records of deaths of the Department of Statistics and Health information of the Ministry of Health of Chile (DEIS) [16]. Death records include the basic cause of death, coded with the tenth International Classification of Diseases (ICD-10). Cases were included if their primary cause of death was defined by codes C-23, corresponding to malignant Tumor of the Gallbladder [17]. The population at risk was obtained from the population projections of each year published by the National Institute of Statistics of Chile [18].
With these data, crude and specific rates for each age group (in five- year periods) were calculated, both from the country and the Araucanía region. Adjusted rates were calculated through the direct method, using the reference population estimated by the World Health Organization (WHO) for 2015 [19].
In order to evaluate trend behavior, a temporal adjustment of mortality rates was made through a generalized linear model with Poisson distribution, using time, age and interaction between them as explanatory variables. Age was grouped in decades, selecting the ages from 35 years, and a Poisson model was developed assuming the existence of a different linear trend of the logarithm of the expected value of mortality rates for each age group [20]. As a summary measure of the temporal trend, the average annual percent change (AAPC) was calculated, using the statistical program Stata 13 [21].
Results
Death records during the 2004-2014 period account for a total of 14,979 deaths from gallbladder cancer in Chile. Of them, 25.54% correspond to men and 74.46 % to women. For the Araucanía region in the same period, a total of 1,218 deaths from gallbladder cancer are recorded, of which 23.97% correspond to men and 76.03% correspond to women.
Figure 1 shows the evolution of the time trend of gallbladder cancer mortality rates between 2004 and 2014. The mortality rate in the Araucanía region is higher than that reported by Chile during the same period. In 2004, Chile reported a rate of 8.58 per 100,000 inhabitants while in 2014, it was 6.43 by 100,000 inhabitants, which implies a percentage of variation of -28.6 %. This percentage for the Araucanía region was-14.7%, so the percentage variation was lower in the region. Figure 2 shows mortality rates according to sex, with a higher mortality rate in females, with more than twice the rate calculated for males.
 Full size
Full size 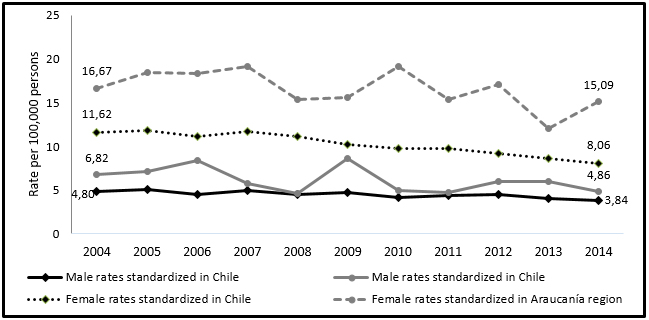 Full size
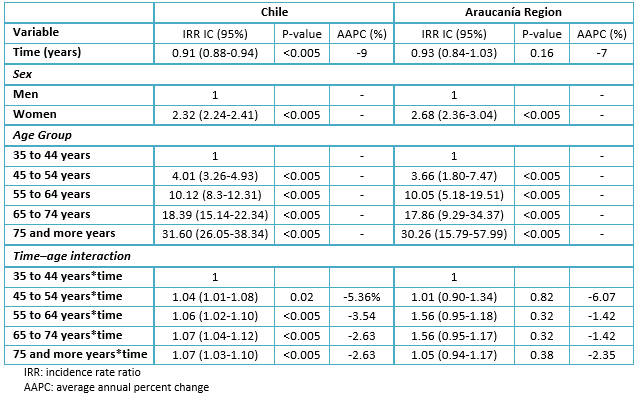
Full size Table 1 describes the results of the Poisson regression model for the mortality rate for gallbladder cancer in Chile. It shows that, at the national level, mortality has decreased with an annual percentage change of 9% (IRR = 0.91 P-value < 0.05), adjusted by sex and age. The mortality rate in women was 2.32 times higher than in men. The magnitude of mortality rates increased with age and was 31.6 times higher in the group of 75 and more years compared to the group of 35 to 44 years. The average annual percent change (AAPC) shows the largest reduction in the group of 45 to 54 years (AAPC =-5.36); the lowest decrease is observed over 65 years (AAPC =-2.63).
In the Araucanía Region, the average annual percent change for the studied period obtained a decrease of 7%, not being statistically significant (IRR 0.93 p-value > 0.05). The mortality rate in women was 2.68 times higher than in men (p-value < 0.05). The average annual percent change (AAPC) does not provide significant results for temporal trend in age groups.
 Full size
Full size Discussion
This study showed that during the period 2004-2014, the rate of gallbladder cancer mortality, standardized by age and sex, has decreased slightly at the country level. However, it should be considered that Chile presented in the years 2003-2007 the highest mortality rate in central and South American countries [22]. In the Araucanía region, the age and sex standardized mortality rates are higher than those in the country. Studies show a great variation for mortality among the regions of Chile.
