Revisión sistemática
← vista completaPublicado el 22 de mayo de 2026 | http://doi.org/10.5867/medwave.2026.04.3085
Efectos de terapia manual sobre dolor y funcionalidad en pacientes con fascitis plantar: revisión sistemática de literatura
Effects of manual therapy on pain and function in patients with plantar fasciitis: A systematic review of the literature
Abstract
Objective Plantar fasciitis is common and impairs people’s ability to move. Manual therapy is frequently used to treat plantar fasciitis. However, its effects are inconclusive. For this reason, the purpose of this systematic review is to determine the effect of manual therapy on plantar fasciitis.
Methods A systematic review of the literature was conducted, following the PRISMA checklist. Five databases (CINAHL, Scopus, PubMed, Web of Science, and OVID) were searched, along with a review of the gray literature and a manual search. Randomized clinical trials from 2014 to 2024 were selected that examined the efficacy of manual therapy in reducing pain intensity and improving function in patients aged 18 to 60 years with a clinical diagnosis of plantar fasciitis. Methodological quality (PEDro scale) and risk of bias (risk of bias scale) were assessed.
Results Four randomized clinical trials (n = 224) were included, reporting controversial statistical differences in pain and function. In addition, two studies reported clinically relevant changes favoring manual therapy. PEDro scale scores ranged from 4 to 6, and three studies presented a high risk of bias.
Conclusions The effects of manual therapy on pain and function in patients with plantar fasciitis are uncertain. The evidence is limited, heterogeneous, and lacking in methodological rigor. A larger number of randomized clinical trials with more consistent, replicable protocols are needed to determine the contributions of manual therapy to improving pain and function in patients with plantar fasciitis. Similarly, the inconsistency and limited evidence on indicators of clinical significance in the selected studies preclude an assessment of the clinical impact of this intervention.
PROSPERO registration CRD42024501550.
Main messages
- Plantar fasciitis is a common condition in the general population that has been treated with non-invasive methods, particularly manual therapy, the effectiveness of which is uncertain.
- This study evaluates the isolated effect of manual therapy, unlike previous reviews in this field, where manual therapy was included as part of a multimodal treatment regimen.
- The limitation of this study lies in the inability to complement the qualitative analysis with a quantitative analysis, due to the variety of measurement instruments, application techniques, and different time points at which the outcomes of interest were assessed.
Introduction
The plantar fascia is a broad, thick band of connective tissue that originates at the calcaneus and attaches to the forefoot at three distinct sites [1]. The central band supports the longitudinal arch of the foot, acting as a windlass mechanism during the stance phase of gait [2]. In turn, this structure may cause pain due to perifascial edema from microtears at the calcaneal insertion site, leading to plantar fasciitis or plantar fasciosis [3,4,5,6]. Plantar fasciitis has a prevalence of 9.6% in the general population, preferentially affecting adults between 40 and 60 years of age [7,8]. It is associated with several major risk factors, including increased plantar flexion range of motion, high body mass index, and increased tension in the posterior calf muscles [9,10,11].
One of the non-invasive interventions used for plantar fasciitis is manual therapy, defined as the application of force to body tissues using the hands or other body parts, tools, or modalities, with therapeutic intent [12]. It includes thrust manipulation, joint mobilization, soft tissue mobilization, and neurodynamic movements [13]. These interventions provide physiological mechanical effects, such as blood shear stress or tissue stretching, which induce the release of nitric oxide from endothelial tissue and blood cells, in addition to neurological effects related to the descending pain modulation pathway [14,15].
Systematic reviews and overviews of systematic reviews evaluating the effect of manual therapy in plantar fasciitis have been published from 2011 to 2018, with overviews extending to 2021. However, none of them have presented conclusive findings on the effects of manual therapy on variables such as pain and function in patients with plantar fasciitis [16,17,18,19]. Furthermore, previously published reviews have evaluated the effect of manual therapy in combination with different co-interventions [16,17,18], without further exploring their clinical significance; therefore, the isolated effect of manual therapy and its clinical impact remain unknown.
