Estudios originales
← vista completaPublicado el 15 de julio de 2022 | http://doi.org/10.5867/medwave.2022.06.002555
Sistematización de iniciativas en salud sexual y reproductiva según criterios de buenas prácticas en repuesta a la pandemia COVID-19 en la atención primaria en Chile
Systematization of initiatives in sexual and reproductive health about good practices criteria in response to the COVID-19 pandemic in primary health care in Chile
Abstract
Introduction The COVID- 19 pandemic discontinued sexual and reproductive health care in Chile and the world. The national focus on hospital care led primary care teams to respond in natural and diverse ways. Understanding the factors involved in this process may improve future responses from the judgment of good practices. Therefore, this study aimed to identify and systematize sexual and reproductive health initiatives raised by primary care teams in response to the COVID- 19 pandemic in Chile.
Methods We systematically evaluated initiatives and practices in sexual and reproductive health in prima-ry care between June 2020 and November 2021. This study was developed in three methodological phases: a review of documents, a collection of experiences through an electronic instrument sent to the 29 health services in Chile, and in-depth interviews. According to best practice criteria, mapping and characterizing the initiatives and critical discourse analysis of narratives and interviews were carried out.
Results Forty-one initiatives from 19 health services were identified, mainly from the South Central macro zone and urban areas. In these areas, care was recognized. These practices were relevant, aligned with their objectives, rapidly implemented, and used novel strategies through new technologies. However, these initiatives had little intercultural relevance or evaluation. Perceived success was related to motivation, leadership, and institutional and community resilience. The adaptability of initiatives emerged as a new need and criterion of analysis.
Conclusion The lessons learned from these initiatives invite us to consider health care teams' mental health, their relationship with the community, the use of new technologies, the evaluation of practices considering satisfaction, cross- cutting approaches, and their adaptability. In all, these aspects may improve primary care response in sexual and reproductive health to new crises.
|
Main messages
|
Introduction
At the beginning of the COVID- 19 pandemic, it was foreseen that the population’s health would be severely affected, especially in groups with biological and social vulnerabilities [1].
In Chile, epidemiological studies assessed the health policies adopted for the initial management of the pandemic and the challenges faced by the system. These studies warned the need for constant evaluation and intersectoral participation to respond to the crisis [2],[3],[4].
The high demand for COVID- 19 care led the Chilean health system to focus mainly on hospital care, which was administratively and economically dependent on the central level, prioritizing the growing need for critical beds. Thus, the overuse of physical, human, and economic resources for COVID- 19 care led to decreased availability of regular inpatient and outpatient services [5].
Although there were general recommendations from the central level since March 2020 [6], primary care – whose administration depends on the municipalities – had to reorganize, prioritize and self- manage its functions. Amidst crisis, primary care faced structural challenges that positioned local teams as guarantors of continuity of care.
Sexual and reproductive health services were one of the most affected services. For this matter, specific guidelines appeared four months after the pandemic started. These services' avail-ability, utilization, and coverage were affected, impacting the quantity and quality of sexual and reproductive health care [7],[8].
According to a survey of civil society in Chile regarding sexual and reproductive health care in 2020, 44% of people reported access difficulties, most of which were women [9]. Likewise, according to the Ministry of Health, sexual and reproductive health services in primary care decreased by 47% in 2020. In this scenario, pregnancy, postnatal and fertility care were prioritized, but preconception care, gynecological screening, and climacteric care decreased its accessibility. Despite efforts, pre-natal care admission activities decreased by 13% between 2019 and 2020, with a concomitant 2% increase in late prenatal admission [10].
Any detriment in availability and access to sexual and reproductive health services generates gender, equity, and rights issues – especially in women, girls, and adolescents [11],[12],[13] –, directly and indirectly impacting their health and wellbeing [14].
In line with the above, it has been shown that recovering universal access to sexual and reproductive health services is one of the main objectives that societies should aim at to reverse the population’s health drawbacks during the pandemic [15].
To achieve these objectives, we need to learn from the sexual and reproductive health teams in primary care and see where health promotion and prevention foundations are laid today, which was strongly threatened by prioritizing care associated with COVID- 19 [16].
