Reporte de caso
← vista completaPublicado el 4 de junio de 2026 | http://doi.org/10.5867/medwave.2026.05.3179
Niveles elevados persistentes de tiroglobulina que revelan un «Struma ovarii» en una paciente tratada por un carcinoma papilar de tiroides: reporte de caso
Persistent elevated thyroglobulin revealing Struma ovarii in a patient treated for papillary thyroid carcinoma: A case report
Introduction
Struma ovarii (SO) is a rare ovarian mature teratoma composed predominantly of thyroid tissue, accounting for <1% of all ovarian tumors and <5% of ovarian teratomas. Although typically benign, functional thyroid tissue in SO may cause thyrotoxicosis or interfere with surveillance of differentiated thyroid carcinoma due to ectopic thyroglobulin (Tg) production [1]. We report a case of persistent elevated serum thyroglobulin after total thyroidectomy and radioiodine ablation for papillary thyroid carcinoma (PTC), ultimately attributed to an incidental struma ovarii.
Case presentation
A 37-year-old woman with no relevant past medical history presented for evaluation of a newly detected thyroid nodule. She was euthyroid, and neck ultrasound (US) revealed a 1.9×1.3cm thyroid nodule located in the left lobe without suspicious cervical lymphadenopathy, and the fine-needle aspiration biopsy revealed a Bethesda V cytology. The patient underwent total thyroidectomy, and the histopathologic examination demonstrated a 1.8×1.4×1.2cm classic papillary thyroid carcinoma without aggressive features.
At 3-month follow-up, while receiving levothyroxine 125 mcg/day, she had a thyroid-stimulating hormone (TSH) of 2.5 µIU/mL, thyroglobulin of 18.9 ng/mL, undetectable anti-thyroglobulin antibodies and a negative neck ultra sound. After discussing with the patient the most appropriate management approach for her situation — including surveillance with neck ultra sound and serial thyroglobulin measurement, systemic evaluation with 131I whole-body scan (131I-WBS), and 18F-FDG PET/CT — the patient elected to undergo 18F-FDG PET/CT, which showed no evidence of locoregional or distant metastases, except for a 1.5 cm hypometabolic lesion in the left adnexa suggestive of mature teratoma. Upon evaluation by a multidisciplinary team of endocrinologists, radiologists, nuclear medicine physicians, and gynecologists, we concluded that, given its size and low SUV on 18F-FDG PET/CT, the ovarian lesion was amenable to imaging surveillance, independent of the thyroid cancer.
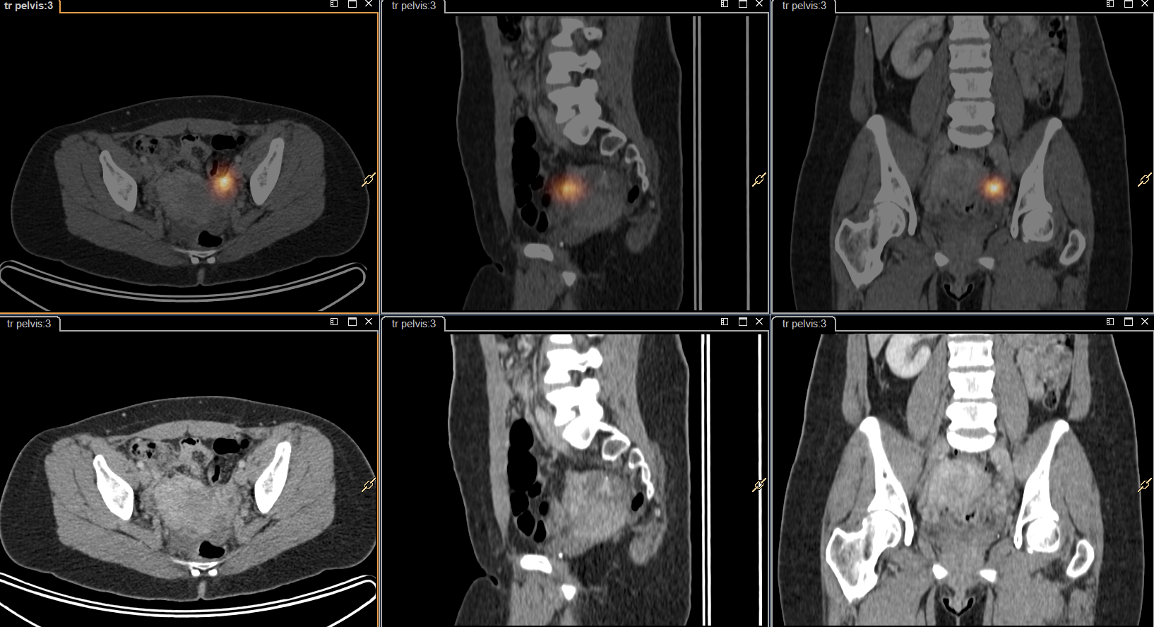
After preparation with recombinant human TSH (rhTSH), the patient underwent ablation with 30 mCi of radioactive iodine (RAI), and post-therapy whole-body SPECT/CT demonstrated focal radioactive iodine uptake in the thyroid bed and the left adnexal region (Figure 1). A transvaginal ultra sound confirmed a 1.3×1.3×1.1 cm left ovarian lesion suggestive of a teratoma. Therefore, a laparoscopic left oophorectomy was performed, and histological analysis established the diagnosis of SO (Figure 2). Two months after surgery, serum thyroglobulin was <0.1 ng/mL.