The aim of the present review is to determine the effect of manual therapy in patients with plantar fasciitis on pain reduction and improvement in functionality, based on a systematic search and updated analysis of randomized clinical trials in the field. It is expected that manual therapy, applied as a standalone intervention in patients with plantar fasciitis, will produce a significant reduction in pain and an improvement in functionality compared with other interventions or no intervention.
Methods
A systematic review of the literature was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Protocols (PRISMA) checklist [20]. The study was registered in the International Prospective Register of Systematic Reviews (PROSPERO) under registration code CRD42024501550.
Literature search strategy
The search strategy was developed using the “population, intervention, comparison, and outcome measures” framework to conduct a precise search [21]. The following is an example of the search strategy used for the CINAHL database: Heel-Pain (S1) OR Heel-Spur (S2) OR Plantar-Fasciitis (S3) OR Policeman’s-Heels (S4) OR Heel-Spur-Syndrome (S5) OR Chronic-Plantar-Fasciitis (S6) OR Calcaneal-Spurs (S7) OR Musculoskeletal-Pain (S8) AND Manipulations-Musculoskeletal (S9) OR Manipulation-Therapy (S10) OR Manipulative-Therapy (S11) OR Manual-Therapies (S12) OR Manual-Therapy (S13) AND Pain (S14) OR Function (S15). The complete search strategy is described in Supplementary Material 1.
The population consisted of patients diagnosed with plantar fasciitis; the intervention studied was isolated manual therapy techniques; and the comparison groups included control, placebo, and sham interventions. The primary outcomes were pain intensity and functionality. To develop the search strategy, four articles related to the topic were selected, and the search terms were obtained from the titles, abstracts, and keywords of each article [16,17,18,19].
Two investigators, with a third reviewer serving as a tiebreaker in cases of disagreement, conducted an exhaustive search of the available literature. The databases used were CINAHL, Scopus, PubMed, Web of Science, and Cochrane. The applied filters were related to the time frame and restricted to randomized clinical trials only. Duplicate articles identified through the search strategy were removed using a tool called Rayyan [22]. A gray literature search was also conducted using the Google search engine, reviewing the first 10 pages of results. In addition, a manual search was performed.
Selection process
Two investigators (MIA, JGM) independently conducted the search and article selection process. Disagreements were resolved by consensus with the participation of a third reviewer (JYV). Potential publications were selected by screening titles and abstracts for the inclusion of the intervention under study and the assessment of the variables of interest. Potentially eligible studies were retrieved, and the full-text articles were reviewed before applying the inclusion and exclusion criteria.
Eligibility criteria
Studies were considered eligible if they met the following criteria:
-
Plantar fasciitis had to be diagnosed.
-
Randomized clinical trials had to be published in journals between January 1st, 2014, and April 1st, 2024.
-
Studies had to report the isolated efficacy of manual therapy, along with changes in pain intensity and functionality.
Studies were excluded if they met any of the following criteria:
-
Editorial letters, books, pilot studies, or qualitative studies.
-
Studies including healthy subjects under an induced experimental pain paradigm.
-
Studies involving heel pain lesions of arthritic, infectious, neuropathic, traumatic, tumoral, or vascular origin.
Data collection process
Data extraction was performed using a standardized Excel spreadsheet that included multiple categories: article information (authors, year, design, country); population information (eligibility criteria); study groups; intervention characteristics (type of treatment, duration, number of sessions); and outcome measures, results, and clinical significance. Two investigators (MIA, JGM) independently participated in this phase. In the event of disagreement, a third reviewer (JYV) was involved and made the final decision. The most relevant information from the selected studies is presented in Table 1.
The main variables analyzed in this review were pain intensity [27], pressure pain threshold [28], and functionality [29]. Secondary variables included flexibility (range of motion and popliteal angle grading), quality of life, and body mass index.