Arranging how health teams initially responded to the pan-demic and what processes they developed based on good practice criteria [17] is essential to identify challenges, strengths, gaps, and lessons learned in these years. In all, this process con-tributes to avoiding new interruptions of services and violations of sexual and reproductive rights [18],[19]. Therefore, this study aims to identify and systematize initiatives proposed by primary care teams in sexual and reproductive health based on good practice criteria in response to Chile’s COVID- 19 pan-demic between June 2020 and November 2021.
Methods
We arranged initiatives developed by sexual and reproductive health teams in primary care in response to the COVID- 19 pan-demic between June 2020 and November 2021. This study was part of a project named "Identification and systematization of good practices and lessons learned in sexual and reproductive health in response to the COVID- 19 pandemic in Chile and Latin America" from the Department of promotion of women’s and newborn health of the Universidad de Chile.
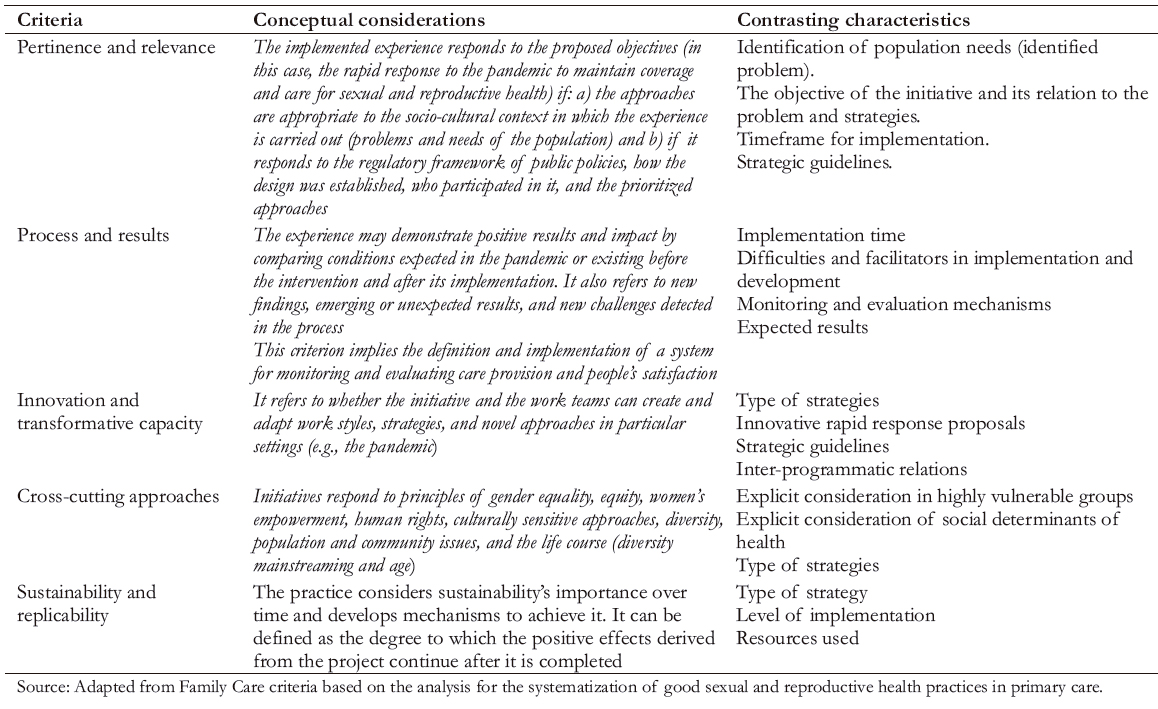
The study was carried out in three methodological phases [20]. First, a review of documents on good health practices was carried out [17],[18],[21],[22] to select and arrange analysis criteria. These included relevance and pertinence, process and results, innovation and transforming capacity, cross- cutting approaches [23], and replicability and sustainability of good practices, as described in Table 1 [17].
In a second phase, a tool was developed to collect initiatives that included mapping variables, including distribution according to rural and urban areas and macro geographic zones of Chile with climatic and population density differences. These macro zones, apart from the Metropolitan Region, divide the country into Northern (desert and low population density), Central and Central South (tempered climate and high population density), South (rainy and medium population density, and Austral (cold climate and low population density) regions [24]. We also included other variables such as the establishment type and implementation time, the month of initiation, and the speed of implementation according to the number of weeks needed for the initiative (less than four, between four and eight, or more than eight weeks). In addition, the guidelines, strategies used, areas of sexual and reproductive health considered, and open- ended questions aimed at sharing the experience were recorded.
