Protocolo
← vista completaPublicado el 15 de diciembre de 2022 | http://doi.org/10.5867/medwave.2022.11.2570
Video-retroalimentación Focalizado en los Recursos para mejorar la sensibilidad en díadas madre-infante con síntomas depresivos: protocolo de un ensayo clínico aleatorizado piloto
Strength-based Video-feedback to improve maternal sensitivity in mother-infant dyads with maternal depressive symptoms: Study protocol for a randomized controlled feasibility trial
Abstract
Introduction Maternal sensitivity and mentalization are fundamental for children’s mental health development. These skills have been negatively associated with maternal postpartum depressive symptomatology. Moreover, its prevalence increases in low socioeconomic and psychosocial risk contexts, where the access to treatment is scarce. Even though Attachment Based Interventios, such as Video-Feedback has been internationally recognized as an effective intervention. Its cost, as well as the need for language translation and cultural adaptation makes it difficult to implement in Latinamerican countries.
Aim The present study aims to assess the feasibility and acceptability of an online Video-Feedback intervention informed n mentalization aimed at mother-infant dyads with depressive symptomatology who attend Chilean public health centers.
Method This is a pilot randomized clinical trial with two groups of 60 mother-infant dyads between 4 and 12 months of age. Participants will be randomly assigned to control and experimental groups in a 1:1 ratio. Even though both groups will receive usual treatment, the experimental group will also receive the present video-intervention. At the end of the study, feasibility will be assessed based on focus groups aimed at interveners and quantitative outcomes such as recruitment rate, questionnaire completion rate and intervention completeness. Acceptability will be assessed from in-depth interviews with participants. In addition, effect sizes of primary and secondary outcomes will be calculated.
Expected results Results are expected to generate parameters to design a larger-scale clinical trial and to preliminary assess the effect of the reported mentalization-informed intervention on maternal sensitivity. Additionally, it seeks to contribute with a mental health intervention for low-income mother-infant dyads, which can be implemented remotely, at a low cost, and that would be suitable for implementation at a mental health care system policy.
The protocol of this trial’s design was registered at Clinical Trials (NCT04748731).
Main messages
- Depression in the perinatal period is highly prevalent disease and negatively affects maternal and infant mental health.
- Video-feedback interventions aimed at promoting attachment and mentalization are cost-effective worldwide. However, training is costly and needs cultural adaptations.
- The design of protocols that evaluate the implementation of brief and culturally sensitive interventions is required.
Introduction
Peripartum depressive symptomatology is a public health priority due to its high prevalence [1] and impact on maternal negative consequences and child development [2]. The challenges of early parenting have been shown to increase the risk of mental health problems, especially in women. In a meta-analysis, Shorey et al. (2018) describe an incidence and prevalence of postpartum depression of 12 and 17%, respectively. In Chile, it is estimated that between 16 and 20% of women are at risk of postpartum depression within the first six months after childbirth [3]. In children, a greater risk of suffering depression throughout life has been described [4], as well as negative consequences in affective, cognitive, and behavioral development [5,6]. The care response for this population, especially in contexts of psychosocial risk, is a cost-effective [7] and effective [8,9,10,11,12,13,14] public health measure at the international level. In this context, attachment-based interventions using video feedback are a good example of a brief and cost-effective tool to reduce depressive symptomatology, improve maternal sensitivity, and increase the security of infant attachment [13,15,16,17]. However, Chile does not have guidelines to implement such evidence-based practices at the public health level [18,19].
Local barriers to achieving this objective include the difficulty of translation, cultural adaptation, copyright, and training costs [20]. In this sense, local interventions have been developed to respond to public mental health care’s specific needs, vulnerabilities, and cultural characteristics. Thisvideo intervention focused on resources (VI-FR) is an attachment-based intervention developed in 2012 to reduce depression and promote maternal responsiveness. This method has been applied for ten years by mental health professionals trained in a university diploma program and used in clinical practice in a perinatal mental health program at the same university four years ago. Preliminary studies have shown to improve parental sensitivity, decrease postpartum depressive symptomatology, and improve infant socio-emotional development [21,22,23].