Methodological quality and risk of bias
Methodological quality was assessed using the Physiotherapy Evidence Database (PEDro) scale, which comprises 11 items assessing a study’s external and internal validity. Each item is evaluated as either fulfilled (yes) or not fulfilled (no) [30]. Risk of bias was analyzed using the updated version of the Cochrane Collaboration tool (RoB 2), which considers five domains evaluated as follows:
-
Y: yes.
-
PY: probably yes.
-
PN: probably no.
-
N: no.
-
NI: no information.
An algorithm determined the overall risk of bias as low-risk, some concerns, or high-risk [31]. Both scales were independently applied by two reviewers (MIA, JGM). A third reviewer (JYV) intervened in cases of disagreement.
Clinical effect and effect size
The clinical change and effect size of manual therapy were determined in patients with plantar foot pain and the associated disability. Effect size refers to the magnitude of an outcome [32]. The term effect size may refer to the magnitude of an unstandardized effect (for example, the difference between group means, relative risk, or odds ratio) or standardized effect sizes (such as “correlation” or “Cohen’s d”) [33]. Effect size provides information about the magnitude of the association between variables and the size of the difference between groups [33,34]. Likewise, effect magnitude has been interpreted as an index of clinical relevance. The greater the effect size, the greater the difference between groups and the greater the clinical relevance of the findings [33]. According to Cohen’s guidelines, values of 0.2, 0.5, and 0.8 are considered small, moderate, and large mean-difference effect sizes, respectively [35]. Complementing this categorization, a criterion for effect size definition proposed for rehabilitation research was also included, with values of 0.14 (small), 0.31 (moderate), and 0.61 (large) [36].
Certainty of evidence and strength of recommendation
The Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach was used to perform an overall assessment of the quality of evidence across five domains: risk of bias, inconsistency of results, indirect evidence, imprecision, and publication bias [37,38]. This system allows assigning a summary rating to the body of evidence regarding the effect of an intervention on a specific outcome measure, thereby facilitating the formulation of recommendations that guide clinical decision-making. After applying the GRADE approach, the results were classified according to their level of evidence [37,38]. This assessment was conducted considering a review in the absence of the estimated effect [39].
Results
The search strategy identified a total of 4793 potentially eligible studies for this review, of which four were ultimately included. Figure 1 shows the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram illustrating the study selection process.
PRISMA flow diagram for study selection.
The flow diagram indicates that, of 4793 records identified across five databases, four studies were ultimately included after screening (titles/abstracts) and eligibility (full-text review) processes.
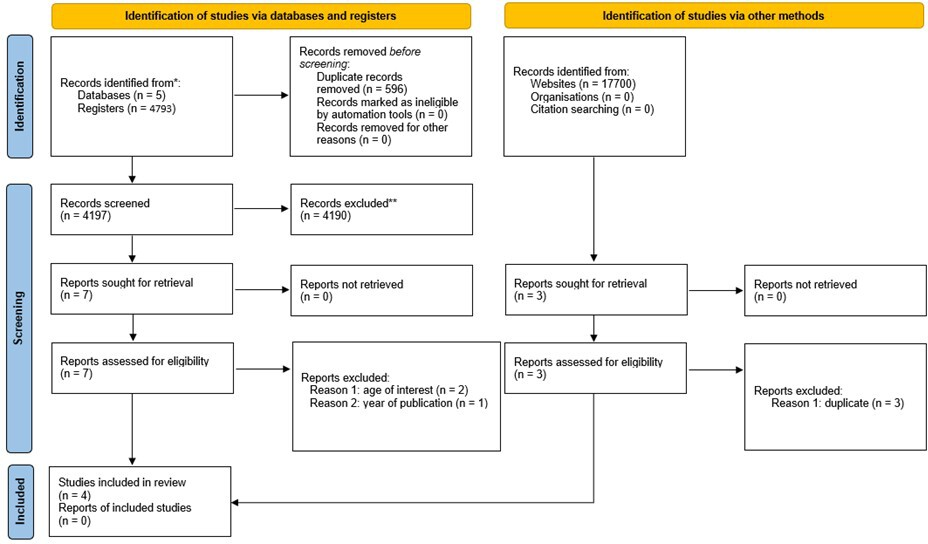
Source: Prepared by the authors based on the PRISMA proposal template.