The survey was validated for relevance and comprehension by ten expert professionals from different services and levels of care [25]. It was shared from the Ministry of Health through an electronic form to the 29 services of the Chilean National Health System between June and December 2020, obtaining 41 responses. Any health professional could report as an individual, team, or institution implementing an initiative or new practice in response to the pandemic.
To further analyze initiatives development after one year, in the third phase between October and November 2021, all those who reported initiatives in the survey were invited to be inter-viewed. Finally, 15 were interviewed, corresponding to all who voluntarily responded to the invitation.
Each interview was recorded, transcribed, and organized within the framework of the instrument in a systematization matrix. Systematization was understood as "the critical analysis of experiences that, from their ordering, reconstruction and expression of their actors, discovers or explains the logic of the process, the factors that intervened, how they related to each other and why they did it that way" based on previously defined criteria [26]. In this case, according to good practice criteria.
Critical analysis was based on the theory of interpretative structuralism focused on discourse and social setting, considering each experience as a study case [27]. From a reflective and constructive approach from the setting and factors configuring the initiatives [28], units and categories were identified and presented in domains as criteria of good practices. These considerations and contrasting characteristics are presented in Table 1.
 Full size
Full size Ethics
The study was approved by the Human Research Ethics Committee of the Faculty of Medicine of the Universidad de Chile, N°085- 2020. Informed consent was requested in the second phase and ratified in the third phase by the informants.
Results
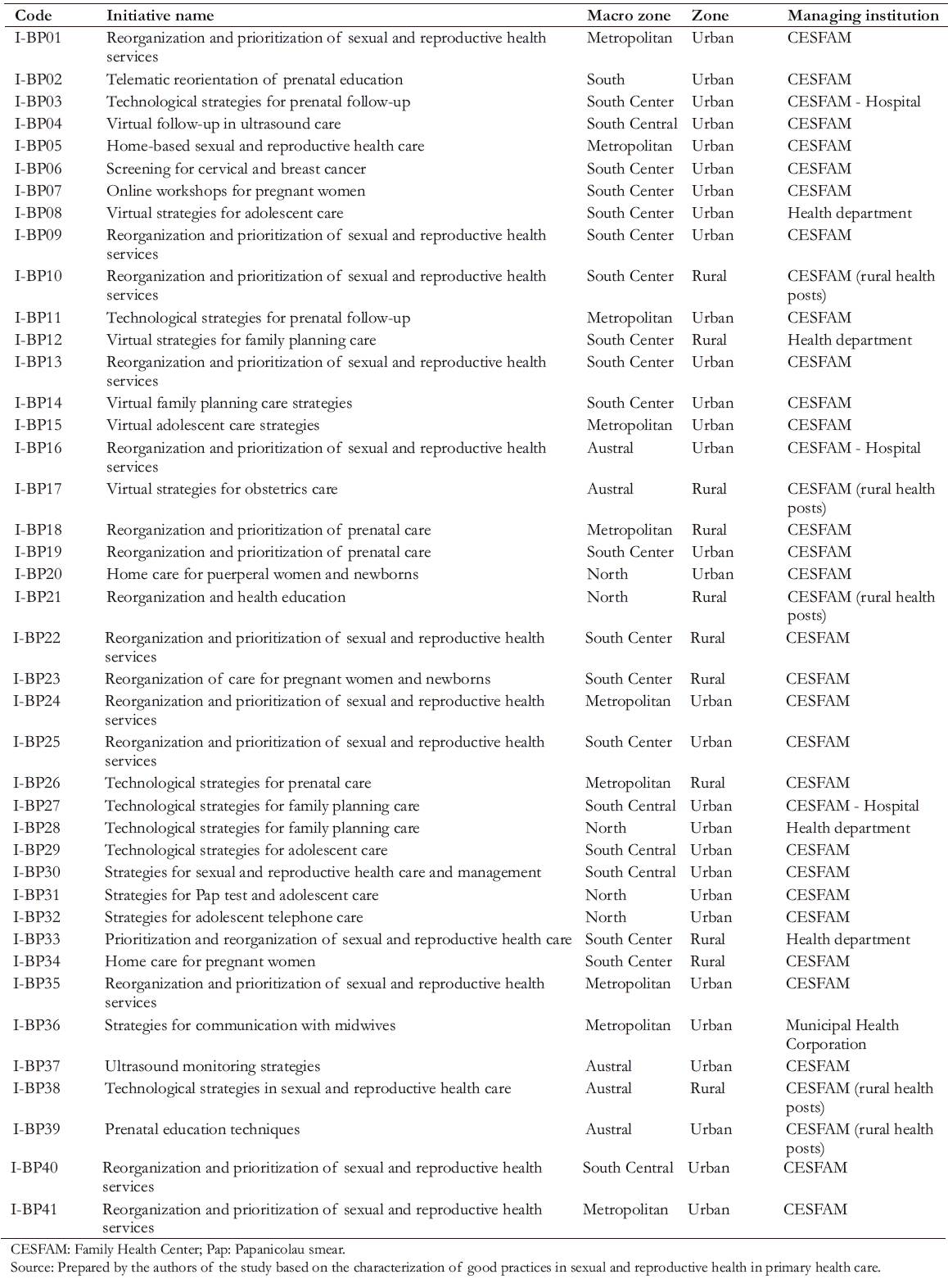
Forty- one initiatives from 34 family health centers, five municipal corporations, and three hospitals related to primary care were identified (Table 2). These came from 19 of Chile’s 29 health services.
Of the total initiatives, 30 (73%) were carried out in urban areas and 11 in rural areas (27%). Moreover, 46.3% were from South Central (19), 24.4% from Metropolitan (10), 2.4% from South (1), 12.2% from North (5), and 12.2% from Austral Macro Zones (5).