The resource-focused video intervention is a brief intervention, flexibly structured to be tailored to each mother-baby dyad. Specifically, the intervention seeks to:
-
Increase "shared pleasure" in the dyad, activating reward circuits that reinforces mother and infant to repeat this experience.
-
Improve the maternal sensitive response using mentalization as a mechanism.
-
Reduce maternal hostility, reinforcing positive interactions observed in videos and reflecting on complex or dysfunctional aspects.
The aim is to observe the positive interactional patterns and talk about challenging aspects by quoting the mother herself in functional episodes, observed in order to rethink complicated interactions and discover new ways of dealing with them. According to local experience [23], these objectives can be accomplished in four sessions to complement existing maternal and infant mental health services.
The resource-focused video intervention considers the therapist’s attitude as a key factor: he/she is positioned not as an expert but as a collaborator with curiosity and doubts. Therapists are trained in trauma and its intergenerational transmission, capable of recognizing and validating the experience of the other, and regularly participating in reflective supervision groups.
At the same time, the COVID-19 health crisis highlighted the overload of the health system and the need for remote mental health care during the postpartum period aimed at public service users with clinical symptomatology [1,24]. The resource-focused video intervention seeks to respond to these needs straightforwardly and remotely, using a strategy that has shown promising results in this population [25].
Considering the above, the study presents a brief, online intervention based on attachment theory and using video feedback to improve parental sensitivity in depressed, low-income mother-baby dyads and users of Chilean public health services. This model is expected to:
-
Provide a remote postpartum mental health intervention for low-income dyads with restricted access to face-to-face care [26].
-
Low-cost, evidence-based, and suitable for scale-up to public mental health care.
Objective
To assess the feasibility and acceptability of a resource-focused video-feedback intervention for mothers with depressive symptoms and their children to design a larger-scale randomized clinical trial. As a secondary objective, we seek to evaluate the intervention’s effect on maternal sensitivity preliminarily.
Main results (trial feasibility)
-
Recruitment rates for participation and randomization.
-
Retention and follow-up rates as participants progress through the trial.
-
Rates of adherence to study procedures, intervention attendance, and engagement.
