Estudios originales
← vista completaPublicado el 26 de abril de 2019 | http://doi.org/10.5867/medwave.2019.03.7617
Reconocimiento de trastornos de salud mental en adolescentes escolarizados: estudio descriptivo
Recognition of mental health disorders in adolescent students in Chile: a descriptive study
Abstract
Objective To describe high school students’ ability to recognize six mental health disorders.
Method This is a descriptive, cross-sectional study. Participants were teenagers between 14-19 years of age, high-school students from the town of Talca, in the Maule Region (Chile). In order to examine the recognition of mental health issues, six vignettes were used, each describing a teenager showing symptoms of six different problems (stress, anxiety, depression, suicidal thoughts, alcohol abuse, and psychosis). The vignettes are part of the general help-seeking questionnaire for mental health problems in adolescents (vignette version). Participants were instructed to read the vignettes and then answer the question: what do you think is happening to them? The descriptive analysis mainly considered frequencies and percentages.
Results The vignette questionnaire was administered to 400 adolescents of both genders between 14-19 years of age (Mean = 15.73 years). The topic most recognized by the participants was the abuse of alcohol, while anxiety was the least recognized. Women showed a greater tendency to recognize all mental health issues, being the topic of alcohol abuse the one showing the most differences in recognition, with 56.6% of female adolescents recognizing the problem and 41.4% of males identifying it.
Conclusions In general, results showed low levels of ability to recognize mental health disorders among participating adolescents. Female adolescents and participants of subsidized educational establishments tended to better acknowledge the different problems presented.
|
Key ideas
|
Introduction
Despite the fact that adolescence comprises an age group in which good health predominates, it is estimated that mental health disorders and risk behaviors affect as many as 20% of young people worldwide [1]. In Chile, evidence of these problems has emerged in the national health survey, in which 12.2% of adolescents 15-19 years old reported risky alcohol consumption [2], and in the 8th national youth survey (2015), in which 1 out of 4 adolescents reported having felt sad, discouraged, or depressed in the last month. In addition, research shows that adolescents do not tend to seek out professional help for mental health problems [3]. One of the barriers to mental health help-seeking is low mental health literacy [4].
The concept of mental health literacy was introduced in 1997 by Jorm , who defined it as ”knowledge and beliefs about mental disorders which aid their recognition, management or prevention”[5]. Characteristics of mental health literacy were defined as 1) the ability to recognize specific disorders, 2) knowledge of how to seek mental health-related information, 3) knowledge about risk factors and causes of the disorders, 4) knowledge about self-help and the availability of specialized help, 5) attitudes that promote appropriate help-seeking, and 6) attitudes that promote the recognition of mental health problems [6].
Various studies have shown that mental health literacy is a determinant of mental health status in adults[7],[8] and adolescents[9],[10], and, due to earlier help-seeking as a result of mental health literacy, there is an association between level of mental health literacy and mental health status[6]. Some studies have shown that incomplete mental health literacy constitutes a major barrier to seeking help and accessing professional mental health services in these age groups[3],[4], and that low levels of mental health literacy are associated with higher rates of depression[6].
One indicator of mental health literacy is the ability to recognize mental health disorders and their symptoms[5]. Recognition of mental health disorders is often defined in studies as the ability to identify and name a mental health disorder based on symptoms described in a vignette[11].
Most research in adolescents assessing recognition of mental health disorders has found that this age group has difficulty identifying these types of health problems[6],[12],[13] For example, a transversal study by Coles et al.[12] that assessed knowledge and beliefs about mental health in U.S. high school adolescents, using vignettes, found that 1) only 40% recognized depression, 2) only those with a higher level of knowledge mentioned seeking professional help for a mental health problem, and 3) only 1% recognized anxiety. Some studies carried out under this same methodology have reported higher rates of disorder recognition in adolescents. For example, the Loureiro study conducted in Portugal in a large sample of youth 16-24 years old found that 67% could identify symptoms of depression[14], and a study of Chinese adolescents found high levels of recognition for alcohol abuse (58.2%), with much lower recognition levels for depression (16.1%) and anxiety (15.5%))[13].
Other research has assessed the ability of young people to recognize symptoms of schizophrenia and psychosis. A study in Portuguese adolescents[14] found moderate levels of schizophrenia recognition (42.17%) and low-to-moderate levels of psychosis recognition (22.21%). Therefore, at the international level, there is some evidence that adolescents have the ability to recognize various mental health disorders, and that depression tends to be the one recognized most easily.
While several studies have assessed adults’ ability to recognize mental health disorders[12],[13],[15],[16], research on this ability in the adolescent population is limited, although interest in this topic, and recognition of its importance, across multiple cultures, has been increasing systematically[15],[17],[18],[19]. Unfortunately, no prior research was found on adolescent’s ability to recognize mental health disorders in the Chile’s socio-cultural context.
