Research papers
← vista completaPublished on March 7, 2022 | http://doi.org/10.5867/medwave.2022.02.002096
Overview of traditional medicine in the Muisca Reserve of Cota, Colombia: A cross-sectional study
Panorama de la medicina tradicional en el Resguardo Muisca de Cota, Colombia: estudio transversal
Abstract
Introduction The Muisca Indigenous people in Cota, Colombia, has committed to reviving and strengthening their traditional culture, including the ancestral knowledge associated with their traditional medicine.
Objective To explore the occurrence of traditional medicine and factors associated with its use among the Muisca people in Cota, Colombia.
Methods A participatory cross-sectional study applied a questionnaire to 471 Muisca mothers who had at least one child over 10 in April 2019. The 44 questions inquired demographic, social, and cultural factors of participants and their knowledge, use and practice of traditional medicine. We used the Mantel-Haenszel procedure to measure the associations using Odds Ratio and 95% confidence intervals.
Results 66.2% (312/471) of the mothers knew at least three cases of traditional diseases; 56.8% (267/470) had and used medicinal plants; 15.8% (73/462) had practiced traditional self-care for flu, menstruation and postpartum; and 11.8% (54/458) reported that they had gone to midwives, bonesetters and healers. Four factors had a significant association (p < 0.05) with traditional medicine: consumption of three traditional foods; having traditional gardens and plants; living within the reservation; and parents born in a municipality of indigenous influence.
Conclusions The study showed that the permanence of traditional medicine is strongly associated with traditional food, agricultural vocation and the possession and use of medicinal plants. The results suggest that the strategy for the recovery of traditional medicine could focus on promoting a stronger link between indigenous identity, territory, food and health.
|
Main messages
|
Introduction
When the conquerors arrived, the Cundiboyacense highlands were inhabited by a large indigenous Muisca population of the Macrochibcha linguistic family. This population was one of the most socially organized in the American continent along with the Incas in Peru, the Tayrona in the Sierra Nevada of Santa Marta, and the Mexica in the Mesoamerican highlands [1].
Unlike many others in the Americas, the Muisca population did not offer strong resistance to the conquerors. This peaceful mentality resulted in a rapid subjugation, but allowed them to continue their agricultural and handicraft traditions. However, the shamans were severely persecuted, and the medical and religious institutions disappeared, leaving few traces in the following generations. The Chibcha language was replaced by the Spanish language, although today, some words of Muisca origin are preserved in the popular speech. Ritual, religious and cultural manifestations did not survive either, and today we find mestizo folklore with significant influence of European traditions. The severe acculturation that occurred during the first centuries challenges finding differences between the mestizo peasants and the indigenous groups. According to the 1919 census, only 14% of the population in the departments of Cundinamarca and Boyacá identified themselves as indigenous [2].
Some Muisca groups maintained small collective territories in municipalities near Bogotá, Chía, Cota, Sesquilé, Suba, and Bosa [3]. The indigenous reserve in Cota was first recognized in 1975 and ratified in 2018 [4]. It has maintained kinship ties and cultural identity, despite the gradual process of acculturation [5]. With about 3300 inhabitants, their governance is maintained through the indigenous Council. Nevertheless, about half of the inhabitants live outside the collective territories and intermingle within the urban and rural population of the municipality.
Little is known about the Muisca’s traditional medicine. By the 19th century, medical specialists, particularly jeques or shamans, had disappeared [6]. Still, some traditions persist today, primarily through medicinal plants [7], traditional midwives, sobanderos, and the knowledge of diseases typical of the ancestral cultural nosology [8]. The inhabitants of the Muisca reserve of Cota recognize the loss of their cultural identity and traditional knowledge. Despite this loss, through the constitutional recognition of Colombia’s multiethnic and multicultural character and the worldwide indigenous movement, Muisca people have undertaken a process of cultural recovery over the last 30 years. This recovery includes studying and teaching Muisca language and rescuing traditional production systems and cultural practices. Now, they are recovering and strengthening ancestral knowledge related to traditional medicine. To achieve this, Muisca people need to understand the role of traditional medicine in their community and what factors have influenced its permanence.
