Estudios originales
← vista completaPublicado el 5 de diciembre de 2017 | http://doi.org/10.5867/medwave.2017.09.7097
Factores asociados a mortalidad intrahospitalaria en pacientes con diabetes mellitus tipo 2: estudio transversal analítico en tres hospitales peruanos
Factors associated to inpatient mortality rates in type-2-diabetic patients: a cross-sectional analytical study in three Peruvian hospitals
Abstract
INTRODUCTION Diabetes mortality has increased in recent years. In Peru, there are few studies on in-hospital mortality due to type 2 diabetes in the provinces.
OBJECTIVE To determine factors associated to hospital mortality in patients with diabetes mellitus type 2 in three hospitals from Cusco-Peru.
METHODS An analytical cross-sectional study was performed. All patients with diabetes mellitus type 2 hospitalized in the city of Cusco during the 2016 were included. Socio-educational and clinical characteristics were evaluated, with "death" as the variable of interest. The crude (cPR) and adjusted (aPR) prevalence ratios were estimated using generalized linear models with Poisson family and log link function, with their respective 95% confidence intervals (95% CI). The values p <0.05 were considered significant.
RESULTS A total of 153 patients were studied; 33.3% (51) died in the hospital. The mortality rate increased when the following factors were associated: age of the patients increased the mortality rate by one-year increments (aPR: 1.02; CI95%: 1.01-1.03; p<0.001); to have been admitted by the emergency service (aPR: 1.93; CI95%: 1.34-2.77; p<0.001); being a patient who is readmitted to the hospital (aPR: 2.01; CI95%: 1.36-2.98; p<0.001); and patients who have had a metabolic in-hospital complication (aPR: 1.61; CI95%: 1.07-2.43; p=0.024) or renal in-hospital complications (aPR: 1.47; CI95%: 1.30-1.67; p<0.001). Conversely, the mortality rate was reduced when admission was due to a urinary tract infection (aPR: 0.50; CI95%: 0.35-0.72; p<0.001); adjusted by seven variables.
CONCLUSIONS A third of hospitalized diabetes mellitus type 2 patients died during the study period. Mortality was increased as age rises, patients admitted through emergency rooms, patients who were readmitted to the hospital, and patients who had metabolic or renal complications. Patients admitted for a urinary tract infection had a lower mortality rate.
Introduction
According to the International Diabetes Federation, it was estimated that 415 million people had diabetes mellitus in the world in 2015 and approximately 5 million people died from this disease [1]. In Peru, more than one million people have diabetes, geographically distributed in each natural region: coast, mountain and forest with prevalence of 8.2%, 4.5% and 3.5%, respectively. The national prevalence is about 7% (among adults over 25 years) [2]. Diabetes mellitus and its complications are among the ten leading causes of death in the world [3]. It is a chronic disease that requires continuous medical checking, which is a problem in spite of having strategies that try to reduce complications endangering the patient's life [4].
Cerebral vascular accidents and acute myocardial infarction are the main causes of mortality in patients with diabetes in countries with high economic income; while infections in lower and middle-income countries [5],[6]. A study conducted in a hospital in India found that there is a greater probability of dying in patients with diabetes when they also have vascular or renal diseases, and infections. In Peru, a study conducted in a general hospital in Lima, described cerebral vascular accident, respiratory infection and acute renal injury as factors associated with mortality in these patients [7]. We have not found reports that describe factors which increase mortality in this type of patients in regional hospitals from Peru, where the resources of the health sector are deficient, medications are limited and the glycemic controls are inadequate [8].
Therefore, the objective of this study was to determine factors associated with intra hospital mortality in patients with diabetes mellitus type 2 in three hospitals located in the southern mountain range of Peru.
Methods
Design and population
An analytical cross-sectional study was conducted, using data from 153 patients with diabetes mellitus type 2 hospitalized during 2016 in the Internal Medicine services from three hospitals in the City of Cusco, located in the southern mountain range in Peru. The hospitals were: Hospital Regional del Cusco, Antonio Lorena Hospital both dependents of the Ministry of Health and the National Hospital Adolfo Guevara Velasco under the Ministry of Labor and Promotion of the Employment of Peru. The latter belongs to the Social Security, an institution for insured workers or their relatives, who receives monetary contributions from its policy holders and has a bigger budget for different activities compared with others health institution in Cusco. The hospitals are third level regional reference hospitals, which also serve patients from other regions of the southern mountain range in Peru and from different socioeconomic conditions. The entire data found in census sampling was used.
Selection of participants
Data from medical records of all patients with diabetes mellitus type 2 (according to the American Diabetes Association) [9] hospitalized in the internal medicine service were included. The disease must have been confirmed by a doctor of internal medicine or an endocrinologist. Patients hospitalized only for performing a diagnostic or therapeutic procedure (renal biopsy, peritoneal dialysis catheter placement, pulses with corticoids, etcetera), and pregnant patients were excluded.
