Epistemonikos summaries
← vista completaPublished on November 21, 2015 | http://doi.org/10.5867/medwave.2015.6320
Low molecular weight heparin in one or two doses for the initial treatment of venous thromboembolic disease?
¿Una o dos dosis diarias de heparina de bajo peso molecular para el tratamiento de la enfermedad tromboembólica?
Abstract
The preferred dosification for low molecular weight heparins is in two doses for most patients with venous thromboembolic disease. A daily dose would make treatment simpler, less expensive and more comfortable while retaining a similar benefit and safety. Searching in Epistemonikos database, which is maintained by screening 30 databases, we identified two systematic reviews including five randomized trials. We combined the evidence using meta-analysis and generated a summary of findings table following the GRADE approach. We concluded it is not clear whether the risk of recurrence differs between the two alternatives because the certainty of the evidence is very low, and that administering low molecular weight heparin in two doses might be associated to little or no difference in the risk of major bleeding and mortality.
Problem
There is wide consensus that low molecular weight heparins are part of the standard treatment for many patients with venous thromboembolic disease. Traditionally they are administered twice daily. However, a single daily dose could increase patient’s comfort, reduce costs and facilitate ambulatory treatment. However, it is not clear if this dosification has a similar benefit and safety profile.
Methods
We used Epistemonikos database, which is maintained by screening more than 30 databases, to identify systematic reviews and their included primary studies. With this information we generated a structured summary using a pre-established format, which includes key messages, a summary of the body of evidence (presented as an evidence matrix in Epistemonikos), meta-analysis of the total of studies, a summary of findings table following the GRADE approach and a table of other considerations for decision-making.
|
Key messages
|
About the body of evidence for this question
| What is the evidence. See evidence matrix in Epistemonikos later |
We found two systematic reviews [1],[2] including five randomized controlled trials overall [3],[4],[5],[6],[7]. |
| What types of patients were included |
Patients with confirmed thromboembolic event: deep vein thrombosis and/or pulmonary embolism. Four studies included patients with deep vein thrombosis and one [5] included patients with pulmonary embolism or deep vein thrombosis. |
| What types of interventions were included |
All of the studies compared subcutaneous low molecular weight heparin administered once versus twice daily. Two studies used dalteparin [4],[6], one enoxaparin [5], one nadroparin [3] and one logiparin [7]. Four studies used the same daily dose in both arms and one [5] used 75% of the total dose in the once daily dose arm. |
| What types of outcomes were measured |
Symptomatic recurrence, major bleeding (intracranial, retroperitoneal, requiring transfusion, surgery or anticoagulant withdrawal, or as cause of death) during and 48 hours after treatment; total bleeding episodes; global mortality and cause-specific mortality (recurrence, bleeding); clot size increase in venography. |
Summary of findings
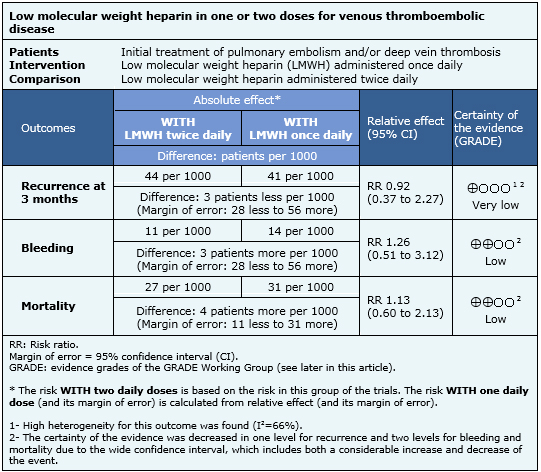
The information is based on five randomized studies which included 1508 patients. Four studies reported all-cause mortality, three studies reported symptomatic recurrence at 3 months of follow up and five studies presented information on major bleeding during treatment with low molecular weight heparin.
- It is not clear whether a daily dose of low molecular weight heparin modifies the risk of recurrence compared with two daily doses because the certainty of the evidence is very low.
- One daily dose of low molecular weight heparin could result in little or minimal increase in the risk of major bleeding. The certainty of the evidence is low.
- One daily dose of low molecular weight heparin might not increase mortality. The certainty of the evidence is low.
Other considerations for decision-making
|
To whom this evidence does and does not apply |
|
| About the outcomes included in this summary |
| Balance between benefits and risks, and certainty of the evidence |
|
| What would patients and their doctors think about this intervention |
|
| Resource considerations |
|
|
Differences between this summary and other sources |
|
| Could this evidence change in the future? |
|
How we conducted this summary
Using automated and collaborative means, we compiled all the relevant evidence for the question of interest and we present it as a matrix of evidence.
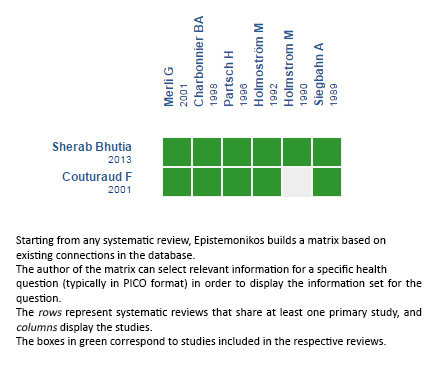
Follow the link to access the interactive version: Low molecular weight heparin administered once versus twice daily for venous thromboembolism
Notes
The upper portion of the matrix of evidence will display a warning of “new evidence” if new systematic reviews are published after the publication of this summary. Even though the project considers the periodical update of these summaries, users are invited to comment in Medwave or to contact the authors through email if they find new evidence and the summary should be updated earlier. After creating an account in Epistemonikos, users will be able to save the matrixes and to receive automated notifications any time new evidence potentially relevant for the question appears.
The details about the methods used to produce these summaries are described here http://dx.doi.org/10.5867/medwave.2014.06.5997.
Epistemonikos foundation is a non-for-profit organization aiming to bring information closer to health decision-makers with technology. Its main development is Epistemonikos database (www.epistemonikos.org).
These summaries follow a rigorous process of internal peer review.
Conflicts of interest
The authors do not have relevant interests to declare.