Regarding implementation time, 73% (30) of the initiatives started between [3] the same proportion was implemented in less than four weeks. Regarding the strategics, 70% (29) made changes in care activities, 90% (37) considered the reorganization of services, and 39% (16) made programmatic changes. The main types of strategies are shown in Figure1, where it can be seen that most of the initiatives included communication and technological changes.
Maternal health accounted for 39% of the main areas of sexual and reproductive health addressed, followed by family planning (29.3%). Gynecology was only recorded in two initiatives.
Table3 shows quotes from stories extracted from the analysis of the initiatives according to good practice criteria.
The following are the results of the systematization and analysis of the initiatives according to the criteria of good practices.
Pertinence and relevance
In the absence of central recommendations at the beginning of the pandemic, the initiatives came from the motivation of the teams to respond to an emerging health situation that generated problems in promoting, preventing, and continuing care for sexual and reproductive health (Table4). The following categories stand out from this process.
Social relevance and territoriality
A high social relevance was observed in the initiatives, reflected in the innate capacity of the primary health care teams to detect and respond to the needs of women, pregnant women, and adolescents. These teams generated limited and prioritized strategies according to the needs and context.
Thus, a territorial approach stood out since the strategies were related to the geographic area and urban or rural settings. For example, home visits were chosen to avoid discontinuity in southern and rural areas, and telecommunication was chosen in urban areas. This reflects cultural aspects possibly related to the territory.
Importance of the team-community relationship
An excellent institutional registration system and knowledge and communication with the population were considered facilitators for identifying needs and planning strategies.
Moreover, the magnitude and scope of initiatives depended on the need, the level of action, and management. Thus, when initiatives came from leaders respected by the community and the team, they covered larger areas and even involved more than one care program. On the contrary, when they were raised from needs perceived by a single professional, they had less development and scope.
Although the implementation process was fast in most cases (less than four weeks), the evolution was complex, and the following difficulties and facilitators were identified.