Variables of study
The variable of interest was status at discharge (died or alive) during the study period. To characterize the study population socio educational variables such as sex, age, marital status, education level and place of residence were considered. The hospitalization cause, defined as diagnosis at the time of admission was also considered as a variable. This was subdivided into: infectious (urinary, respiratory, subcutaneous tissue, diabetic foot), metabolic (hypoglycemia, diabetic ketoacidosis, hyperosmotic condition), cardiovascular (cerebrovascular accident and acute myocardial infarction) and renal (acute kidney failure and chronic kidney disease). Finally, we considered comorbidities, intra hospital complications, admission route to the hospital (emergency or doctor's office), length of stay and glycemic control (appropriate if glycosylated hemoglobin was <7% and inappropriate if ≥7%).
Data analysis
A database was developed for each hospital using Microsoft Excel (version for Windows 2013) which later on was revised, depurate and analyzed. To analyze the data we used the statistical program Stata v.11.1 (Stata Corp LP, College Station, TX, USA). A descriptive analysis of categorical variables was made using absolute and relative frequencies, quantitative variables were described through the median and the interquartile range according to the previous evaluation of normality with the Shapiro Wilk test.
Bivariate and multivariate analytical statistics was applied, in which “death” was used as a dependent variable. This was individually combined with each independent variable (bivariate analysis) and afterwards, with all the variables that were statistically significant in the bivariate analysis (multivariate analysis). Both, the crude and adjusted prevalence ratios were calculated with 95% confidence intervals together with the p values. We used generalized linear models, with Poisson family (we used this family because the main variable was dichotomous and allows to obtain prevalence ratios when generalized linear models are applied in analytical cross-sectional studies), log link function, sturdy models and using each hospital as a cluster. The p values <0.05 were considered significant.
Ethical aspects
The study was reviewed and approved by the ethics and research committee of the mentioned hospitals. Names were eliminated from the database after collecting the data of each patient, and an anonymous list was used for the analysis.
Results
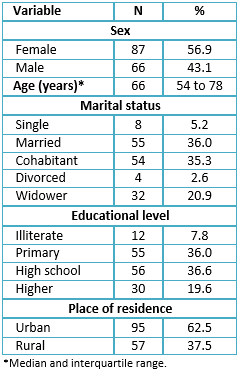
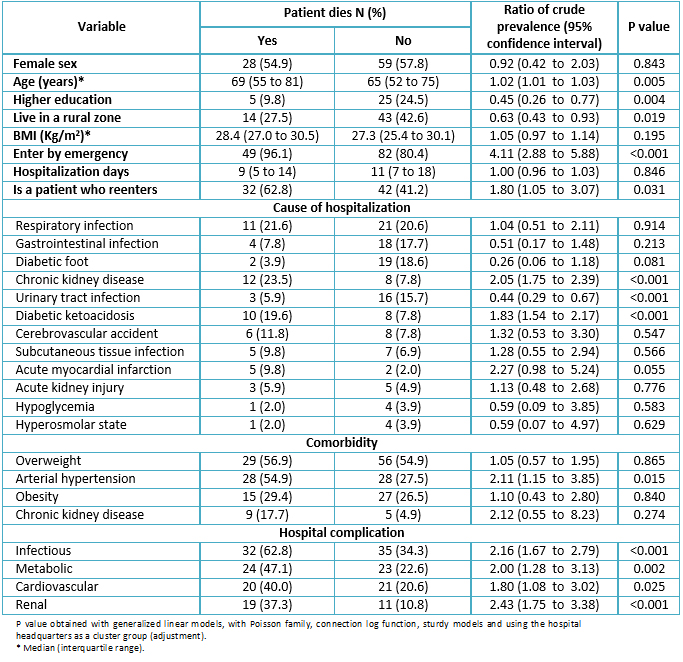
From the 153 patients, 56.9% (87) were female, the median age was 66 years (interquartile range 54 to 78 years old). The main socio-educational results are shown in Table 1.
 Full size
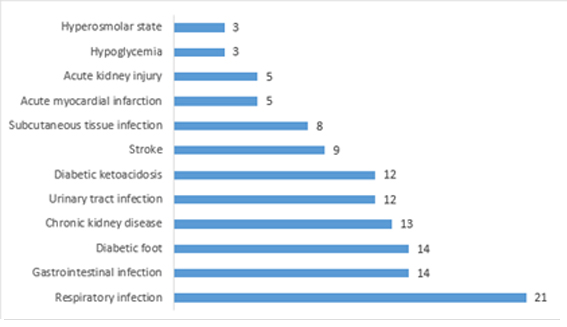
Full size Of all patients, 55.6% (85) were overweight and 27.5% (42) were obese. One hundred thirty one, (85.6%) were admitted from the emergency service and the median length of stay was nine days (interquartile range 6 to 17 days). Seventy four (48.4%) (74) were re-admitted; 14.4% (22) had a glycosylated hemoglobin test of which 95.5% (21) had inadequate glycemic control; 33.3% (51) died during hospitalization. The main cause of hospitalization was respiratory infection (21%), followed by gastrointestinal infection and diabetic foot (14% each) (Figure 1).