-
Effect size in maternal sensitivity (calculating sample size in randomized clinical trials).
-
Progression criteria for a definitive trial.
Methods
This study has the full ethical approval of the local Ethics Committee (Comité de Ética Científico de Medicina, Pontificia Universidad Católica de Chile, ID 201201009, date 17-12-20). Written informed consent will be obtained from the participants. This trial was registered in February 2021 in Clinical Trials, registration number NCT04748731 (
Design
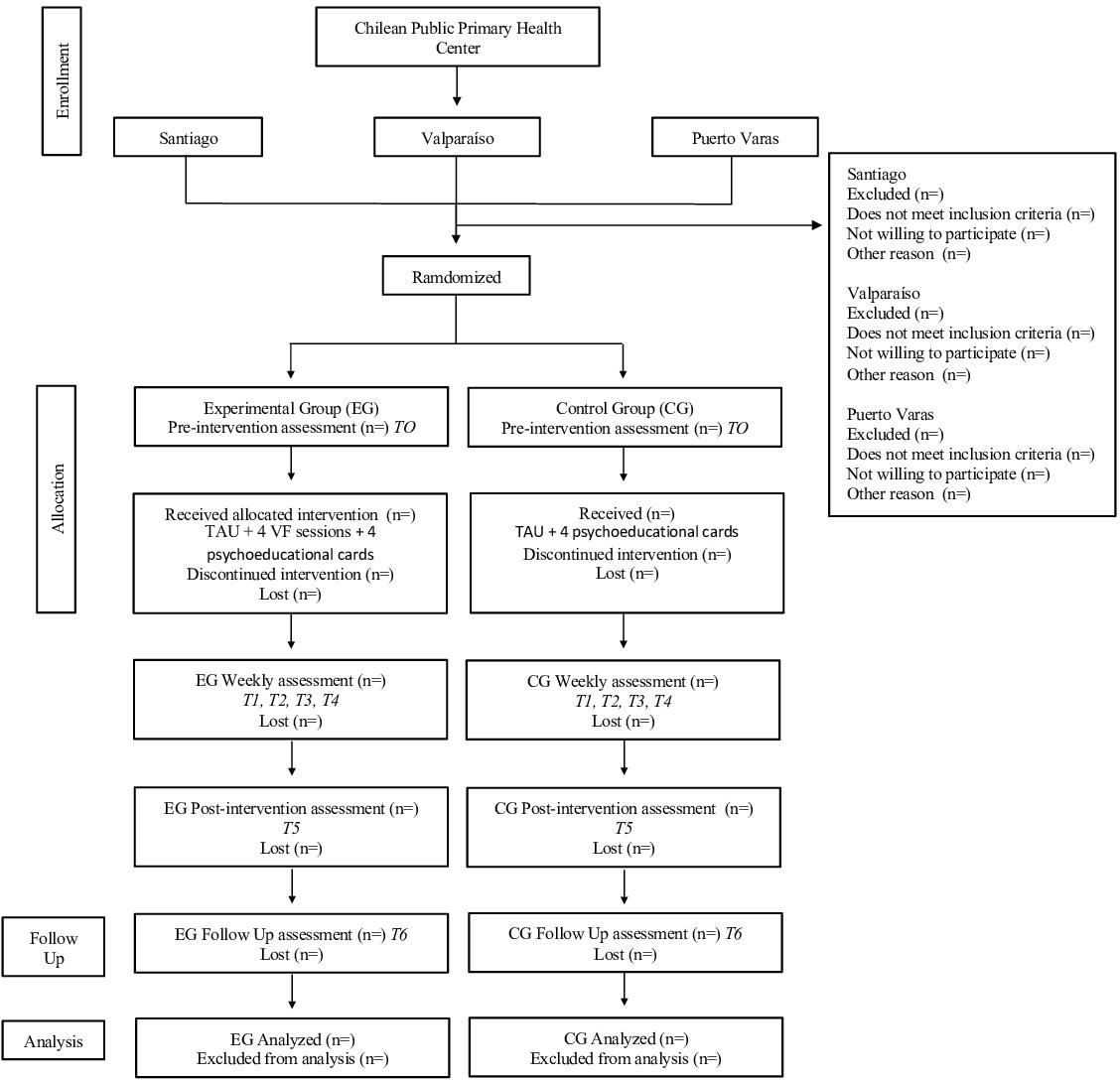
Pilot randomized clinical trial with two parallel groups of mothers with depressive symptomatology and their infants. Both groups will receive the usual treatment plus psychoeducational material. Only the experimental group will receive the intervention with the proposed resource-focused video-intervention model. Details on the chronology of the study are presented below in Figure 1.
Recruitment, randomization, follow-up, and analysis flowchart.
Setting
As shown in Figure 1, the recruitment, intervention, and data collection will be conducted entirely online. Participants will be referred to the study from five primary care centers in Santiago, Valparaíso, and Puerto Varas. The Chilean public health system provides free care to the two poorest segments of the population [27]. The virtual platform will be Zoom – a videoconferencing service identified as a valuable and secure tool for conducting research interviews and has demonstrated acceptability [28].
Sample size
It was estimated considering its usefulness in providing information to assess feasibility. Guidelines for developing pilot randomized clinical trials consider 30 participants per group as a reasonable number to reliably estimate the variation among participants' outcomes [29] and estimate the standard deviation of outcome variables and the correlation coefficient between baseline and follow-up scores [30]. Considering the above, we expect to invite 570 mothers to recruit 72 in the trial and end up with 60 participants at follow-up (30 for each arm).
Eligibility criteria
Regarding eligibility criteria, this study include women aged 18 years or older who are:
-
Mothers of infants between 4 and 12 months of age.
-
Users of public health care.
-
Scoring five or more points on the Edinburgh Postnatal Depression Scale during routine assessments in their care centers.
-
Fluent in Spanish.
Patients will be excluded with the presence of:
-
Maternal severe intellectual deficit and/or psychotic symptoms.
-
Severe developmental disorders in infants.
-
Identification of current family violence and legal proceedings for violation of rights.
The participants' referral medical centers will evaluate eligibility criteria.