 Full size
Full size 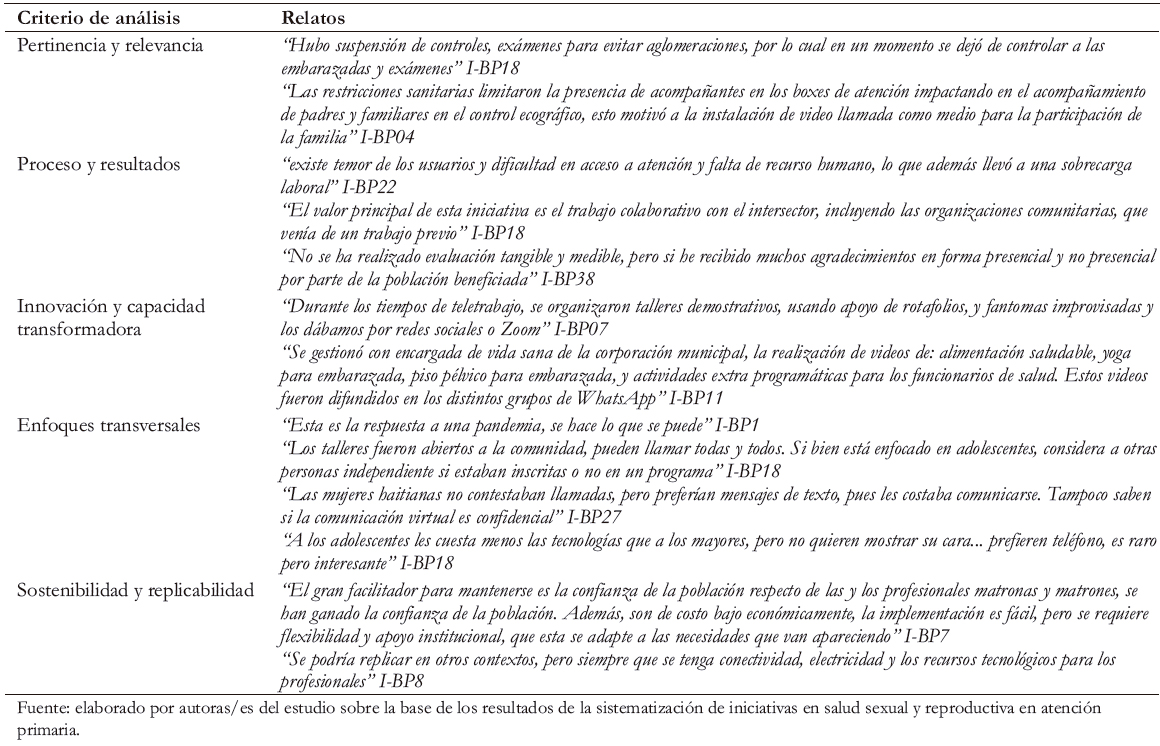 Full size
Full size 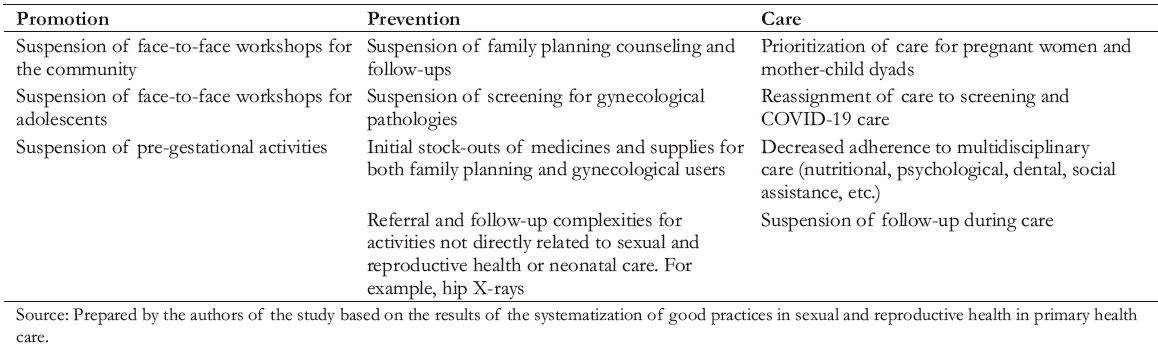 Full size
Full size 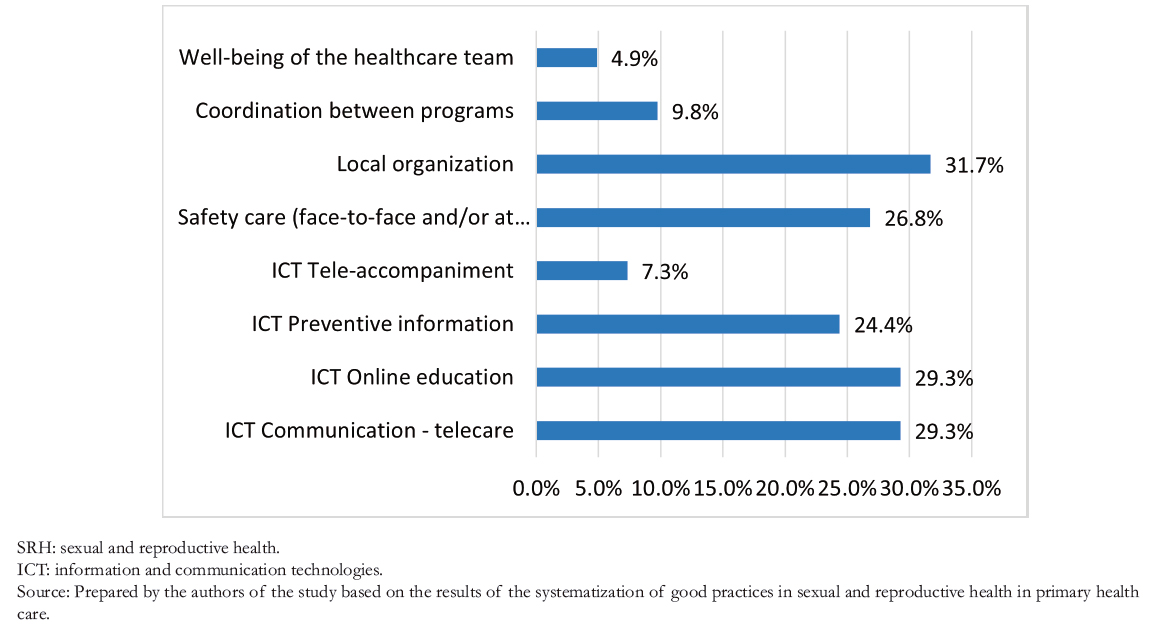 Full size
Full size Process and results
Difficulties
Changes in conditions and ways of providing care
The main difficulties came from the need to reorganize human resources for new activities for which the equipment and infra-structure were not prepared. These difficulties involved changing workplaces, remote work, and performing untraditional functions. In some experiences, it was reported that the closure of the medical- statistical orientation units implied reorganizing the strategies for informing the community, assigning hours, and managing agendas. These difficulties were exacerbated by the bureaucracy of administrative systems and the impossibility of adapting to new settings, especially with complex management mechanisms.
Demand for new competencies
The initial fears of the personnel associated with using new technologies are noteworthy. However, the in- depth interviews showed that acquiring "new digital competencies" was finally seen as a learning opportunity.
The need for training and new technological resources, as well as the deepening of ethical confidentiality aspects in remote care settings, emerged as new challenges for the teams and the system.
Workload and work evaluation
The physical and mental exhaustion of teams and work over-load related to the difficulty of replacing human resources due to illness or remote work was a limiting factor. The same happened with the absence of initial boundaries in the communication between professionals and users when the personal phone was used to provide information. The initiatives were more likely to develop when these factors were addressed. Effective communication with managers influences the perception of the outcome.