The four selected articles were randomized clinical trials, including a total of 224 patients. Analysis of the intervention protocols revealed marked heterogeneity in the techniques used to address the same clinical condition. The interventions applied included manual therapy, particularly myofascial release [23,26]; joint mobilization [40]; custom foot orthoses [40]; the Gua Sha method [25]; structural diagnostic and management approach [26]; and cryostretching [25]. The detailed characteristics of each study are presented in Table 1.
Pain and symptomatology were evaluated in the four selected articles using different assessment tools: pressure pain threshold [23,25], the American Orthopedic Foot & Ankle Society ankle-hindfoot scale [40], the Foot Function and Pain Scale [40], the Numeric Pain Rating Scale [25], and the Foot Function Index, which includes five pain-related items [25].
Ajimsha et al. reported that the myofascial release group demonstrated a greater increase in pressure pain threshold compared with the control group (p < 0.01) [23]. Grim et al. reported that, at both the 1-month and 2 to 3-month follow-ups, the manual therapy group demonstrated greater improvements than the foot orthosis group and the combined therapy group (p < 0.01), both in the ankle-hindfoot scale and in the Foot Function and Pain Scale [40]. Jadhav et al. reported a statistically significant reduction in pain on day seven after the intervention in all three groups, as assessed by pressure pain threshold and the Numeric Pain Rating Scale (p < 0.001). Akter et al. reported that the structural diagnostic and management group showed significant improvements in pain, as measured by the Foot Function Index, compared with the myofascial release group (p < 0.01).
Functionality was evaluated in the four selected articles using two assessment tools: the Foot Function Index [23,25,26] and the Foot Function and Pain Scale [40].
The Foot Function Index results reported by Ajimsha et al. were controversial, showing statistically significant differences for the groups treated with myofascial release compared with the control group at 4 and 12 weeks (p < 0.001) [23]. In turn, the study by Jadhav et al. showed that the cryostretching group was significantly better than both the Gua Sha group (p < 0.001) and the positional release group (p < 0.001) [25]. Furthermore, in the study reported by Akter et al., the structural diagnostic and management approach group outperformed the myofascial release group (p < 0.01) [26]. Regarding the Foot Function and Pain Scale, significant improvements were observed, although the manual therapy group improved more (p < 0.01) than the other groups [40].
Clinical relevance reported by the authors
Table 1 details the reports on clinical relevance, which were explicitly reported only in the study by Grim et al. [40] and were retrospectively calculated for the studies by Ajimsha et al. [23] and Jadhav et al. [25]. Grim et al. [40] indicated that the manual therapy group showed a 35% change compared with the custom foot orthosis group, as measured by the American Orthopedic Foot & Ankle Society ankle-hindfoot scale. In the study by Ajimsha et al. [23], the effect size for the pressure pain threshold variable across the three measured time points ranged from d = 0.87 to d = 1.32 (large effect sizes) in favor of the manual therapy group compared with the control group. For Jadhav et al. [25], pain intensity, measured using the Numeric Pain Rating Scale, showed a large effect size (d = 1.16) in favor of the Gua Sha group compared with the positional release technique group. Meanwhile, for the pressure pain threshold variable, the effect size was d = 0.14 (small) in favor of the cryostretching group compared with the Gua Sha group.