Instruments
Table 1 summarizes all of the study’s assessment instruments.
Intervention
In addition to usual primary public healthcare, the dyads in the control group will receive four psychoeducational parenting cards via weekly text messages.
The intervention is delivered online by trained clinical psychologists (30 hours of training). The implementation considers a pre-assessment session and four one-hour intervention sessions with the same structure (Figure 2). All sessions are recorded for supervision.
Summary of intervention elements.
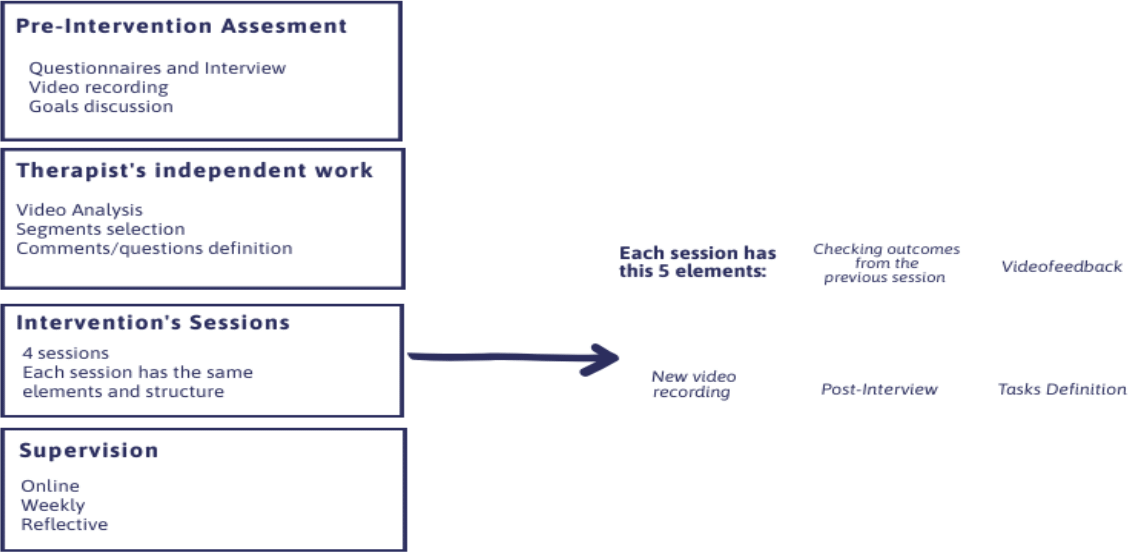
As shown in Figure 2, the elements of the intervention process are as follows:
-
Pre-assessment: 90 minutes. It considers the application of instruments to the mother, the infant, and the dyad. We intend to explore the mother’s concerns about the child, their relationship and maternal role, the reason for the consultation, and the objectives of the intervention.
-
Autonomous work of the therapist: 60 minutes, weekly frequency. This activity aims to review the case’s clinical background, analyze the interaction observed in the video and its possible association with maternal concern and infant distress. From this information, the therapist elaborates the script for the feedback and observation of the video with the mother.
-
Intervention sessions with video feedback: 60 minutes, weekly frequency. The main objective is observing the interaction videos and their analysis, seeking to promote reflection in the mother about the internal states in her and the child, the underlying needs, the mutual influence, and the elements of her childhood history that relate to elements of the observed interaction. The session is conducted online by the same therapist who conducted the initial assessment. From the second session onwards, changes observed from the tasks defined in the previous session are reviewed with the mother.
-
Video recording: each session considers the video recording of an interaction from a new task (e.g., playing, feeding, singing).
-
Post-video interview: after each video recording, a semi-structured interview addresses the mother’s subjective experience during the interaction and the experience she imagines her child had.
-
Definition of tasks or practices between sessions: at the end of each session, possible activities to be carried out during the week are defined together, taking into account the mother’s discoveries or new learning.
-
Supervision: the team of therapists meets weekly for two hours to supervise the intervention processes. The objective is to address challenges that arise in the intervention, evaluate progress and ensure fidelity to the model. A reflective methodology [31] is used during supervision, which considers each participant’s experience. The supervisor and the clinical team act as support figures for the therapist.