Post-(radio) iodine pelvic[131I] L- SPECT/CT scan shows intense (radio) iodine uptake in left adnexal tumor.
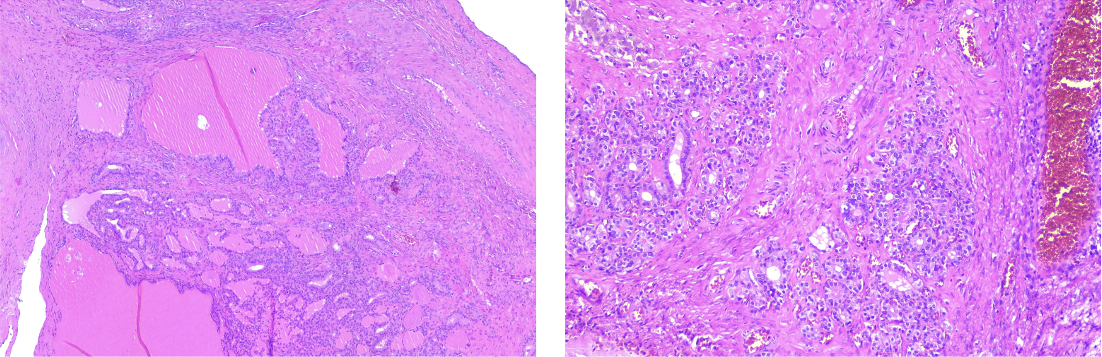
Histopathologic features of ovarian struma. Hematoxylin-eosin stain showing ovarian tissue with a multilocular cystic architecture, lined by a simple cuboidal epithelium containing colloid-like material, cholesterol crystals, and multinucleated giant cells.
Discussion
Persistent elevation of serum thyroglobulin after definitive treatment for differentiated thyroid carcinoma warrants evaluation for residual thyroid tissue or metastatic disease [2]. When standard imaging is unrevealing, ectopic thyroid tissue sources, though rare, must be considered. Struma ovarii, a monodermal teratoma variant, contains >50% thyroid tissue and may secrete thyroglobulin, mimicking residual thyroid carcinoma. Only isolated reports exist of elevated thyroglobulin leading to its diagnosis.
Imaging plays a pivotal role in localization. Struma ovarii is typically detected as a complex adnexal mass exhibiting solid and cystic components; 18FDG-PET/CT may reveal metabolic activity but lacks specificity. Radioactive iodine uptake in the ovarian region may represent benign struma ovarii, ovarian metastasis from papillary thyroid carcinoma, or a papillary thyroid carcinoma arising within a struma ovarii [3,4,5]. Surgical excision is both diagnostic and therapeutic. Histologically benign lesions are managed with oophorectomy alone, while malignant transformation (e.g. papillary thyroid carcinoma arising in struma ovarii) requires oncologic staging and potential adjuvant radioactive iodine therapy [6]. In this patient, benign ectopic thyroid tissue was responsible for biochemical persistence and resolved following resection, thereby avoiding unnecessary radioactive iodine retreatment or neck exploration.
The clinical presentation of struma ovarii in patients with differentiated thyroid cancer is heterogeneous, as the ectopic tissue does not always retain the capacity for both thyroglobulin production and 131I uptake [7,8]. While our patient presented with biochemical persistence (thyroglobulin: 18.9 ng/mL) that normalized post-resection, the literature reveals a broad spectrum: from cases with extreme thyroglobulin elevations reaching 2,315 ng/mL to instances described by Shim and Kim where intense 131I occurred despite low stimulated thyroglobulin levels (0.84 ng/mL) [3,4]. This variability implies that struma ovarii must remain a differential diagnosis for any unexplained thyroglobulin elevation or pelvic radiotracer accumulation, even when biochemical and scintigraphic findings appear discordant [9].
The diagnostic challenge is further complicated when the ectopic thyroid tissue undergoes atrophy or necrosis, often as a secondary effect of prior radioiodine therapy [7]. In such scenarios, typical follicular architecture may be poorly preserved or absent, making immunohistochemical (IHC) staining for thyroglobulin an essential tool for definitive confirmation [3,5,7]. As noted in previous reports, IHC staining can identify scattered thyroglobulin immunoreactivity along cystic walls or within atrophied follicles, even when standard hematoxylin-eosin staining is inconclusive [7]. Incorporating IHC evaluation not only reinforces the pathological diagnosis but also provides a clearer scientific basis for the "biochemical persistence" observed in cases where the morphological functionality of the tissue is limited [9].
In our case, the ovarian mass containing thyroid tissue was detected on the post-radioactive iodine whole-body scan. The elevated pre-ablation serum thyroglobulin suggested the presence of thyroid tissue, although it was unclear whether this represented metastatic disease or benign ectopic tissue. A marked decline in serum thyroglobulin following oophorectomy confirmed the ovarian tumor as its source.
Conclusion
In patients treated for papillary thyroid carcinoma, in the presence of unexplained elevated serum thyroglobulin, the existence of ectopic functional thyroid tissue such as struma ovarii should be included in the differential diagnosis. 18FDG-PET/CT imaging aids in detection beyond the cervical field. Surgical excision confirms diagnosis and normalizes biochemical markers. Awareness of this rare entity prevents misinterpretation of tumor marker dynamics and guides appropriate management.