Assessment of methodological quality and risk of bias
Table 2 describes the scores assigned by the evaluators to assess methodological quality, highlighting the studies conducted by Ajimsha et al. [23] and Jadhav et al. [25], which obtained a score of 6. Figure 2 shows the percentage of compliance with the PEDro scale criteria for the selected articles. According to these criteria, none of the studies fulfilled the blinded subjects or blinded therapists criteria. In contrast, random allocation and adequate follow-up were fulfilled in all articles.
Percentage compliance with PEDro scale criteria for selected articles.
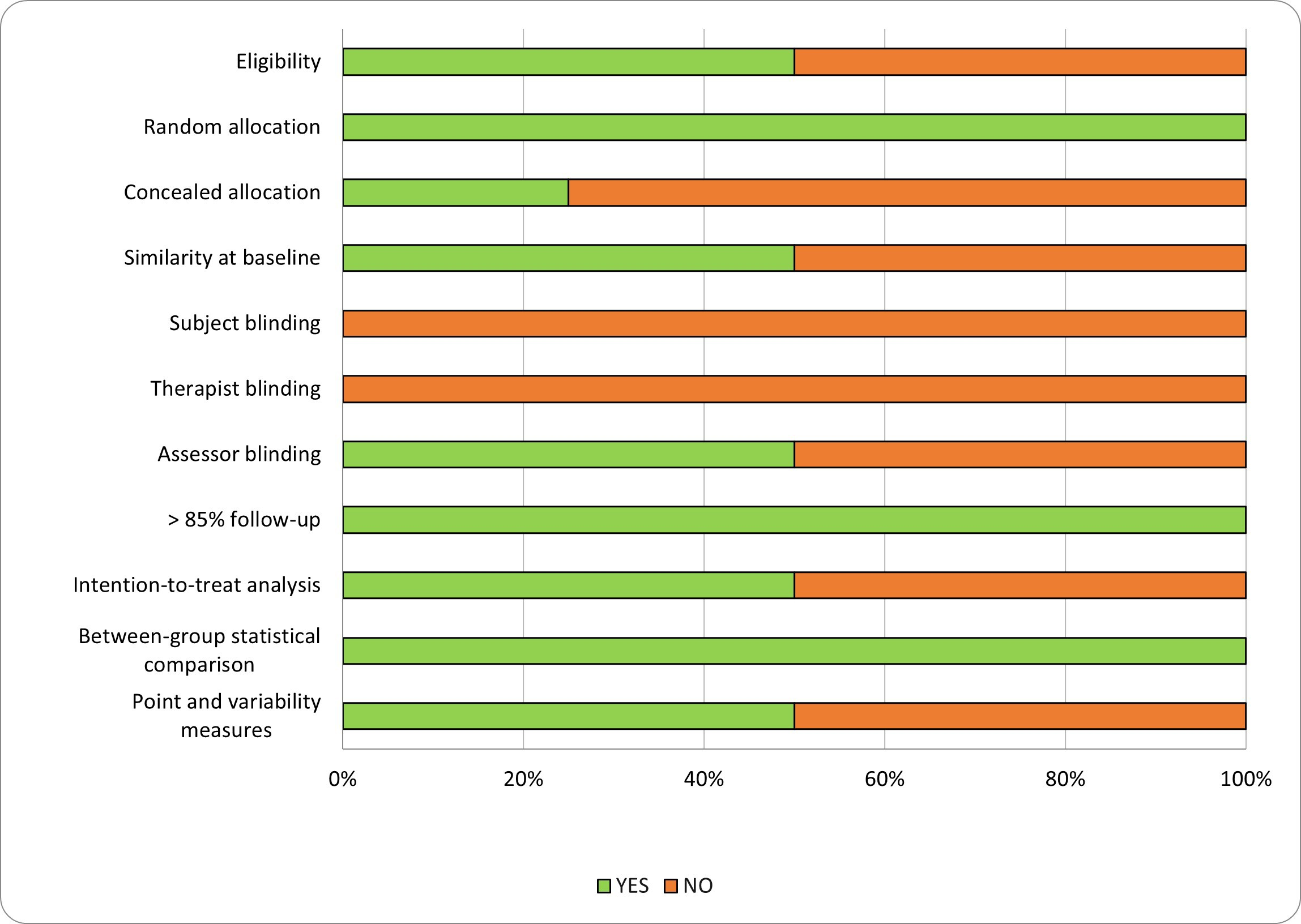
PEDro: Physiotherapy Evidence Database.