 Full size
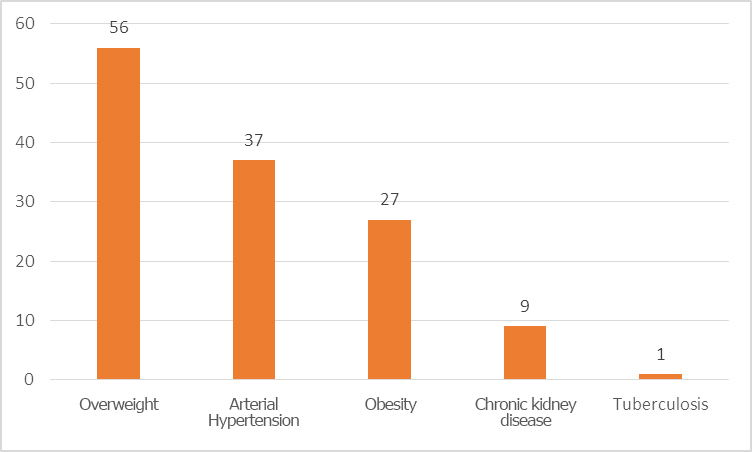
Full size The main comorbidities were overweight (56%), hypertension (37%) and obesity (27%) (Figure 2).
 Full size
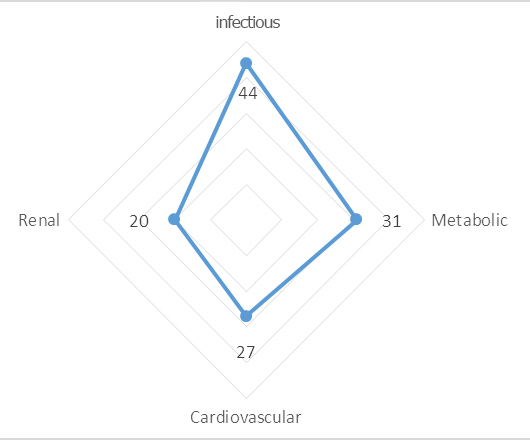
Full size The main complication during hospitalization was an infection (44%), followed by metabolic complications (31%) and cardiovascular complications (27%) (Figure 3).
 Full size
Full size In the bivariate analysis, we found that factors associated with a higher mortality were: age (p=0.005), being admitted through the emergency service (p<0.001), being a patient readmitted to the hospital (p=0.031), chronic kidney disease (p<0.001) or diabetic ketoacidosis (p<0.001) as admission cause and having an infectious (p<0.001), metabolic (p=0.002), cardiovascular (p=0.025) or renal (p<0.001) complication during hospitalization. On the other hand, the highest level of instruction (p=0.004), living in a rural area (p=0.019) and being admitted for a urinary tract infection (p<0.001) were related to decreased mortality (Table 2).
 Full size
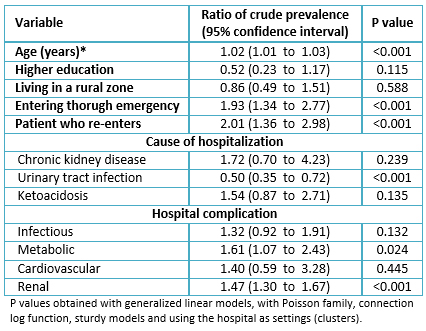
Full size According to multivariate analysis, variables associated with a higher mortality were: age (adjusted prevalence ratio 1.02, 95% confidence interval 1.01 to 1.03, p value <0.001), admission through the emergency department (adjusted prevalence ratio 1.93, 95% confidence interval 1.34 to 2.77, p value <0.001), being a patient who re-enters to the hospital (adjusted prevalence ratio 2.01, 95% confidence interval 1.36 to 2.98, p value <0.001) and having an inhospital metabolic (adjusted prevalence ratio 1.61, 95% confidence interval 1.07 to 2.43, p value = 0.024) or renal (adjusted prevalence ratio 1.47, 95% confidence interval 1.30 a 1.67, p value <0.001) complication. Conversely, mortality decreased when the cause of hospitalization was urinary tract infection (adjusted prevalence ratio 0.50, 95% confidence interval 0.35 to 0.72, p value <0.001). All these variables were adjusted by educational level, place of residence, chronic kidney disease or diabetic ketoacidosis as cause of admission. Having an inhospital infectious or cardiovascular complication and for the hospital (table 3).
