Estudios originales
← vista completaPublicado el 22 de julio de 2022 | http://doi.org/10.5867/medwave.2022.06.002567
Caracterización clínica, psicológica y sociofamiliar de la conducta suicida en adolescentes chilenos: análisis de correspondencias múltiples
Clinical, psychological, social, and family characterization of suicidal behavior in Chilean adolescents: a multiple correspondence analysis
Abstract
Introduction Suicide is the second leading cause of premature death in people between 15 and 29 years old and the third in young people between 15 and 19 years old. Adolescence is a critical period concerning mental health disorders since there is greater vulnerability to suicidal behaviors. The situation in Latin America is worrying, with Chile being one of the two countries where suicide rates of children and adolescents increase yearly. This study aims to analyze clinical, psychological, family, and social risk factors associated with suicidal behavior in a clinical sample of adolescents treated in the public health system of the Maule region.
Methods The study design is cross- sectional. We used a sample of 388 adolescents between 10 and 21 years old admitted to the health system of the Maule Region. The participants were evaluated by applying five measuring instruments (The Barrat Impulsivity Scale, The Difficulties in Emotional Regulation Scale, The Depression, Anxiety and Stress Scale, The General Help-Seeking Questionnaire for mental health problems in adolescents, and The Columbia Suicide Severity Rating Scale) in addition to collecting social and family information and relevant clinical history from the medical records.
Results The analysis allowed us to identify distinctive characteristics of adolescent suicidal behavior by describing clinical, psychological, and family social factors.
Conclusions Adolescents with a history of suicide attempts are characterized by having suicidal ideation, anxious-depressive symptoms, stress, insomnia, and impulsiveness. Likewise, they report being non-religious, belonging to sexual minorities, and victims of sexual harassment and/or abuse.
Introduction
Adolescence transitions between childhood and adulthood and involves elements of biological growth and transition to social roles, which have changed significantly at the end of the last century [1]. Earlier puberty and delayed completion of education, marriage, and parenthood have extended adolescence to an age range of 10 to 24 years [2].
Suicide is one of adolescents' leading causes of death [3]. Between 10 and 24 years, more deaths occur from suicide than traffic accidents, cancer, and heart disease [4]. As in adults, there is a gender paradox in this age group; males commit suicide more than females, and females attempt suicide more than males [4],[5]. However, the suicide rate among adolescent males and females has been leveling over the past decade [6].
Despite efforts to prevent suicide in this age group, the suicide rate has not decreased [7]. Adolescent suicide deaths in Chile increased by 55% between 1999 and 2005, and Chile is the second country of the Organization for Economic Cooperation and Development (OECD) with the highest percentage variation [8]. A recent study compared the suicide rate of adolescents aged 10 and 19 years among OECD member countries. In this study, Chile had the fourth- highest rate with 5.36 deaths per 100 thousand inhabitants, and by subgroups, the highest rates between 10 and 14 years in men and women with 2.23 and 1.56 deaths per 100 thousand inhabitants, respectively. Meanwhile, for the 15 to 19 years age group, it ranked third in males and fourth in females with 15.87 and 6.32 deaths per 100 thousand inhabitants [9].
To understand suicide, we need to analyze interrelated behaviors that constitute a "continuum" in which biological, social, psychological, and clinical factors intervene. These factors interrelate and clinically manifest as suicidal behavior [10],[11].
Suicidal behavior is understood by psychology as a process that begins with the "death wish" – a stage in which thoughts down-grade one’s existence and question the very act of living, in addition to dissatisfaction with daily life. Subsequently, "suicidal ideation" – a phase in which ideas of ending one’s life arise – may occur with or without planning, although its presence indicates a more serious clinical condition. This process may culminate in a "suicide attempt", dramatically increasing the likelihood that the individual will take his or her own life [12],[13],[14].
Suicide ideation and attempts are most prevalent during adolescence [15]. In turn, the probability of making a suicide attempt in adolescents increases 12- fold when combined with suicidal thoughts [5]. Likewise, rates of self- injury are also high in adolescents with an early- onset at 12 years of age, mainly in females, reaching 20% at 15 years of age [16]. There is evidence of significant associations between self- injury and suicidal thoughts and attempts [16],[17].
On the other hand, suicidal behaviors show irregular and fluctuating patterns in adolescence. Some adolescents plan to take their own life but never make a suicide attempt, while others attempt without planning. Some make a single attempt, while others make repeated attempts, and there are also those who – despite their vulnerability – never develop these behaviors [5],[10]. It is estimated that for every completed suicide in young people, there are between 100 and 200 attempts [18]. In addition, suicidal thoughts have been associated with subsequent attempts and repetition [15], which is one of the main predictors of suicide in adolescents [19]. It is estimated that about one- third of adolescents with suicidal thoughts will attempt suicide during the next 12 months [5].