Source: Prepared by the authors based on the study results.
The risk of bias for each study and the overall risk are shown in Table 3 and Figure 3. Three of the four studies had a high risk of bias, and only one study obtained a risk-of-bias classification of “some concerns” [25]. The domain with the lowest level of compliance was “deviations from intended interventions” (50% of the studies) [23,26], which were categorized as “high risk of bias”, in contrast to the “measurement of the outcome” domain, in which all studies were classified as “low risk of bias”. For the domain “selection of reported results”, all articles were categorized as “some concerns”.
Percentage compliance with risk-of-bias scale criteria for selected articles.
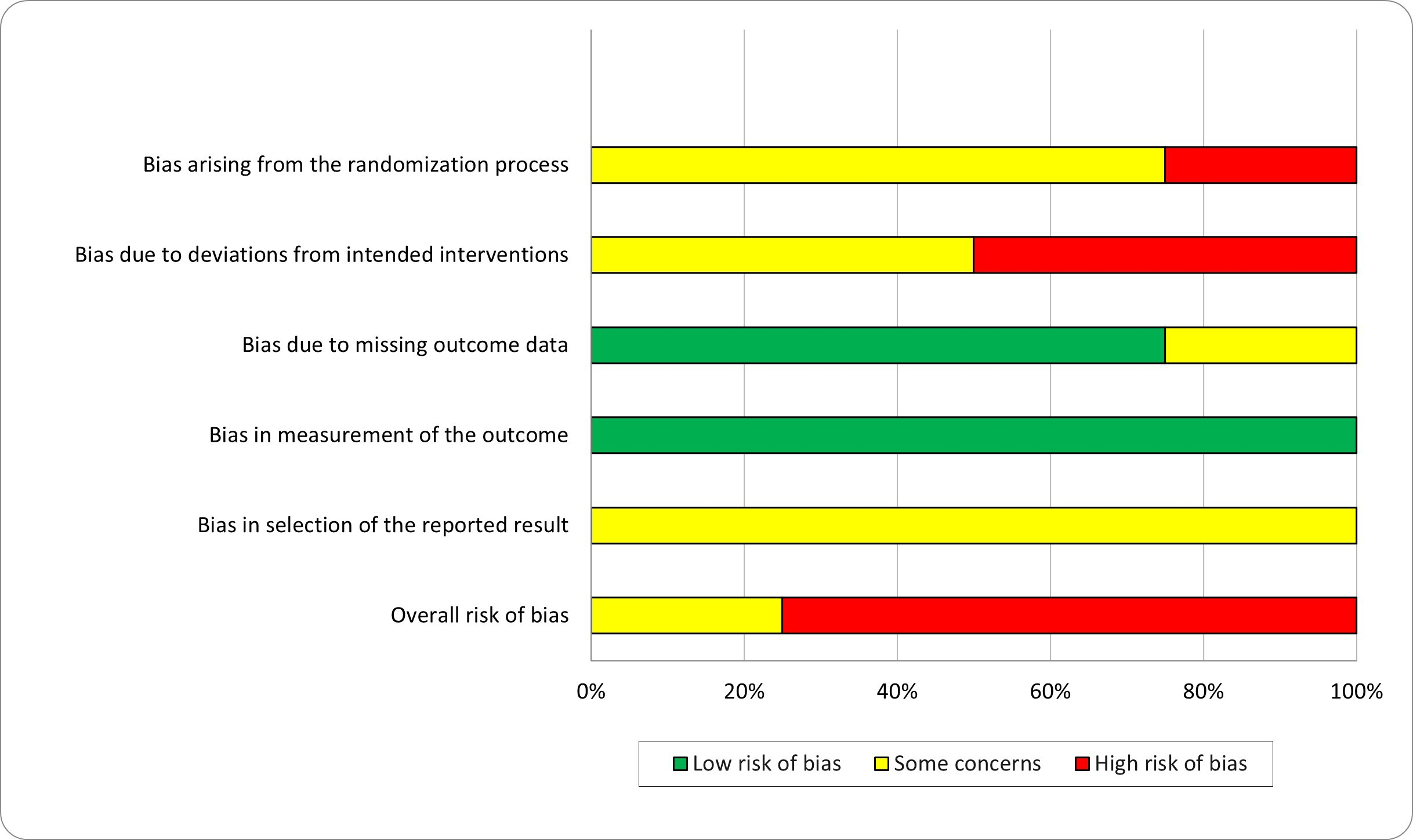
Source: Prepared by the authors based on the study results.
