Epistemonikos summaries
← vista completaPublished on August 28, 2015 | http://doi.org/10.5867/medwave.2015.6233
What are the effects of hypertonic saline plus furosemide in acute heart failure?
¿Cuál es el efecto de la combinación de suero hipertónico y furosemida en la insuficiencia cardiaca aguda?
Abstract
In search of new therapies to solve diuretic resistance in acute heart failure, the addition of hypertonic saline has been proposed. Searching in Epistemonikos database, which is maintained by screening 30 databases, we identified two systematic reviews including nine pertinent randomized controlled trials. We combined the evidence and generated a summary of findings following the GRADE approach. We concluded hypertonic saline associated with furosemide probably decrease mortality, length of hospital stay and hospital readmission in patients with acute decompensated heart failure.
Problem
Volume depletion is the mainstay of treatment for acute heart failure, mainly with loop diuretics such as furosemide. However, some patients develop resistance to diuretics. Among the alternatives that have arisen as a potential solution to this clinical problem is the use of hypertonic saline. The increase in plasma osmolarity allows mobilization of extracellular fluid into intravascular. As baroceptors sense intravascular expansion, peripheral resistance decreases, improving ejection fraction, therefore increasing kidney and other organs blood flow, which improves response to diuretics. In addition, animal studies show hypertonic saline alone could improve myocardial contractility and reduce proinflammatory factors.
Methods
We used Epistemonikos database, which is maintained by screening more than 30 databases, to identify systematic reviews and their included primary studies. With this information we generated a structured summary using a pre-established format, which includes key messages, a summary of the body of evidence (presented as an evidence matrix in Epistemonikos), meta-analysis of the total of studies, a summary of findings table following the GRADE approach and a table of other considerations for decision-making.
|
Key messages
|
About the body of evidence for this question
|
What is the evidence. |
We found two systematic reviews [1],[2] including nine randomized controlled trials reported in 10 references [3],[4],[5],[6],[7],[8],[9],[10],[11],[12]. |
|
What types of patients were included |
All studies included patients with heart failure; six of them had reduced ejection fraction as inclusion criteria: three with <45% [4],[6],[7], three with <40% [8],[11],[12] and one with <35% [9],[10]. Three studies required patients were refractory to standard treatment [4],[7],[9],[10]. Seven studies restricted inclusion to patients with preserved renal function: three of them set creatinine limit in 2 mg/dl and without previous consumption of non-steroidal anti-inflammatories [4],[7],[9],[10]. |
|
What types of interventions were included |
Hypertonic saline in various concentrations, adjusted according sodium plasma level in five studies [4],[6],[8],[9],[10],[11], combined with intravenous furosemide in doses ranging from 250 to 2000 mg/day, administered either as bolus or continuous infusion. All studies compared with furosemide alone that was administered in the same way and dose as in the group intervened. |
|
What types of outcomes |
All-cause mortality, mortality from heart failure, need for hospitalization, length of hospital stay, change in New York Heart Association (NYHA) classification, renal function, cardiac markers, body weight. |
Summary of findings
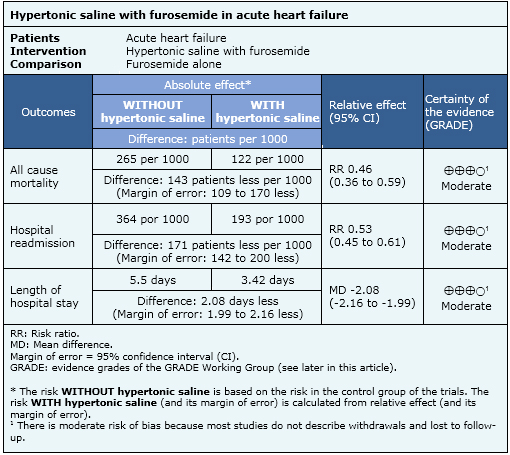
Information on the effects of adding hypertonic saline to the treatment with furosemide is based on nine randomized trials including 2566 patients. Only four studies reported overall mortality [4],[8],[10],[12], three studies reported readmissions [4],[8],[10], six studies reported length of hospital stay [4],[6],[7],[8],[10],[11] and seven studies reported change in creatinine serum level [3],[4],[6],[7],[8],[10],[12].
- Adding hypertonic saline to furosemide probably decreases mortality in patients with acute heart failure. The certainty of the evidence is moderate.
- Adding hypertonic saline to furosemide probably decreases length of hospital stay in patients with acute heart failure. The certainty of the evidence is moderate.
- Adding hypertonic saline to furosemide probably decreases hospital readmissions in patients with acute heart failure. The certainty of the evidence is moderate.

Other considerations for decision-making
|
To whom this evidence does and does not apply |
|
| About the outcomes included in this summary |
| Balance between benefits and risks, and certainty of the evidence |
|
| Resource considerations |
|
|
Differences between this summary and other sources |
|
| Could this evidence change in the future? |
|
How we conducted this summary
Using automated and collaborative means, we compiled all the relevant evidence for the question of interest and we present it as a matrix of evidence.
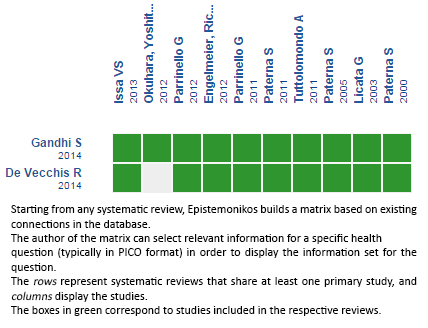 Full size
Full size Follow the link to access the interactive version: Hypertonic saline plus furosemide for acute heart failure
Notes
The upper portion of the matrix of evidence will display a warning of “new evidence” if new systematic reviews are published after the publication of this summary. Even though the project considers the periodical update of these summaries, users are invited to comment in Medwave or to contact the authors through email if they find new evidence and the summary should be updated earlier. After creating an account in Epistemonikos, users will be able to save the matrixes and to receive automated notifications any time new evidence potentially relevant for the question appears.
The details about the methods used to produce these summaries are described here http://dx.doi.org/10.5867/medwave.2014.06.5997.
Epistemonikos foundation is a non-for-profit organization aiming to bring information closer to health decision-makers with technology. Its main development is Epistemonikos database (www.epistemonikos.org).
These summaries follow a rigorous process of internal peer review.
Conflicts of interest
The authors do not have relevant interests to declare.