The World Health Organization (WHO) has called to recognize and value traditional medicines [9], as well as the right of indigenous peoples to maintain their health practices [10]. In Colombia, a constitutional mandate seeks to provide a differential ethnic approach to health [11]. The health secretary of the municipality of Cota supported this initiative through an agreement and the participation of the Center for Intercultural Medical Studies. This institution is a non-governmental organization with experience in research and extension projects with various indigenous communities in Colombia.
We conducted an observational epidemiological study to answer the following question: What is the prevalence of traditional medicine, and the demographic, social, and cultural factors associated with the validity or loss of traditional medicine in the Muisca indigenous reserve of Cota? It is necessary to understand that studying traditional health systems requires different strategies, given that their epistemological framework differs from Western medicine. The WHO has proposed general guidelines for research methodologies and evaluation of traditional medicine. To this end, it has insisted that "the lack of research data is due not only to health care policies but also to the lack of an adequate or accepted research methodology for evaluating traditional medicine" [12].
In this research, the indigenous people contributed at all stages. The study followed the ethical principles of medical research in indigenous communities [13]. The results could allow the Muisca community of Cota to have tools to inform its own planning process. This will include updating their life plan to
propose pertinent actions to recover and strengthen their traditional health system based on epidemiological data.
Methods
We conducted a cross-sectional study to explore the knowledge, resources and practices of traditional medicine and their association with some social, demographic, and cultural factors in the Muisca community of Cota (Cundinamarca). In order to address the research question, we carried out several night sessions of intercultural dialogue, with the presence of the indigenous council and the representatives of the health commission. In this way, they indicated questions about resources, practices, practitioners, and knowledge of Muisca traditional medicine that were considered essential to investigate. These questions included foods, diseases, and treatments with medicinal plants.
Participants
The target population was the Muisca indigenous community of the municipality of Cota, with approximately 3300 people gathered in 700 families. We obtained a convenience sample, given the accessibility and proximity of the subjects for the interviewers.
We conducted a household survey applied to mothers of families with at least one child over ten years of age. We took into account that women are primarily responsible for self-care for health. Having a child older than ten years means that the mother has had more opportunities to experience events such as menstruation, puerperium, and childhood flu.
Selection bias was likely since the surveys were conducted at home and women who did not study or work outside the home were more likely to be included. The surveys were conducted on a flexible time schedule to address this bias, including evenings and weekends.
Information bias was also possible since the survey was carried out within a program to recover traditional indigenous medicine. For this reason, an overestimation in the report of traditional knowledge, resources, and practices could be expected, especially if the respondent was an older person.
Variables of interest
We considered some demographic, social, and cultural factors as exposure variables based on information obtained from previous studies on traditional medicine [14].
a) Demographic and social factors included schooling, occupation of the respondent and partner, persons in the household who have steady jobs and receive salary, housing, and population density.
b) Cultural factors included traditional foods, vegetable gardens and traditional plants, dwelling’s location (inside or outside the reserve), and local and indigenous ancestry.
Concerning the investigation of traditional foods, they chose three: chucula (a hot drink made from a mixture of cocoa and cereals), mazamorra (a soup prepared with corn), and envueltos ( a food prepared with tender corn dough). Regarding traditional plants, they chose tallos (Brassica oleracea var. acephala), a type of cabbage planted for food in the Cundiboyacense highlands, and diosme (Coleonema album), a common plant in traditional vegetable gardens, planted for cultural purposes.
Also, in the investigation of cultural factors, it is known that racial and cultural miscegenation has been a gradual process since the conquest. For this reason, it is almost impossible to determine who holds 100% indigenous ancestry and who holds racial miscegenation. For this purpose, we asked about the birthplace of the father and mother. Although the answer does not guarantee the degree of miscegenation, we assume that those born in Cota or neighboring municipalities (that historically have had a Muisca population) are more likely to demonstrate their indigenous ancestry.
We also explored the occurrence of traditional medicine. We considered different resources, practices, attending traditional practitioners and having knowledge of traditional diseases, identified by the community as part of their culture from their traditional knowledge:
a) Traditional resources: cultivation of medicinal plants, consumption of aromatic plants in general and medicinal plants for health care, and use of wild plants.
b) Traditional medicine practices: traditional health care for events such as flu, menstruation and puerperium, placenta burial, and herbal baths or wahes of the home.
c) Traditional medicine practitioners: visit to traditional midwives, sobanderos (bonesetter), and healers. We also asked if they considered these specialists were needed in the community.
d) Knowledge of traditional diseases according to cultural nosology in the indigenous tradition of these peoples. In consensus with the community members, we asked about five (descuaje, internal fever, fallen womb, frio del difunto, and sereno).