Studying only adolescents who have attempted suicide restricts access to valuable evidence of suicide risk in this age group, given that more than three- quarters of adolescent suicides occur in the first suicide attempt [20]. Therefore, the present study aims to characterize the clinical, psychological, social, and family risk factors associated with suicidal behavior in a broad clinical sample of adolescents in the Maule region’s public health system.
Methods
Design
An observational, cross-sectional design was used for this study.
Participants
The sample included adolescents of both sexes between 10 and 21 years of age who were admitted between March 1 and August 31, 2018, to different primary and secondary care mental health programs in the Maule Region, Chile. Participants were selected by non- probabilistic sampling [21]. Illiterates, adolescents who refused to participate or whose mother, father, or legal guardian refused consent, and adolescents with active psychotic symptomatology were excluded from the study. The analyzed data are part of the Fondecyt project No. 11170342 entitled “Trayectorias de ideación e intentos de suicidio en adolescentes con trastornos psiquiátricos de la región del Maule”.
Instruments
The Barrat Impulsivity Scale (BIS- 11) assesses impulsivity through 30 items grouped into three subscales: cognitive (eight items), motor (10 items), and unplanned impulsivity (12 items). Each item has a four- point Likert scale (1: rarely or never, 2: occasionally, 3: often, 4: always or almost always). This scale has been validated in the Chilean adolescent population and has a moderate internal consistency with a Cronbach’s α of 0.77 [22].
The Difficulties in Emotion Regulation Scale (DERS) is an instrument that measures clinically relevant difficulties in emotional regulation and includes five subscales: emotional dyscontrol (six items), emotional rejection (seven items), emotional interference (four items), emotional inattention (five items) and emotional confusion (three items). It is answered on a six- point Likert scale (1: I strongly disagree, 2: I disagree, 3: I somewhat disagree, 4: I somewhat agree, 5: I agree, 6: I strongly agree). The scale was validated in Chile in a university population with high internal consistency, Cronbach’s α of 0.92 [23].
The Depression, Anxiety and Stress Scale (DASS- 21) is com-posed of 21 items, measuring depressive (seven items), anxiety (seven items), and stress symptoms (seven items). Each statement has a four- point Likert scale that describes how the per-son felt during the last week (0: never, 1: sometimes, 2: often, 3: always). This scale was validated in the Chilean population presenting a high internal consistency with a Cronbach’s α of 0.91 [24].
The General Help- Seeking Questionnaire for mental health problems in adolescents (GHSQ- V) consists of 11 items describing perceived barriers to seeking professional help. Each item is evaluated on a six- point Likert scale (1: I strongly dis-agree to 6: I strongly agree). A higher score indicates more perceived barriers to help- seeking. This scale is validated in Chile in the adolescent population and showed moderate internal consistency with a Cronbach’s α of 0.76 [25].
The Columbia Suicide Severity Rating Scale (C- SSRS Chile/Spanish 5.1) was designed to collect information about suicidal ideation, suicidal behavior, and non- suicidal self- injury. It quantifies the severity of suicidal ideation and behavior during specific periods. This instrument has a mixed format, with open- ended, closed- ended, and Likert- type questions. It has presented acceptable predictive results for future suicidal attempts in clinical and adolescent populations [26],[27].
In addition to the instruments already described, a sociodemographic questionnaire was used to access information regarding sex, sexual orientation, religious beliefs, and family structure characteristics. Moreover, medical records were assessed for information that included previous attempts, hospitalizations, and treatments. Finally, the participants' clinical records were reviewed to collect information about school bullying and domestic violence.
Procedure
The study proposal was distributed among mental health teams of hospitals, community mental health centers (COSAM), and family health centers (CESFAM) of the Maule region, Chile. Subsequently, we performed a census of the patients who had visited the mental health units in the last six months. Then, a research team member invited patients to participate and informed them about the essential aspects of the research, including its purpose, benefits, and clinical implications. Next, they were asked for their informed consent, signed by the mother, father, or guardian for adolescents under 18 years. Eligible patients were evaluated with the instruments described above. Medical records were also analyzed to obtain data on their clinical history (psychiatric and medical diagnoses, hospitalizations, and treatments, among others) and social and family information such as sex, age, family composition, sexual orientation, and religious beliefs.
The instruments were applied by professionals (physicians, psychologists, occupational therapists, and nurses, among others) from the different health centers participating in the study.