Lack of knowledge and uncertainty in a new healthcare setting
The lack of new care strategies and communication problems made the initiatives more complex. In the face- to- face activities, the uncertainty of the health setting and the non- guaranteed availability of personal protection elements for both workers and users generated great stress and additional responsibility for the health team.
Facilitators
Leadership, teamwork, and organizational idiosyncrasies
Teamwork was the most frequently mentioned unit of meaning. Likewise, positive and motivating leadership emerged as an incentive for initiatives, contrary to individual practices that were only maintained in the first months of the pandemic.
The teams developed the initiatives better with a pleasant work environment, defined roles, and organized functioning. In these cases, the discourse reflected an anticipatory and empathic capacity that translated into confidence in the capacities of resilient teams committed to all health areas beyond the expected outcome. This showed a positive organizational idiosyncrasy – i.e., the natural, cultural, and appropriate way of acting in an organization and moving towards a joint achievement.
Intersectoral relationship and appreciation of municipal authorities
Working with other sectors such as education and municipal management was mentioned in the discourse of self- declared successful practices. The intersectoral relationship was a positive strategy, and such work should be promoted with and with-out crisis. Likewise, the spread of information promoted by municipal authorities and the allocation of local resources to primary health care management – particularly in sexual and reproductive health – were crucial factors in achieving expected short- and medium- term results.