Data collection
We designed a data collection instrument with 44 questions. We conducted a pilot study with 10% of the expected sample to verify the comprehension of the instrument and the proper use of the mobile devices. We conducted the pilot test in the indigenous reserve of the neighboring municipality of Chía, because it has similar demographic, social, and cultural characteristics. The pilot followed the same procedures of the survey, except for the sample size, and was applied in 30 households. Trained women administered the surveys to facilitate communication with the respondents, especially regarding women’s health. The survey took place in April 2019. We used Google forms with real-time data capture through mobile devices.
Data analysis
The information was processed using the CIETmap statistical program for univariate, bivariate, and multivariate analysis [15].
For univariate analysis we used proportions of events for dichotomous variables or averages with standard deviation to describe the sample. In order to establish the compatibility of the data with possible associations between exposure and outcome variables, we used the Mantel-Haenszel procedure. We used this procedure as part of our exploratory objective, aware of the low external validity due to the nature of convenience samples.
For the bivariate analysis, we generated dichotomous variables, some based on the mean and others on binomial categories defined with the representatives of the community. We contrasted these variables with each traditional medicine outcome (resources, practices, practitioners, and knowledge). In addition, we calculated odds ratios with 95% confidence intervals to describe their possible relationship with demographic, social, and cultural factors.
To explore the independence of the relationships between variables, we conducted a multivariate analysis with the variables that showed a p-value lower than 0.05 in the bivariate analyses.
Ethics and community Participation
Although this project involved human participants, it was considered that the instrument did not ask sensitive information. Therefore, the study was in the category of research with minimal risk, according to Resolution No.8430 [16].
The study followed a participatory research approach that sought to involve the communities throughout the process of knowledge generation, from the research question, and discuss the results to improve their living conditions. The direct participation of community members followed the principles of benefit, active participation, and training and capacity building established by the Traditional Health Systems Study Group [13].