Data analysis
The data were analyzed using the SPSS statistical program, version 25. Descriptive analyses were performed using frequency distribution and summary statistics. In addition, multiple correspondence analysis was used as a multivariate statistical analysis, allowing to study of many qualitative variables [28]. Although multiple correspondence analysis is considered an exploratory and descriptive technique, it distinguishes associations between categorical variables without statistical assumptions [29],[30]. Moreover, multiple correspondence analysis processes the collected data without establishing a priori relationships between the evaluated variables, visually representing the possible associations between the categories of variables [31]. As a result, multiple correspondence analysis provides a visual representation of the categories of variables considered in a two- dimensional space, using a transformation of the Euclidean distance, called Chi- square distance [28].
Ethics
The Scientific Ethics Committee of the Universidad Católica of Maule approved the project. Also, following the Declaration of Helsinki and Law 20 120 regulating biomedical research in Chile, the participants completed an informed consent as proof of voluntariness and knowledge of the implications of their participation.
Results
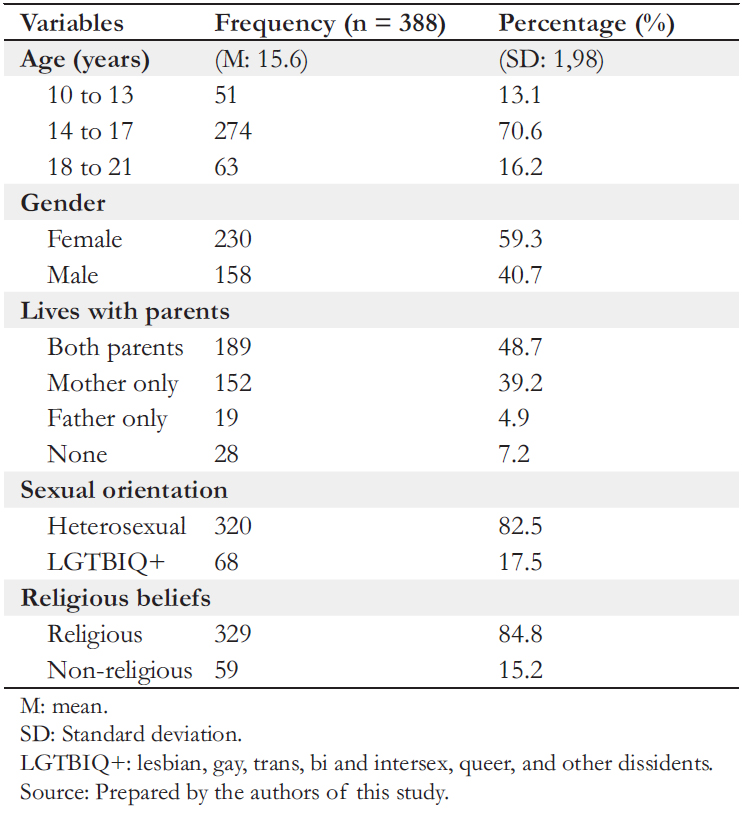
The sample consisted of 388 participants, 230 females (59.3%) and 158 males (40.7%), aged 10 to 21 years, with a mean age of 15.63 years (standard deviation: 1.98).
Of the social and family variables, 44.1% of the adolescents reported coming from a single- parent family, while 7.2% lived without their parents. Moreover, 82.5% identified themselves as heterosexual, and 84.8% reported having some religious belief (Table 1).
Regarding the psychological factors, 39.2% (152) presented high levels of impulsivity, and 70.9% (275) had problems regulating their emotions. On the other hand, 16.5% (64) of the adolescents did not seek help in the presence of any problem related to their mental health.
Regarding the clinical variables (Table 2), we found that 92.0% had been diagnosed with some psychiatric illness, the most prevalent being depressive (31.2%) and anxiety disorders (16%). In turn, 82% of the adolescents presented more than one mental health diagnosis (comorbidity), and 13.1% reported not receiving any treatment for mental disorders.
Regarding self- injury and suicidal behavior, 58.0% reported having self- inflicted non- lethal injuries. In addition, 30.4% reported passive suicidal ideation (death wish) during the last month, while 45.9% reported that they had done so once in their lifetime. Likewise, 18.8% reported active suicidal ideation during the last month, and 41.0% reported doing so in their lifetime. Regarding suicide attempts, 33.2% had a history of previous attempts, of which 55.0% had made two or more. The mean age for the first attempt was 13.6 years (standard deviation: 2.3).
Finally, 64.9% reported having been victims of some abuse or mistreatment, the most recurrent being bullying (46.9%), domestic violence (33.5%), psychological mistreatment (17.8%), and sexual abuse or harassment (14.7%).
Multiple correspondence analysis
Through the multiple correspondence analysis, we analyzed social, family, psychological and clinical variables, which were explored together with the history of suicide attempts. Although three multiple correspondence analyses (three types of variables studied) were required due to the large number of clinical variables evaluated, the researchers decided to segment the clinical variables into two groups (clinical history and current clinical status) given the visual nature of the interpretation. Therefore, a total of four multiple correspondence analyses were performed.