Certainty of evidence and strength of recommendation
Tables 4 and 5 describe the rating and judgment of the quality of evidence based on the GRADE analysis. Based on the analysis of pain intensity, the certainty of evidence was categorized as very low due to a high risk of bias (resulting from issues related to the randomization process, deviations from the intervention, and unclear or inadequate outcome data). In addition, there was serious imprecision and inconsistency because the total sample size was small, generating controversial and imprecise results (wide confidence intervals).
Discussion
The interventions used for plantar fasciitis, as described in this review, were manual therapy (myofascial release) [23,26], joint mobilization [40], custom foot orthotics [40], the Gua Sha method [25], a structural diagnostic and management approach [26], and cryostretching [25]. In all of them, manual therapy was the most common intervention. For both the pain and functionality variables, results were controversial, as some studies found statistically significant differences for groups receiving manual therapy [23] while others did not [26], regarding both pain and functionality.
The analysis of the results raises important points for discussion. First, it is important to note the small sample size analyzed (n = 224). Although the few selected studies reported positive effects of manual therapy, it is well known that in systematic reviews, small sample sizes can be associated with lower statistical power and, consequently, with differences between groups [41] or an increased risk of Type II error [42]. Another consequence of small sample sizes in systematic reviews is the limited generalizability of the review's results and conclusions [43]. Second, the review of the selected studies demonstrates heterogeneity in the intervention protocols used for this condition. For example, it is interesting to note that there is a wide variety of protocols regarding the number of sessions per week, the time allocated, and the choice of techniques. This suggests that the effects of treatment may depend on the dosage (time and number of techniques used) and the number of sessions, among other factors.
Among the most notable studies in this review is the work by Ajimsha et al. [23], who used myofascial release techniques over 12 sessions, with a 12-week follow-up after randomization, employing the Foot Function Index to assess function and the pressure pain threshold to assess pain. This study explored the clinical significance of the results for each variable evaluated in the studies. A growing trend in intervention studies is to accompany hypothesis testing with a measure of effect magnitude, or effect size; doing so provides an estimate of the effect size observed in subjects receiving the intervention. Despite growing interest in this topic and efforts to raise awareness, reporting of clinical significance in rehabilitation remains insufficient [44,45]. These findings are confirmed in our review, where most of the included articles do not report clinical significance values or indicators. Of the four selected articles, only one study reported this. Using the data provided in two of the studies, this indicator was calculated. The study by Grim et al. reported a 35% improvement in favor of the manual therapy group on the Foot and Ankle Orthopedic Society Ankle and Hindfoot Scale, classifying this as a “much better” change [46]. Ajimsha et al. [23] reported effect sizes for pressure pain threshold ranging from d = 0.87 to d = 1.32 in favor of the manual therapy group compared with the control group. These results were considered to represent a large or clinically relevant effect size, according to Cohen [35] and Kinney [36]. Finally, Jadhav et al. [25] reported an effect size of d = 1.16 for the Gua Sha group compared to the positional release technique group regarding pain intensity, as measured by a numerical pain rating scale. These results were considered to represent a high (clinically relevant) effect size. Furthermore, for the pressure pain threshold variable, the effect size was d = 0.14 in favor of the cryostretching group compared to the Gua Sha group, which is a clinically modest change according to the criteria of Cohen [35] and Kinney [36].