The objective of this study was to describe adolescents’ ability to recognize mental health disorders and their symptoms using a sample of Chilean high school students.
Methods
Design
This study was exploratory and descriptive, as the main research objective was to identify recognition of mental health disorders in mid and late adolescence. It was also transversal, as the data correspond to specific moments in time.
Population and sample
The total population included 17 736 adolescents enrolled in secondary schools in the town of Talca in Chile’s Maule Region. Non-probabilistic convenience sampling was used to collect responses. The minimum required sample to ensure a 95% confidence level and 5% margin of error was 377, with an assumed maximum variance of 50%. The final sample surpassed the minimum sample size, with data collected from 400 adolescents. Sampling was designed to look for homogenous distribution by adolescence sub-stage (mid versus late).
Potential study participants were identified at eight high schools. The schools were selected based on their administrative and financial structure, to ensure representation of all types of secondary schools in Chile. Four of the eight schools declined to participate in the study for internal administrative reasons. Of the four institutions that agreed to participate, one was municipal (i.e., financed and managed by the State, with local administration) and three were private (higher-socioeconomic-level) schools that received government subsidies (i.e., financial support from the State). The socioeconomic classification of the schools was based on criteria determined by Chile’s Ministry of Education for different types of educational institutions using assessment tests on quality of learning and the student vulnerability index [20]. Approximately 20 students per school did not respond to the survey due to lack of parental consent for their participation in the study.
Variables
The study’s primary research variable was mental health literacy, defined as recognition of mental health disorders and symptoms. To determine if mental health literacy varied by the demographic characteristics of the study sample, data on gender, age group (mid versus late adolescence), and type of school (municipal versus subsidized private) were also collected.
Instruments
To assess mental health symptom recognition, we used the vignette version of the General Help-Seeking Questionnaire (GHSQ-V)[1], adapted for Chile. This instrument is used to assess adolescents’ willingness to seek help from specified professional mental health resources and their ability to identify seven different types of health disorders (stress, anxiety, depression, suicidal ideation, alcohol abuse, psychosis, and a physical illness). Each question includes a vignette in which an adolescent displays symptoms of one of the seven health disorders. To assess mental health literacy, participants are asked to read the vignette and then answer the question “What do you think is happening to him/her?” (survey item “K”). The participant is instructed to name and describe the disorder indicated by the symptoms shown in each vignette, in writing. The answers are then scored as “1” (“recognizes”) or “0” (“does not recognize”). An additional questionnaire was then administered to each participant to gather socio-demographic data, including age group, gender, current level of education, and type of school (municipal versus private subsidized, to determine socioeconomic status based on the Ministry of Education classifications).
Ethical aspects
After obtaining authorization for participation in the study from the four secondary schools, informed consent was requested from the study participants. The questionnaires were administered in high school classrooms by psychologists trained in their deployment. This study was approved by the ethics committee of the Universidad Católica del Maule.
Analysis
The initial statistical analysis generated absolute and relative frequencies (percentages) for sample characteristics by participant gender and age. Criteria for mental health literacy were described and measured as absolute and relative frequencies and sorted by mental health disorder, gender, school type, and adolescence sub-stage (14-15 years or mid adolescence versus 16-19 years or late adolescence). The number and percentage of adolescents recognizing the six mental health disorders described in the vignettes were then calculated. The remaining data were excluded from the analysis.
Results
Sample characteristics
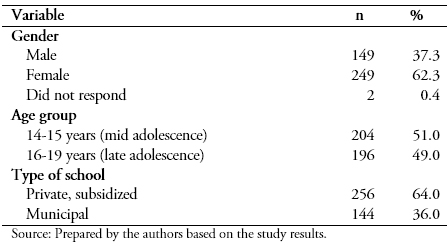
The final sample included 400 adolescents 14-19 years old (M = 15.73; SD = 1.4). A total of 249 participants were female (62.3%) and 149 were male (37.3%). Table 1 shows the distribution of selected sample characteristics (gender, age group, and type of school).
A total of 233 participants (58.3%) had a mid-low or low socioeconomic level and 167 (41.7%) had a mid socioeconomic level. A total of 144 (36%) studied in municipal schools and the remaining 256 (64%) studied in private schools that receive government subsidies.