The first multiple correspondence analysis was performed considering the family and social variables and the history of suicide attempts. In this analysis, we observed that the absence of suicide attempts had a higher level of correspondence and is therefore characteristic of adolescents who reported being heterosexual, male, and having some religious belief. Likewise, we observed that the lesbian, gay, trans, bi, intersex, queer, and other dissidence (LGTBIQ+) and non- religious categories are associated with two or more suicide attempts. Moreover, being female is the character closest to adolescents performing a single suicide attempt (Figure 1).
The second multiple correspondence analysis explored the psychological variables and suicide attempts. We can see in the graph resulting from the analysis that adolescents without impulsivity and who seek help concerning mental health problems (formal and informal sources) correlate with adolescents without suicide attempts. Having a history of two or more suicide attempts is closer to adolescents with high levels of impulsivity and shows no association with the other categories analyzed. Moreover, emotional regulation did not correspond with any of the three categories of history of suicide attempts (Figure?2).
The third multiple correspondence analysis explored the association between clinical variables and suicide attempts. We found proximity between adolescents without suicide attempts and adolescents with no history of self- harm, domestic violence, bullying, harassment, or sexual abuse and no history of hospitalizations related to mental health. On the other hand, a single suicide attempt was closely related to having a history of self- injury and having been a victim of bullying or sexual abuse. Adolescents with a history of two or more suicide attempts were associated with a history of sexual abuse or harassment and previous hospitalizations due to mental health problems (Figure 3).
In the fourth multiple correspondence analysis, we explored variables linked to the current clinical status of the subjects and suicide attempts. The resulting graph showed that adolescents with no suicide attempts had a stronger association with adolescents without anxious- depressive symptoms, insomnia, or suicidal ideation. Likewise, the category representing adolescents with two or more suicide attempts shows a higher level of correspondence with anxious-de pressive symptoms, stress, insomnia, and suicidal ideation during the last month. Moreover, performing a suicide attempt reached its highest level of correspondence with having suicidal ideation once in a lifetime (Figure 4).
Discussion
The results of this study align with previous findings [4],[5], con-firming a higher frequency of suicide attempts in women than in men, being 42.6% and 20.3%, respectively.
In addition, 76.2% of adolescents with a history of suicide attempts reported non- suicidal self- inflicted injuries. Although their association has already been demonstrated [17], it could be associated with an increased risk of suicide attempts [16].
Even if the participants in this study were receiving clinical care, they presented high levels of anxious- depressive symptomatology and stress. This is concerning, given that depressive and anxiety disorders are directly related to suicidal ideation and are associated with other factors that increase suicide risks, such as impulsivity, sleep disorders, deficits in emotional regulation, refusal to seek help for mental health problems, and substance abuse [25],[32],[33],[34],[35],[36],[37].
Although adolescent mental health evidence is scarce, an epidemiological study conducted in four regions of the country found that only 33.3% of the subjects who presented a mental disorder had sought some help during the last year (formal or informal). This same study showed an assistance gap, as 66.6% of children or adolescents with a mental disorder did not receive care, increasing to 85% when only the formal health system is considered [38].
Our results and the analyzed evidence shows the low effective-ness of national mental health programs for treatment and follow- up of adolescent patients. We found that 45.4% of adolescents preferred to seek help from non- formal sources or not seek help at all (16.5%) when faced with difficulties related to their mental health. Therefore, improving current mental health care and having effective and easily accessible mental health prevention and intervention programs is essential.
Unlike other techniques, multiple correspondence analysis allowed us to identify underlying relationships between the categories of variables, improving the understanding of this com-plex phenomenon. In particular, our results showed differentiating characteristics in adolescents with two or more suicide attempts and those with a single attempt. These characteristics include anxious- depressive symptomatology, impulsivity, stress, insomnia, and suicidal thoughts during the last month.
Suicidal behaviors and self- injury in adolescents are a public health problem worldwide. Although there is consensus on the importance of developing more effective interventions to reduce their risk, there are still many limitations and challenges to their early and timely management and prevention. Several reports show that, despite national and international efforts to prevent suicide, it has not been possible to reduce the rates of adolescent suicide [7],[8].
Conclusions
We found that adolescents with a history of a single suicide attempt are characterized by being female, having suicidal ideation at some time in their lives, having a history of self- harm, and being victims of bullying or sexual abuse.
On the other hand, adolescents with two or more suicide attempts are characterized by not having any religious beliefs, identifying themselves as LGBTIQ+, having high levels of impulsivity, presenting anxious- depressive symptoms, stress, insomnia, and suicidal ideation during the last month, as well as having a history of hospitalization associated with mental health problems.
These preliminary results can be used to develop complex models that contribute to understanding adolescent suicidal behavior.