Women’s empowerment and community
Communities perceived as organized and empowered with a history of health education reacted and adhered positively to new measures. This reflects the importance of a previous con-nection of the primary health care teams to generate autonomy and obtain an adequate adherence to the strategies in crisis. These communities knew what to do and how to react while care was being readjusted.
On the other hand, the results and impact of the initiatives did not contemplate follow- up or formal evaluation mechanisms, much less qualitative or satisfaction evaluations. However, in initiatives of follow- up of women and home visits, informants perceived satisfaction and had a direct expression of gratitude by the users.
Innovation and transformational capacity
This criterion acquired great relevance since it tested the capacity of teams to adapt to change and find new ways of maintaining coverage and continuity of care.
Although some initiatives only prioritized reproductive health care, others demonstrated a great capacity to innovate through management strategies and new technologies to organize, pro-gram, and execute care in an integrated and comprehensive manner. The following categories emerged from this process.
Innovating for a positive experience in crisis settings
From the discourse analysis, we identified teams' ability to con-sider the comprehensiveness and quality of health from providing care and people’s experience. Strategies aimed at maintaining a positive experience for women despite the restrictions of attending face- to- face services stand out. This encouraged sup-port during care, either in person or remotely, even in some cases using their own technological devices. In turn, users and workers' relaxation and stress reduction techniques reflected empathy and innovation and were perceived as "very comforting" by the informants.
The pandemic as an opportunity to innovate in education and integrated care
New technologies permitted democratizing access to knowledge through online community workshops on various sexual and reproductive health topics through social networks. In this way, a dialogue of knowledge was favored. Additionally, these new technologies managed and provided organized and coordinated care among the programs, which permitted multiple interventions. For example, some initiatives brought together different disciplines to address not only issues of sexuality and reproduction but also lifestyles and mental health, regardless of the health program in which it was conceived.
Cross-cutting approaches
The need to prioritize services and the urgency of their implementation subjugated the incorporation of new approaches to new realities. In this area, the interventions that made up the following categories stood out.
The principle of leaving no one behind and the challenges of gender, diversity, inclusion, and life course
The rights- based approach and initiatives that revealed new needs and ethical considerations in the communication through technological strategies stood out in the open initiatives to the community.
Although the quantitative data reflected a prioritization of reproductive health initiatives, some experiences targeted specific groups (such as people infected with COVID- 19), avoiding discontinuity of access to family planning through scheduling of care and home visits.
Moreover, initiatives lacked approaches toward gender violence, sexually transmitted infections, and HIV, which were only emerging issues.
Regarding the life course, strategies aimed at people in non- reproductive contexts, such as breast and cervical cancer screening, were less considered. These strategies increased again as the program returned to face- to- face attendance. However, additional human resources did not support this increase in strategies and negatively affected promotion initiatives implemented during the pandemic.
Information and communication technologies and democratic access to health care
The increased use of technologies was paradoxical. Although it maintained the coverage of certain benefits and promotion and prevention strategies, it revealed new gaps associated with equitable access to digital resources and competencies. The gaps were associated with sociodemographics such as age, territory, and economic resources. Access to technologies transcends digital competencies and stresses new challenges beyond the health sector.
The debt of interculturalism and crises
Although the pandemic has developed parallel to a migratory crisis in Chile, mainly in the North of the country, interculturalism was scarcely considered in new strategies. Furthermore, problems were revealed, such as the cessation of intercultural mediator programs and the worsening of language barriers, mainly among Haitian women who did not speak Spanish. This pandemic may have aggravated access to the population with previous problems of this nature.
Sustainability and replicability
According to the discourse, the sustainability of the initiatives depends on the needs, the resources allocated, and the organizational vision to maintain them. The following categories emerged.
Responses not to the system but to health emergencies
The analysis shows that the initiatives were designed to rapidly respond to a health emergency and not necessarily improve the quality of care. This result raises the question of which initiatives are sustainable over time. Thus, some care reorganization practices were considered to return to previous normality. In contrast, initiatives aimed at "continuous professional support" through new technologies, information management, organization practices, and inter- program coordination strategies were considered potentially sustainable because they are efficient and facilitating in any setting. However, the return to "normal care" was parallel to the recovery of activities postponed during the first year of the pandemic. Together with the disengagement of human resources, these aspects challenged the continuity of innovative and sustainable initiatives.
