Editorial
← vista completaPublished on July 1, 2015 | http://doi.org/10.5867/medwave.2015.05.6167
Calling for qualitative health studies
Queremos publicar más estudios cualitativos en salud
Since the beginning of sociology and social sciences, the discipline has constantly perfected and sophisticated its research design on the topics and phenomena of interest, together with refining the data collection techniques. What is relatively novel in recent decades, is the inclusion of qualitative methods in the inquiry on problems relating to the health of individuals and populations [1]. The reason for this integration is that many, if not all, health problems are intricate and multifactorial. Positivistic methods make it possible to determine and quantify health problems, their distribution in populations, as well to establish correlation or causality of factors. The shortcoming, however, is that they do not necessarily provide a thorough understanding of people’s experiences, which are of interest to public health in all of its domains [2].
On the other hand, qualitative methods in health research provide insight into the complex forces that are present in public health, thus leading to better-informed health programs and policies [3],[4]. The result is more pertinent interventions for target populations by taking into account social, cultural and economic context and differences, which today we call social health determinants [5],[6].
Figures 1 and 2 show how qualitative methods in health research play out [3].
 Full size
Full size 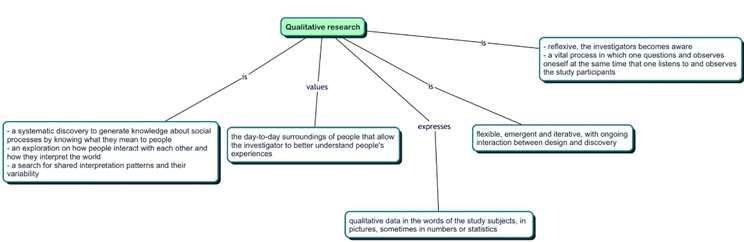 Full size
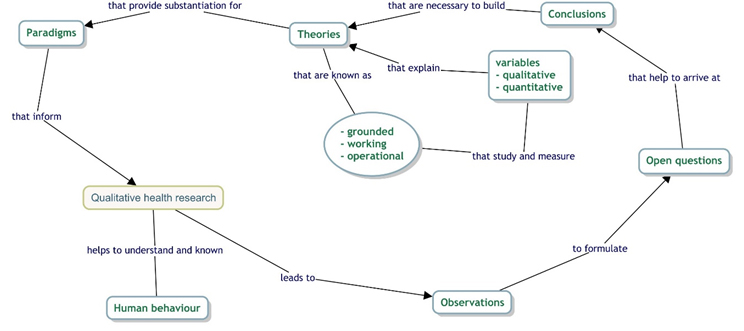
Full size Qualitative methods in health research lead to greater understanding and knowledge of human behavior as a result of observation that captures a greater wealth of elements. Thus we are able to more fully explain how people behave in healthcare settings, what happens in inter-professional work in health facilities, or the complex interactions of underserved social groups with their health systems, to name a few.
Field observations lead to questions that inform and structure qualitative studies that, in turn, are open to reformulating the data collection approach by introducing more open-ended questions that provide answers to the study questions. Study questions can always be changed as the study is conducted.
The above description is quite different from what we are used to in quantitative research. In the latter, once the study protocol has been approved, it must be strictly adhered to, otherwise putting at risk internal validity by exposing the design to systematic bias.
In contrast, in qualitative methods research the conclusions that we arrive at from field data collection will lead to ratification or disproval of theories, or to developing new theories that may explain the phenomenon of interest. When theories are constantly reformulated, as a result of the empirical understanding of social phenomena, it is possible to develop a more grounded grasp of what interests us, as issues arise from the systematic analysis of data. This is known as grounded theory.
There are several different methodologies used in qualitative research. Grounded theory is one of them. There are also action research, working theories, phenomenology, ethnomethodology, among others, all of which may be used before or after positivistic methods, thus resulting in mixed-methods research [7],[8]. Theories are used in qualitative research in order to develop the study questions because they offer complex conceptual frameworks that help to understand social phenomena underlying public health matters. Theories are useful, but we must not forget that they are only a prism through which we look at the reality that we are trying to study, which is one of the reasons why theories that are being used must be properly reported. This is known as reflexivity that can be defined as the act of communicating transparently the researcher’s own beliefs and how these beliefs may interact with study participants [9].
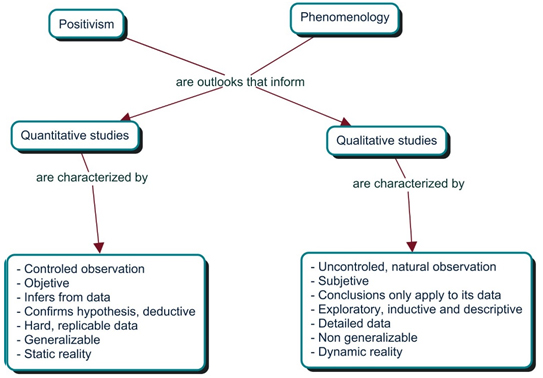
As we can see, the world of qualitative research is very different from the world of quantitative research [3]. Figure 3 shows some the differences in the way in which they approach reality. It is important to dwell on these differences because when we read or do critical analysis of a qualitative study we must know that the methods are very different. For example, in the quantitative perspective you must account for random error, for which you will choose as the best option a probabilistic sample when selecting your study participants. Instead, in qualitative research the sample will be comprised of subjects that show strong pertinence with the likelihood of collecting data. Pertinence is defined as having a high possibility of producing findings from participants aligned with the study’s objectives.
Furthermore, in quantitative research the study finalizes once all measurements are done on the predefined sample, while in quantitative methods the sample can be expanded during the research conduct until achieving “data saturation”, which occurs once new themes of interest stop emerging and answers to the study questions have been adequately provided. In other words, the subjects’ discourses will begin to repeat themselves and you begin to find repetitions, at which point the recruitment of subjects may be stopped [10]. The approach, as we can see, is very different [3].
 Full size
Full size In order to act on this need, the Journal has decided to create an explicit section called “qualitative studies”. We have also created a special checklist or evaluation form for submitted manuscripts that will help reviewers with their task. This critical analysis framework was developed from Trisha Greenhalgh’s book [11], Chapter 12, which refers to “papers that go beyond numbers” (12). The form questions are the following:
- The study describes an important clinical problem addressed via a clearly formulated question.
- The qualitative approach was appropriate.
- The manuscript adequately describes the setting (where the study population is found) and how the subjects were selected.
- The manuscript adequately describes the researcher’s perspective and it has been taken into account.
- What methods did the researcher use to analyse the data— and what quality control measures were implemented?
- The manuscript describes the methods that the researcher used for collecting data, and in enough detail (quality controls).
- The results are credible and, if so, they are clinically important.
- The manuscript clearly reports the study conclusions and these are justified by the results.
- The findings of the study are transferable to other settings.
So, to sum all this up, we warmly welcome your manuscript submissions of studies using qualitative methods in the study design (mixed-methods studies). Likewise, we call upon the investigators of the region to conduct research using the qualitative perspective as this will most certainly enhance our understanding of the social causes of health problems, among other benefits. The doors of our house are wide open to receive your submissions.
Notes
Conflicts of interest
The authors declare no conflicts of interest with the subject of the article.