Procedure
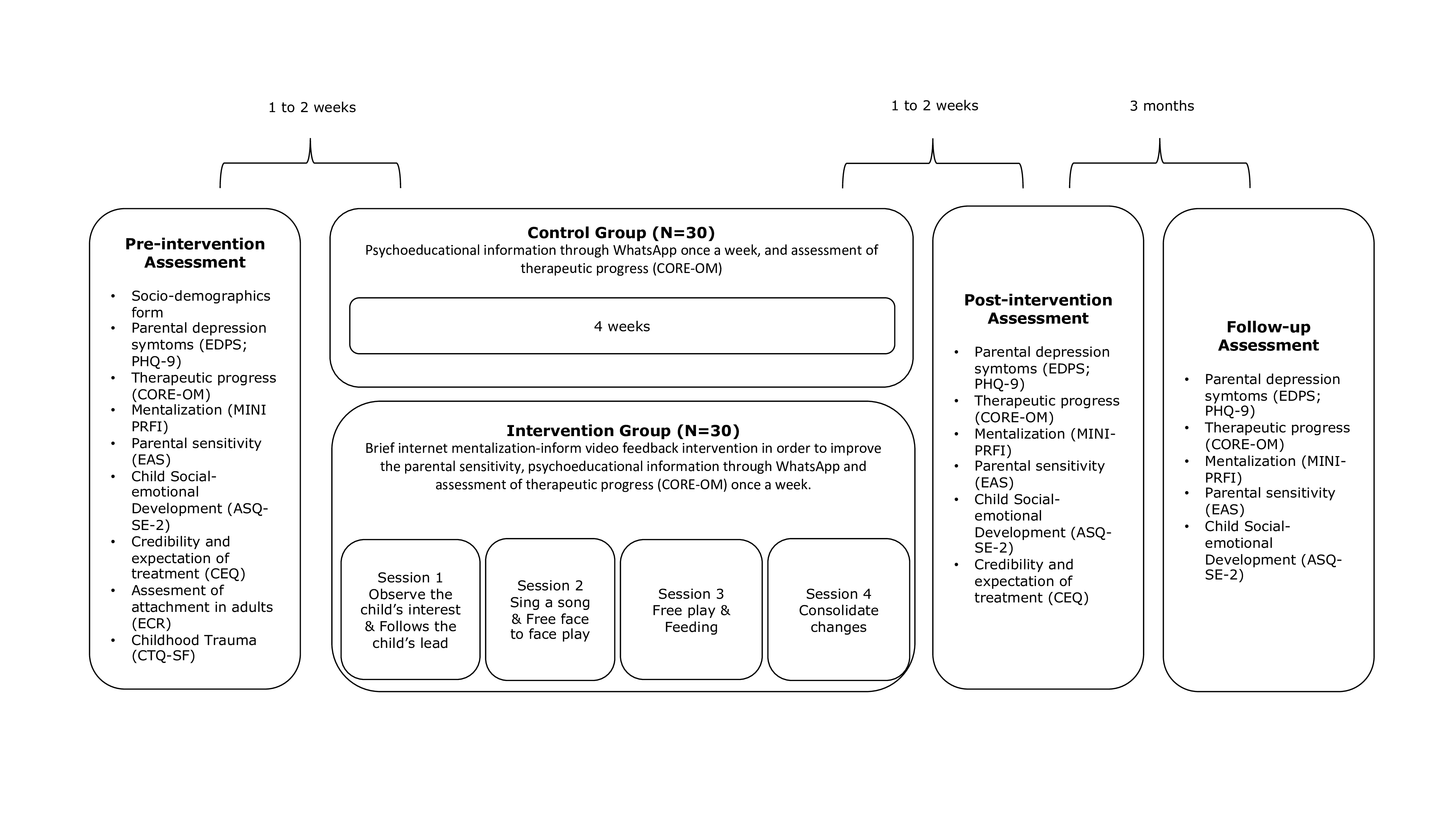
Professionals from the collaborating healthcare centers will verify compliance with the inclusion/exclusion criteria and invite to participate in the study. Those who agree to participate will be assigned to a group (experimental or control), and will be contacted for the initial assessment, in which, after informed consent signing, the following variables will be evaluated: depressive symptoms, maternal sensitivity, socioemotional development of the child, adult attachment, adverse childhood experiences, credibility and expectations about the treatment and therapeutic progress. After the initial assessment, the same therapist who performs the assessment will begin with the interventions according to the assigned group. Once the intervention is completed, a different therapist will perform the post-assessment and the three-month follow-up. The assessments and interventions are detailed in Figure 3.