One of the risk factors corresponds to poverty, according to the results of the latest survey of National Socioeconomic Characterization carried out in 2015 (CASEN-2015), the region of La Araucanía presented a percentage of people in poverty of 23.6%, compared with 11.7% of the total country [23]. Poverty is an important risk factor for gallbladder cancer. Many factors, such as typhoid infection, diet, and access to medical procedures, are related to poverty [13]. The CASEN survey also shows that 32% of people in the region claim to belong or be a descendant of Mapuche people, which is also a risk factor.
By applying the Poisson regression model to assess time trend patterns, the incidence rate ratio (IRR) at the country level shows a decrease of 9% in the average annual percent change. One health goal for 2020 is to reduce mortality from this cancer by 25% [24]. Time trend results in the region of the Araucanía were not significant, that is to say, the trend has remained constant.
At the country level, women presented an average of 2.32 times more risk of dying from this cancer than men. Similar results were obtained in the Araucanía Region, in agreement with the global prevalence, being associated with estrogen levels. A study conducted in India showed that women with early menarche, multiple pregnancies and late menopause would have a higher risk of developing gallbladder cancer [25]. Additionally, estrogens increase the formation of gallstones by increasing biliary cholesterol [26]. Risk analysis by age group showed a significant increase in mortality as the population ages. The group of 75 and older, at country level, presented 31.6 times (IRR = 31.6, 95% CI: 6.05-38.34) more risk of dying from gallbladder cancer compared to the group of 35 to 44 years. This figure is sufficient to consider an expansion in coverage of health interventions at older ages than those currently covered by the System of Explicit Guarantees in Health (GES) [27].
Analyzing the time trend by age group, we observed that the average annual percent change presented statistically significant results, where the greatest decrease in deaths is observed in the group of 45 to 54 years (AAPC =-5.36). In the Araucanía region, the results were not statistically significant, which could lead to the conclusion that the preventive interventions undertaken so far have not yet been effective at the regional level. However, this study does not have sufficient association data to reach this conclusion. According to the data of the Health Superintendence, a total of 4,032,154 cases have been treated between 2006 and 2016, at country level in the 35 – 44 age groups, through GES coverage [28].
Gallbladder cancer is a highly lethal disease with a three years survival less than 20% and five years survival less than 15% [29]. Therefore, an early diagnosis with abdominal ultrasound and its subsequent treatment through surgical intervention could contribute to the reduction of deaths from this cause in Chile and the region [30]. In this sense, M. Gabrielli et al., recommend targeting additional resources for young women living in the highest risk areas, by increasing the age to 64 years in order to detect and treat most of the incipient cancers in this population [29].
This study shows that the Araucanía Region should be considered as a high-risk area of gallbladder cancer within the country, which must be translated into effective measures at both, clinical and health planning levels. In the clinical field, primary health care plays a preponderant role, since it is at this level where people consult for symptoms associated with this disease and where professionals can identify risk factors [31], performing diagnostic suspicion and requesting confirmation studies. This should be reinforced in the health teams of the region as a clinical goal, considering that the region has the lowest prevalence of abdominal ultrasounds in relation to the Metropolitan Region [9]. However, improvements at the clinical level should be accompanied by the incorporation of this disease as a health priority within the region's health services in its annual programming of activities, and implementing the necessary resources to increase the coverage of diagnostic procedures and surgical solution, considering the poverty and geographical difficulties of access present in the region.
A limitation for this study can be related to the quality of the deaths records. In Chile, the exhaustiveness is of 100% of deaths, age registration is complete, certification is carried out by a physician, codification and validation are made on the basis of international standards and the proportion of ill-defined causes of death is lower than 3%, being in most cases, deceased people with ages over 80 years , which could lead to an underestimation of the specific mortality rate in this group [32], but this is maintained within the study period, so it would not transcendentally affect the time trend of mortality rates. Another limitation was the inability to include in the model, other explanatory variables in addition to age and year.
Conclusions
The region presents factors recognized by literature as risk factors such as poverty and Mapuche ethnicity. A group identified as susceptible to developing gallbladder cancer are descendants of Mapuche origin; research has recommended that these populations be educated about this disease [2], evaluating lifestyles and genetic factors [13].
This study concludes that mortality due to gallbladder cancer has remained constant in the Araucanía region, which makes it necessary to plan health interventions that allow an improvement in the prevention of this highly lethal pathology.
Notes
Declaration of conflicts of interest
The authors declare that they have no conflicts of interest with the subject of the report and that they have not received financing for its realization. They also declare not having financial relationships with organizations that may have interests in the published article in the past three years; and not having other relationships or activities that could influence the published article.
Financing
The authors state that there were no external sources of funding.
From the editor
- The authors originally submitted this article in Spanish and subsequently translated it into English. The Journal has not copyedited this version.
- The principal or responsible author states that this manuscript is an honest, accurate and transparent transcription of the study being reported; that no important aspect of the study has been omitted; and that discrepancies between the results of the study and those foreseen (if relevant) have been recorded and explained.