A member of the community was involved as a field coordinator. She received additional training to make her role increasingly active in the research’s design, implementation, analysis, and evaluation components. In addition, the interviewers were selected in agreement with the indigenous community authorities. The procedures for conducting the survey were also defined in coordination with them.
The Center for Intercultural Medical Studies coordinated the study with the authorities of the indigenous reserve, and a community agreement was signed for research and informationsharing agreement. Individual informed consent was requested from the participants, guaranteeing anonymity and confidentiality. The results were formally presented at a community meeting, and signed permission was obtained to authorize their publication in this article.
Considering that the population corresponds to an ethnic minority, the above ethical considerations seek to protect the rights and welfare of this community, in addition to the fact that no judgments are made about their knowledge or practices [17].
Results
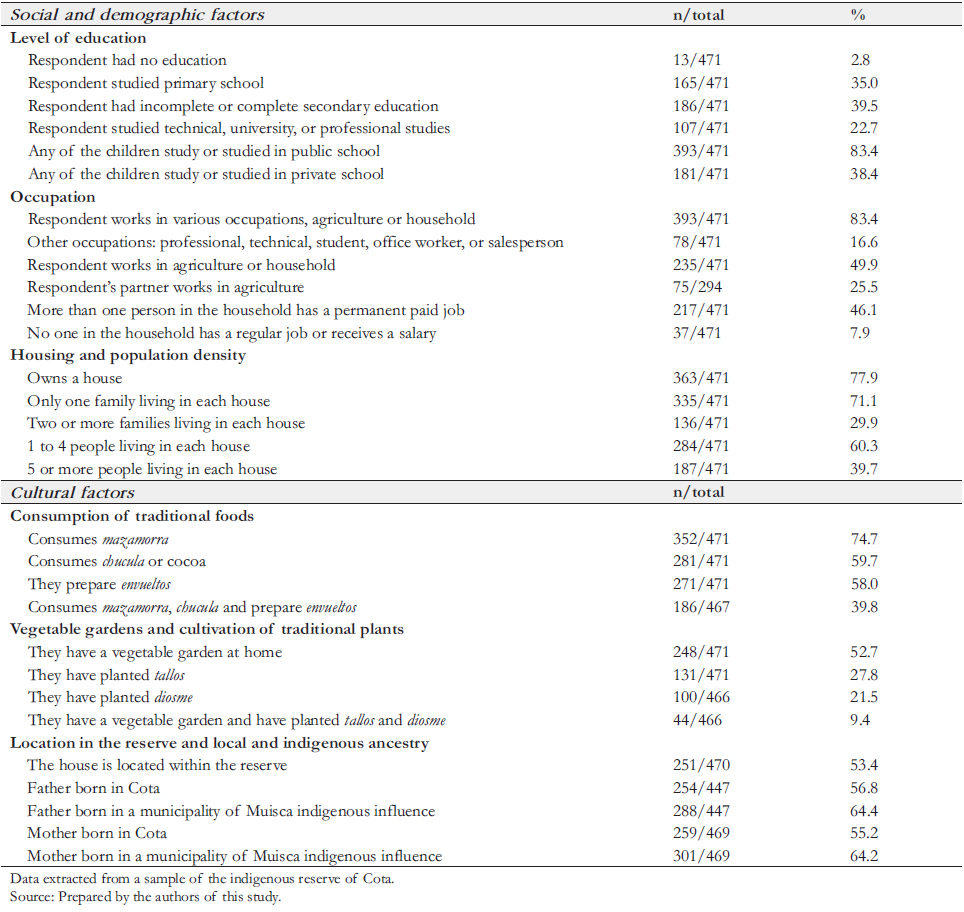
A total of 471 mothers of families belonging to the indigenous reserve of Cota who had at least one child older than ten years of age responded the survey. Of these, 47.6% (224/471) were younger than 47 years old, and 62.7% (295/471) of women were married or in a union, and 18.5% (87/471) never had a stable partner. Table 1 presents the frequencies of the demographic, social, and cultural factors explored in the study.
We found that 56.8% (267/470) have medicinal plants in their homes, regularly consume aromatic herbs, and use medicinal and wild plants for health care. Regarding traditional care, 15.8% (73/462) of families do not bathe during the flu, menstruation, or puerperium. Regarding the use of traditional medicine practitioners, 11.8% (54/458) reported that they had resorted to traditional midwives, sobanderos, and healers and considered that they are needed in the community. We also found that 66.2% (312/471) know at least three traditional diseases. Table 2 shows the reported frequency of traditional knowledge, resources, and practices.
Table 3 shows the main demographic, social, and cultural factors that we explored in the bivariate analyses with traditional medicine regarding resources, practices, practitioners, and knowledge outcomes. Five of them are present in two or more traditional medicine variables. These include consuming three traditional foods, having a vegetable garden, tallos, and diosme, having a father and mother born in a municipality of indigenous influence, and having a house within the reserve. Consuming the three traditional foods was the only variable present in all four outcomes.
Finally, in the multivariate analysis, we found four variables that maintained statistical significance (p < 0.05) in at least one or two of the traditional medicine outcomes, as shown in Table 4.