The results of this review show effect sizes ranging from low to high, reflecting considerable heterogeneity in the clinical response to manual therapy in patients with plantar fasciitis. This variability suggests that the efficacy of manual therapy may depend on individual patient factors, the therapist’s experience, and its combination with other therapeutic strategies. Consequently, although manual therapy can be considered a valid therapeutic option within a multimodal approach, its recommendation should be made with caution and based on the specific characteristics of each case.
Given the limitations of statistical significance (p value) when interpreting the results of a study, reporting clinical significance and providing a clinical interpretation of these results should be a priority in physical therapy intervention studies. In intervention studies, it is important to assess the risk of bias. This risk is particularly associated with the study's internal validity, which affects the reliability of its conclusions.
The included studies have methodological limitations and biases that reduce confidence in their conclusions. This finding is consistent with systematic reviews that report similar results [16,17].
In line with previous reviews, the effects of manual therapy on plantar fasciitis remain uncertain. This necessitates new trials to better understand the effect of manual therapy on plantar fasciitis. However, the results reported by Ajimasha et al. [23] are noteworthy, as they demonstrated that myofascial release reduces pain in subjects with plantar fasciitis. This study has a PEDro score of 6.
When applying the risk-of-bias tool, three of the four articles were categorized as having a “high risk of bias.” The items with the lowest compliance were “deviations from planned interventions” (none met the criteria) and “selection of reported outcomes” (all categorized as “some concerns”). This is mainly due to the nature of rehabilitation studies, in which participants are aware of the assigned intervention and outcomes are self-reported or depend on the evaluator’s judgment.
These criteria have been recognized as a significant source of various biases (selection, assessment, etc.). Several epidemiological studies, particularly in medicine, have found a significant association between randomization, inadequate allocation concealment, and overestimation of the reported effect [47,48,49,50,51]. These results are consistent with another meta-epidemiological study that investigated the impact of selection bias on effect size estimates in clinical studies across different areas of physical therapy. It found that inadequate blinding led to an overestimation of treatment effects when compared to studies with adequate blinding [52].
The certainty of the evidence for this review is very low. This is primarily due to risks of methodological bias, imprecision in sample sizes, and clinical heterogeneity among the included studies. Consequently, the strength of the recommendation should be considered weak or conditional. This implies that its clinical use may be justified in specific contexts, especially when patient preference is prioritized or other therapeutic options have been exhausted. However, additional research with more rigorous designs is needed to strengthen the evidence base and thus enable more robust recommendations.
The limitation of this study lies in the inability to complement the qualitative analysis (systematic review) with a quantitative analysis (meta-analysis), given the variety of measurement instruments, application techniques, and different time points at which the outcomes of interest were assessed. This level of heterogeneity affects, to some extent, the synthesis of the evidence and the clinical applicability of this review's results.
The strengths of the study include: an analysis and discussion of the clinical relevance of the outcome measures of interest. Additionally, it evaluates the isolated effect of manual therapy, unlike previous reviews in the field, where manual therapy was included as part of a multimodal treatment.
Conclusions
Based on the limited, heterogeneous evidence, which is at high risk of bias, it is not possible to confirm the therapeutic effect of manual therapy for plantar fasciitis. Although some trials suggest a moderate benefit of manual therapy in reducing pain, the available evidence is insufficient to draw definitive conclusions.
Given this, there is a need for more randomized controlled trials with greater methodological rigor, including more consistent, replicable protocols. This will allow for definitive conclusions regarding the contribution of this modality in the field of musculoskeletal rehabilitation.