 Full size
Full size Discussion
During the study we observed that mortality increased with age, possibly due to the complications which older people are prone to. This is similar to what we found in other reports [10],[11], where being over 60 years old can be an independent factor associated with complications and mortality [11]. This should be reason to create programs for older people in order to provide more medical advice, diagnosis and support to this group of patients.
Entering through an emergency department increased mortality, a fact that demonstrates the importance of complications generated by this type of admission. Diabetic patients have more risk of dying when they are admitted for urgent reasons [12] particularly if complications are acute such as hyperglycemia, which is one of the most frequent reasons for emergency admission [13] that can even cause the patient´s entrance to the intensive care unit [14],[15]. It also may provoke an extended hospital stay thus increasing healthcare costs [13]. However, in a study made in a general hospital in Lima-Peru, such an association was not found, possibly because of the heterogeneous population compared with ours [7]. We recommend to carry out more studies about reasons for admission and their repercussions in diabetic patients.
Patients who had had previous admissions had a higher mortality rate, possibly for the higher severity and chronicity of complications; this is also reported by a study in Mexico [16], which attributes the most frequent intra hospital complications to infections, hypoglycemia and cardiovascular diseases. This is similar to other Peruvian reports [17],[18].
Patients who presented an inhospital complication of metabolic type had a higher mortality. This is similar to a hospital in India, which indicates that presenting metabolic complications increases the risk of death more than infectious complications [19]. This complication has increased in Peru over the years, especially in older people, raising the mortality rate [20]. Furthermore, an inadequate metabolic control would cause the development of late complications and thus a greater number of comorbidities [17].
Likewise, those with a renal inhospital complication had a higher mortality. This is possibly due to the complications of the kidney disease [21]. Kidney disease affects 20-40% of patients with diabetes, which is also the main cause of end-stage renal disease [22]. This complication is also reported in Peruvian hospitals [7],[18], considering it an important cause of mortality in this population [7],[17]. This pathology has a strong correlation with the condition of arterial hypertension (due to the kidney´s regulation function), for this reason we avoided to include this variable in the multivariate model, but it is known that it is also very important and should be studied separately.
Finally, those who were admitted for a urinary tract infection had a lower mortality, possibly due to an adequate handling in this type of pathology and for its lower complexity. However, there are reports that mention that diabetic patients have a higher risk to acquire complicated urinary tract infections [23], being a frequent reason for admission in Peru [7],[17] and in other countries [24],[25]. We suggest conducting research that shows the most frequent type of urinary infection and its impact on hospitalized diabetic patients that, despite not causing a higher mortality, can have other repercussions on the patient.
Limitations
The study has the limitation of being based on data from medical records and having a limited population. Despite this limitation, the results are important because it is the first study made in a hospital in this region of Peru which evaluates mortality in hospitals with socioeconomically different populations.
This fact presents us a general overview of the problem and allows us to open the field of research about this subject where there are few studies, especially in countries with medium and low income, and where the nutritional status and the epidemiology transition are different. This could cause that this reality changes in the coming years.
Conclusions
According to the results we concluded that: age, emergency admission and re-admission to hospitalization were factors associated with mortality in the study population as well as presenting intra hospital complications of metabolic or renal type. However, presenting urinary tract infection as a cause of hospitalization decreased the probability of mortality.
Notes
From the editor
The authors originally submitted this article in Spanish and subsequently translated it into English. The Journal has not copyedited this version.
Of the authors
The authors make available the databases to serve the scientific community, this is done in the publication as an attachment in https://doi.org/10.6084/m9.figshare.5606041.v1 .
Ethical aspects
The Journal is aware that the study was reviewed and approved by the ethics and research committees of: Hospital Regional del Cusco, Hospital Nacional Adolfo Guevara Velasco and Hospital Antonio Lorena, in addition to removing the names from the database after collecting each patient's data and using an anonymous list for analysis.
Declaration of conflicts of interest
The authors have completed the ICMJE Conflict of Interest declaration form, and declare that they have not received funding for the report; have no financial relationships with organizations that might have an interest in the published article in the last three years; and have no other relationships or activities that could influence the published article. Forms can be requested by contacting the author responsible or the editorial management of the Journal.
Financing
The authors state that there were no external sources of funding.
Editor's note
The principal or responsible author asserts that this manuscript is an honest, accurate and transparent transcription of the study being reported; that no important aspects of the study have been omitted; and that discrepancies between the study results and those anticipated (if relevant) have been recorded and explained.