 Full size
Full size 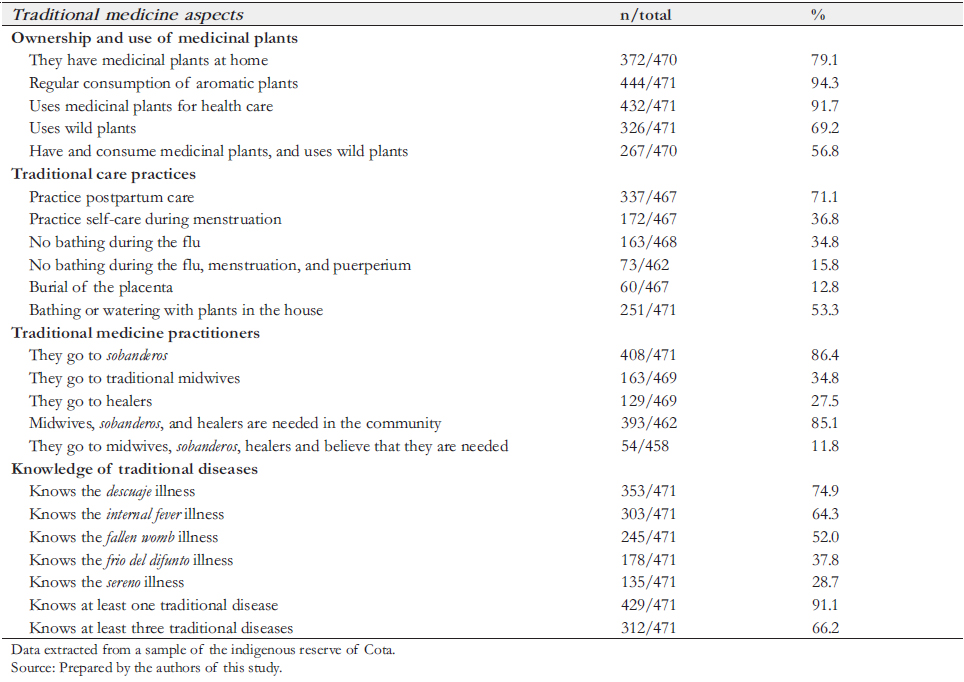 Full size
Full size 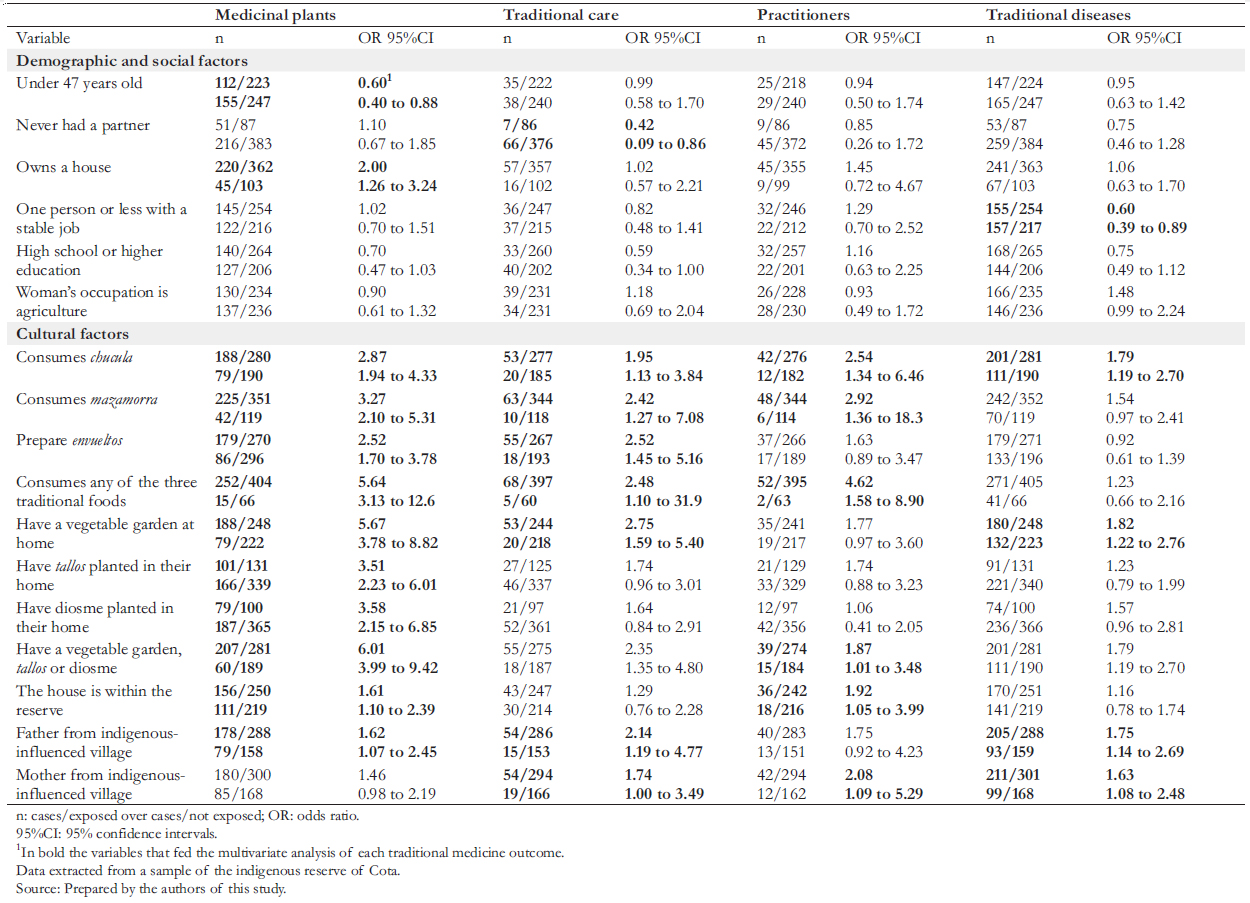 Full size
Full size 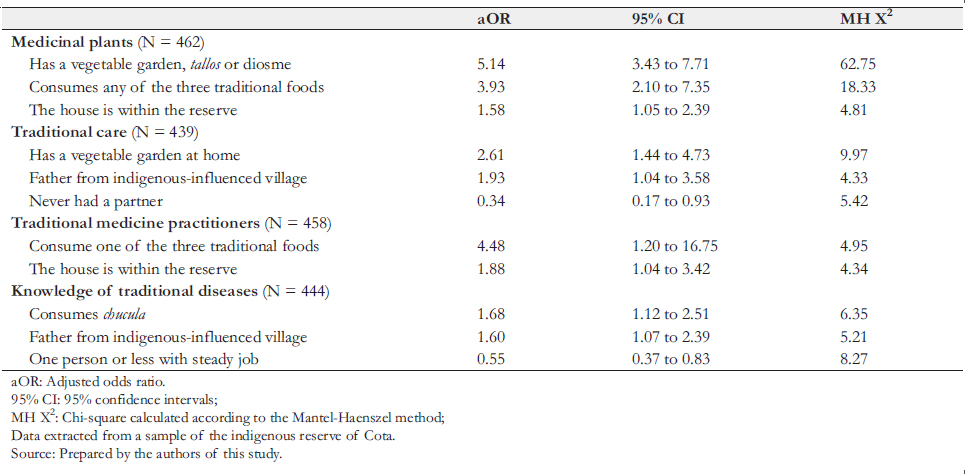 Full size
Full size Discussion
This study showed that traditional medicine persists in the indigenous reserve of Cota, despite its history of cultural loss, although with wide variability within its different expressions. Few studies have measured the prevalence of traditional medicine in Colombia. In 2002, the WHO estimated that 40% of the population in the country still used it [9]. However, these estimates should be taken with caution due to the complexity of traditional medicine definition and, as we have seen in this study, the variability of its expression.
We found that the consumption of three traditional foods, having gardens and traditional plants, having a home within the indigenous reserve, and having parents born in a municipality with indigenous influence, could be associated with traditional medicine in a sample of the indigenous reserve of Cota. These
indicators can guide additional actions in the Muisca community to promote and monitor the recovery of their traditional culture.
We also found that the possession and use of medicinal plants are still very high. A total of 91.7% stated they use them for health care and 79.1% had them planted in their homes. More than two-thirds of the sample had traditional care during the puerperium, which can be explained by the close company of mothers and grandmothers, allowing generational transmission of ancient knowledge. Half of the sample reported traditional flu or menstruation self-care, implying a loss of confidence in traditional customs, preferring Western medicine and pharmaceutical treatments.
Regarding the use of traditional medicine practitioners, we found a high prevalence of care by sobanderos. This phenomenon can be understood because there is a recognized sobandero within the community. On the other hand, the use of midwives barely reached 34.8%, possibly because the community currently recognizes no traditional midwives. Moreover, the use of healers was also low. The reserve currently recognizes an elder or sabedor (“el abuelo”), who also leads the ceremonies and rituals in the sacred house.
The degree of illiteracy among the respondents was very low, and almost 70% had primary or secondary education. More than one-fifth have attained higher education, which is higher than most indicators of Colombia’s indigenous population [18]. This finding can be explained by their proximity to the urbanized world and the long history of cultural mix and access to Western educational centers. We also found that despite their proximity to the urbanized world, and even though half of the families are outside the reserve, the indigenous population remains predominantly agricultural. Indeed, half of the women surveyed and more than two-thirds of their partners (from those who reported having them) were engaged in agriculture.