 Full size
Full size Recognition of mental health disorders by gender
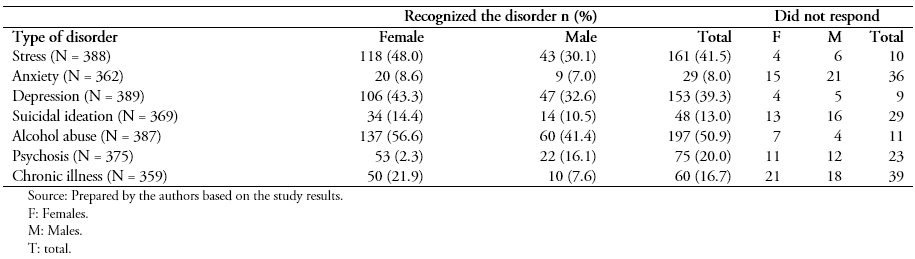
A descriptive analysis of participants’ recognition of six mental health disorders (stress, anxiety, depression, suicidal ideation, alcohol abuse, and psychosis) and one physical health problem (chronic disease) was carried out and expressed in percentages by type of disorder and gender of the adolescent study participant. As shown in Column 4 of Table 2, only 161 (41.5%) of 388 adolescents (118 females (48.0%) and 43 males (30.1%)) recognized stress disorder. The last column in Table 2 shows the total number of participants that did not respond to the standard question assessing recognition of the various health disorders. For example, four females and six males did not respond to the standard question for identifying stress.
Table 2 shows the overall low level of recognition of the six mental health disorders and the physical health problem. The proportion of participants that recognized the disorder was particularly low for anxiety, suicidal ideation, psychosis, and chronic disease. As shown in Table 1, females showed a higher level of recognition of all six mental health disorders compared to males. This difference between males and females was also observed for the physical health problem.
 Full size
Full size Recognition of mental health disorders by age
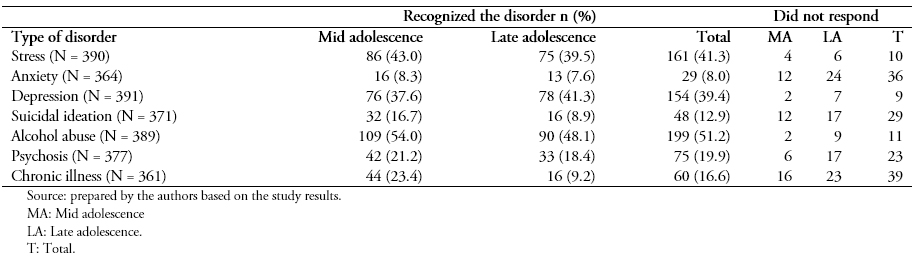
Participants’ level of recognition of each health disorder was also characterized by age. As shown in Column 2 in Table 3, 86 participants in mid adolescence (14-15 years old) (43%) recognized stress disorder.
As shown in Table 3, participants in mid adolescence tended to have a higher level of recognition of all mental health disorders except depression compared to those in late adolescence (16-19 years old). This difference was also observed for recognition of the physical health problem.
 Full size
Full size Recognition of mental health disorders by school type
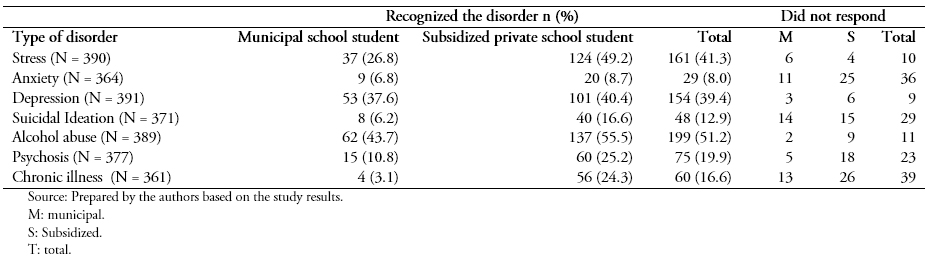
The third part of the analysis entailed characterization of participants’ recognition of the health disorders by type of school (municipal or subsidized private). As shown in Column 2 in Table 4, 37 adolescents from municipal schools (26.8%) recognized stress disorder.
As shown in Table 4, adolescents from subsidized private schools tended to have a higher level of recognition of the six different mental health disorders than adolescents at municipal schools. This difference was also observed for recognition of the physical health problem.
 Full size
Full size Discussion
This research assessed adolescents’ ability to recognize six mental health disorders using a sample of high school students in Chile. The results show an overall low level of disorder symptom recognition. Of the six mental health disorders described in the vignette questionnaire, alcohol abuse was the one recognized by the most adolescent study participants (50.9%), followed by stress (41.5%), depression (39.3%), and psychosis (20%). The least recognized disorders were suicidal ideation (13%) and anxiety (8%). These results match those from similar studies conducted with both adolescent and general populations in which psychoactive substance consumption was reported as one of the most recognized disorders[13].
In this study, alcohol abuse was the most recognized disorder in this study (and the only one recognized by at least half of the study sample). This might be explained by the fact that alcohol and drug abuse has been addressed in Chilean secondary schools for decades, mainly via prevention programs developed by the National Service for the Prevention and Rehabilitation of Drug and Alcohol Use (SENDA)[21]. These types of programs have not been carried out for other mental health disorders, however, which may be reflected in the very low level of recognition of these issues among the adolescents in this study (e.g., only 8% recognized anxiety). Given that depression and anxiety disorders are among the most prevalent mental health disorders in adolescents in Chile, this is an important finding.