Intervention and evaluation process flowchart.
Randomization and blinding
Participants will be randomly assigned to the control or experimental group in a 1:1 ratio. A sequence of random numbers will be generated from permuted block sizes of two and four using Study Randomized®. The sequence will be administered by an external person who will contact the study coordinator each time a participant joins the study. While participants and therapists may not be blinded, outcome assessors will be blinded.
Primary outcome measures: Feasibility of study objectives
Recruitment rates will be calculated from the number of signed consent participants. The percentage of the total number of invited and registered participants will be used. For each arm of the trial, the number of participants who withdrew or could not be contacted will be quantified. Data will be presented as a percentage of the total number of participants in each arm of the trial. The Consolidated Standards of Reporting Trials, CONSORT guidelines for pilot and feasibility studies will be followed (Annex 1
Standard deviations of continuous secondary outcomes related to maternal sensitivity will be calculated to estimate the sample size for a future trial. To estimate potential effect sizes for a primary outcome in a future trial (i.e., the change in scores on main and secondary outcomes before and after the intervention), we will calculate the difference between pre-intervention and post-intervention mean scores for the experimental trial and control groups and divide by the pooled standard deviation at baseline [33].
Progression to a definitive clinical trial will be decided based on the following criteria: recruitment rate over 70% of eligible consenting participants; questionnaire completion rate over 70% of participants (at time 1); and intervention completion rate over 50% of participants who attended all resource-focused video intervention sessions.
The acceptability of the intervention will be evaluated using in-depth interviews with the participants, aimed at finding out both the subjective effect of the intervention and their perception of the benefits and aspects to be modified. Feasibility will be evaluated through focus groups with therapists and health workers from the reference healthcenters to explore their assessment of the intervention. In addition, the success criteria previously mentioned will be considered for this objective.
Secondary outcomes will be changes in maternal responsiveness, reflective functioning, depressive symptomatology, and socio-emotional development.
Table 2 below summarizes the entire schedule of activities associated with the study:
Data analysis
Descriptive statistics will be used to determine the clinical and socio-demographic variables of the groups, the eligibility rate, recruitment rates, dropout rates, and participation-attendance rates, and to estimate the effect size between groups post-intervention and follow-up. To determine differences between groups, repeated measures analyses will be useds, controlling for a baseline for each outcome. Measures considering observation and coding will include at least two independent certified coders, and Cohen-κ will be used to estimate inter-rater reliability.
In-depth interviews will be analyzed using content analysis [34].
Discussion
Research in parenting and early childhood has demonstrated the importance of considering the mental aspects underlying behavior in understanding mother/parent-child interactions [35,36]. Parental mentalization addresses this aspect, and evidence shows that it plays a crucial role in increasing responsiveness and security of attachment [37,38]. Additionally, parental mentalization is fundamental for the development of affect and self-regulation [38,39,40,41,42], the intergenerational transmission of attachment [43,44], and the development of social and mentalization skills in infancy. However, video feedback interventions to enhance parental sensitivity often lack explicit consideration of mentalizing as one of the critical processes involved in maternal sensitivity.
The present study arises in response to the need to provide culturally sensitive interventions for low-income mother-infant dyads in contexts where face-to-face care is restricted. In this setting, online care offers a modality to address the need for care for postpartum depressive symptomatology [1,45].
The results of this pilot trial aim to provide evidence to adjust the intervention, define the required sample size and subsequently develop a larger randomized clinical trial to evaluate its effectiveness. The long-term purpose of the research is to contribute with a brief and cost-effective psychotherapeutic intervention based on attachment theory and video feedback. It is also intended that the intervention developed will be adaptable to the Chilean public health system.