We found that slightly more than half of the respondents consumed traditional foods like chucula, mazamorra, and envueltos. Likewise, although slightly more than half also had gardens, less than a third had plants representative of the indigenous tradition, including tallos or diosme. The cultural loss is evident, although we could affirm that traditional food and vegetable gardens continue to be two of the most important cultural markers in the indigenous reserve of Cota.
Although it may not be possible to determine the degree of racial miscegenation of the Muisca people of Cota, our study found that slightly more than half of the respondents are still descendants of parents born in Cota or municipalities with Muisca indigenous influence. This data could be interpreted as unfavorable for indigenous peoples in general, who aspire to a low degree of racial miscegenation. However, even though the indigenous communities have been invisibilized for almost three centuries, there is currently a worldwide rise of indigenism. It is encouraging that communities such as the reserve of Cota want to return to a true indigenous identity [19].
Education level, occupation, housing, and population density were not associated with traditional medicine in the surveyed group. These data may be contradictory compared to other traditional communities worldwide. In these works, Western education, work activities of the modern world, and lifestyle closer to the Western development model are often factors associated with the loss and abandonment of traditional medicine [20]. Their impact may have already produced a dramatic loss in their traditional medicine over the years. However, at this stage of their history and their eagerness to recover their indigenous identity, new sociological and generational transmission elements emerge to achieve an effective form of resilience in the face of the acculturative effect of the Western education and development model [21].
Weaknesses and stRengths of thIs study
In 2002 the WHO warned that there is a need for innovation in research methods on traditional medicine [12]. Our exploratory study can provide some reflections in this regard. Given that indigenous traditional medicine is still poorly understood, this study explores general variables as proxy measures. Community participation was essential to define these variables and should be included in other studies addressing similar topics. The limitations inherent to cross-sectional studies restrict causal inference. Therefore, it is hard to know to what extent variables associated with the occurrence of traditional medicine may or may not contribute to its recovery.
In a context of scarce funding for research with indigenous groups and limited resources in these communities, exploring non-probability sampling is a feasible alternative to begin. In this study, we included women who possibly have a preponderant role in using traditional medicine and can give more accurate information on this subject. However, the counterpoint of mainly including women is the difficulty of extrapolating the results to the whole reserve or other indigenous populations. Achieving more accurate results will require interdisciplinary consideration of the population characteristics and their relationship to the included sample [22]. Discussion of the results with the communities may also help in this regard.
conclusions
This study showed that traditional medicine in the Muisca reserve of Cota might be associated with traditional food, agricultural vocation, and possession and use of traditional plants.
The findings suggest that the strategy for the recovery of traditional medicine could focus on promoting a grater link between indigenous identity, territory, food, and health.
Notes
Contributor roles
GZ: led the research, from design to writing the final results. CC: participated in the design, was responsible for data collection, and contributed to writing the results. NAR: participated in the design and data collection and contributed to writing the results. SPC: participated in the design and execution, coordinated data collection with the community, and reviewed the writing of the results. IS: Participated in the design, led the data analysis, and contributed to writing the results.
Acknowledgments
The authorities and members of the indigenous reserve of Cota promoted the study, participated in all stages and authorized the publication of this article. The Center for Intercultural Medical Studies (CEMI) also collaborated in all stages of the study. The Department of Family Medicine and Public Health of the Faculty of Medicine of the Universidad de La Sabana collaborated with the participation of XI Semester of Medicine students in the stages of data collection and analysis.
Competing interests
The authors completed the ICMJE competing interest statement and declared that they did not receive funds for this article; they have no financial relationships with organizations that may have an interest in an article published in the last three years, and they have no other relationships or activities that may influence the publication of the article. Forms can be requested by contacting the responsible author or the Editorial Board of the journal.
Funding
The project was financed by the Health Secretary of Cota (Cundinamarca), Colombia.
Ethics
CEMI arranged the study with the authorities of the indigenous reserve, and a community agreement was signed for research and information-sharing agreement. Individual informed consent was requested from the participants, guaranteeing anonymity and confidentiality. The study followed the participatory research model that sought to involve the communities throughout knowledge generation. Although this project involved human participants, it is considered that the instrument does not contain sensitive information, so it falls into the category of research with minimal risk, according to Resolution No. 8430.
Data sharing statement
The data used for the present study are available in the following open repository: https://figshare.com/s/ f8424431d26e8b2c71f6
Language of submission
Spanish.