The results found in this study show that the ability of Chilean adolescents to recognize depression, for example, is similar to that of U.S. adolescents[12], higher than that reported for adolescents in China (where only 16.1% recognized the disorder) [13], and lower than that shown by adolescents in Portugal (where 67% recognized the disorder[14]). Recognition of anxiety was very low for the Chilean adolescents in this study and among their North American peers (8% and 1% respectively), while Chinese adolescents reported higher recognition of the disorder (15%). These results show the variability in the available evidence regarding the ability in adolescents to recognize mental health disorders and symptoms, all of which could have cultural influences[22].
It is interesting that female adolescents in Chile showed a higher level of recognition of all six mental health disorders described in the vignettes compared to males, a result that has been shown in other studies of the adolescent population[9],[19],[23]. One possible explanation for the different levels of recognition by gender is that female adolescents tend to have more experience with mental health disorders and symptoms, especially depression[24]. Females’ tendency to show more empathy than males[25] might also play a role in the higher level of recognition of mental health disorders they reported in this study. Evidence of a relationship between empathy and mental health literacy was found in a study of university students by Furnham & Sjokvist[26]. The results showed that youth with higher levels of recognition of the mental health disorders described in the questionnaire vignettes scored higher in empathy, had studied psychology, and had had more personal experience with mental health disorders than those who with lower levels of mental health disorder recognition.
Given the low level of mental health disorder recognition among Chilean male adolescents found in this study, it seems worthwhile to consider promoting the ability to recognize these symptoms in this group.
The higher level of mental health disorder recognition shown by adolescents from the private subsidized schools compared to those from the municipal schools has been shown in previous studies[17] and might be related to the higher education level of their parents and/or better access to mental health services. One possible explanation for the better ability of students in mid adolescence to recognize mental health disorders such as suicidal ideation compared to those in late adolescence is that the latter group tends to have a greater perception of stigma[27],[28] and shame[29] related to mental health issues, which could create barriers to 1) recognizing and/or reporting them and 2) efforts to seek professional help for them.
The strengths of this research include the fact that it is the only study conducted in Chile examining recognition of common mental health disorders in non-counseled adolescents enrolled in secondary schools, and one of only a few conducted in the Latin American adolescent population.
The limitations of this research included the transversal and non-probabilistic nature of the study, which reduced the possibility of generalizing the results. The fact that the study was carried out in one specific zone of Chile’s Maule region also limits its external validity and generalization. More studies on mental health recognition are needed, using different population samples, to fill this gap. While the use of fictitious cases to assess mental health literacy could be seen as another limitation, the use of vignette-based survey instruments is a common methodology for studying recognition of mental health disorders and symptoms[11],[29].
The results obtained in this research underscore the need to increase Chilean adolescents’ level of knowledge about various mental health disorders, especially the most common ones, such as anxiety and depression. Improving mental health literacy in adolescents will help members of this age group recognize various mental health disorders and thus increase the possibility that they may seek help in a timely manner if they are suffering from any of these conditions. This should in turn increase their well-being and reduce the potentially harmful consequences of not receiving specialized attention for mental health issues. Promoting mental health literacy and recognition of symptoms of mental health disorders in the non-counseled, student population will allow for the systematic promotion of better overall health, as reported in some international research[9],[10].
Conclusion
This study shows the diminished ability of participating high school students from Chile to identify mental health disorders based on the symptoms described in a standard vignette questionnaire. Participants from subsidized, private (i.e., higher-socioeconomic-level) schools showed better recognition of the mental health disorders described in this study compared to adolescents from municipal schools. Likewise, female adolescents, when compared to males, tended to recognize mental health disorders better. These results suggest the need to make adolescents literate in symptoms of various mental health disorders in order to increase their timely recognition.
Notes
Roles and authorship contributions
CO: conceptualization, methodology design, direction and administration of the project, research, data management, manuscript preparation (development of the original draft), writing (revision and edition), allocation of resources for the research.
CM: formal analysis, methodology, data presentation, manuscript preparation (development of original draft), writing (revision and edition).
Declaration of conflict of interest
The authors have completed the ICMJE declaration of conflict of interest form. The instrument used can be requested by contacting the author responsible.
Financial disclosure
The present research is part of the Fondecyt initiation project results 11130473, financed by the National Committee of Scientific and Technological Research, Chile.
Ethical aspects disclosure
The primary study from which one of the databases was used was checked and approved by the Scientific Ethics Committee of the Universidad Católica del Maule (Act of Approval 07/2013). The database in this study is not available in any data repository.