Adaptability as a potential criterion for analyzing initiatives in crisis
The need for "adaptability" of health emergency response practices emerged in the discourse. The evolution of the crisis demanded a constant rethinking of strategies, thus straining the bureaucratic processes that compromised their management. This questions administrative flexibility that transcends the organization of the health system.
Replicability depending on the setting
Most of the initiatives were replicable in similar health crises and new outbreaks, mainly those in which technological resources can be used. However, other health emergencies (e.g., natural disasters) require adaptation to the setting and circumstantial aspects that compromise sexual and reproductive health care.
Discussion
The response initiatives of sexual and reproductive health teams in primary health care were investigated through systematization. This study glimpsed exemplary practices in primary health care in the face of new crises.
Analyzing the pertinence and relevance and the process and results of the initiatives highlights the importance of knowing the community. This may be achieved through constant dialogues and an adequate registration system to identify needs and evaluate the processes. These results are consistent with international recommendations that show the need to invest in monitoring systems to prioritize and improve the health of women and girls [29],[30].
Although there are quantitative recording systems in primary health care in Chile, the absence of this tool in the initiatives evaluated in this study promotes improvement plans and satisfaction assessment to enhance practices based on quality care. This assessment should consider data that evaluate care provision and people’s experiences [31],[32].
Positive leadership and motivation showed great relevance in the emerging initiatives when analyzing the processes, innovation, and transforming capacity criteria. These results also relate to organizational competencies of adaptation to change and cultural and organizational resilience necessary to face crisis contexts [33],[34],[35]. Such resilience possibly triggered locally managed capacity to innovate and transform their practices in response to the emerging needs of the population. However, as revealed by the discourse and evidence, professionals' health and working conditions need improvement since the high workload and exhaustion in complex scenarios can jeopardize the human response capacity and the quality of care [36].
The extensive use of technologies generated fundamental challenges to the democratization of universal access to emergency care and good practices in their use [37],[38], as well as digital literacy in teams and users [39]. In turn, we should consider future reflections on the relevance of telehealth versus face- to- face care and its impact on women’s health to determine whether it is sustainable in multiple scenarios [37].
The results of this study also reflect the need to systematically incorporate cross- cutting approaches to gender, inclusion, interculturalism, and life course in response to health crises. The absence of this approach exacerbates crises, mainly among women and populations with greater sexual and reproductive rights violations, such as the LGTBIQ+ community, people living with HIV, and migrant women and girls [11],[40].
On the other hand, given that care was deprioritized during the pandemic, it is urgent to maintain promotion and prevention practices parallel to this recovery. Thus, the lessons learned from the initiatives invite us to discuss the challenges for the system and teams to continue traditional care simultaneously with the recovery without considering human resources as a basis. This aspect is fundamental since the pandemic highly impacted health workers' physical and mental health [40]. According to the literature, the pandemic particularly impacted female workers, exacerbating gender inequalities [41].
New challenges and criteria emerged in the pandemic, mainly for organizational initiatives, such as the need for administrative "adaptability" [42]. This criterion would account for the flexibility of management systems in crisis dynamics to facilitate rapid responses to emerging sexual and reproductive health needs in complex settings. This adaptability facilitates the achievement of the objectives and their transformation into good sexual and reproductive health practices.
Conclusions
The initiatives and practices presented by sexual and reproductive health teams in primary health care showed positive leader-ship. Moreover, we found that most teams anticipated the recommendations from the central level.
Through the systematization of initiatives, we learned the importance of the relationship between the teams and the com-munity, the recording of community needs, and the importance assigned by decision- makers and the organizational idiosyncrasy.
We also identified the need to consider the workers' physical and mental health and maintain follow- up and monitoring systems for the initiatives, considering cross- cutting approaches to improve satisfaction and the positive impact on health in future crises.
Through the discourse, we also found that the pandemic encouraged the use of technologies to promote inter- programmatic and inter- sectoral work and the new challenges in democratizing access to these technologies.
Finally, it was considered that more than being sustainable and replicable, crisis response initiatives should be adaptable to facilitate their management in crises that become chronic and dynamic, such as pandemics.
