Resúmenes Epistemonikos
← vista completaPublicado el 15 de noviembre de 2016 | http://doi.org/10.5867/medwave.2016.6602
¿Cuándo debe iniciarse la diálisis crónica en pacientes con insuficiencia renal terminal?
At which stage of end-stage kidney disease should chronic dialysis be started?
Abstract
The number of patients requiring renal replacement therapy has increased exponentially in recent years. However, there is still controversy regarding the best moment to initiate chronic dialysis. Searching in Epistemonikos database, which is maintained by screening 30 databases, we identified five systematic reviews comprising 21 trials addressing the question of this article. We combined the evidence using meta-analysis and generated a summary of findings following the GRADE approach. We concluded delaying the initiation of dialysis probably does not increase mortality risk in chronic kidney disease and makes little or no difference in the risk of requiring a temporary catheter or having to check the vascular access.
Problem
Since the onset of renal replacement therapy, both peritoneal dialysis and hemodialysis have experienced an exponential growth.
Traditionally, early initiation of dialysis has been proposed in order to avoid patient's general condition deterioration, especially nutritional status. However, dialysis carries a high-cost, and leads to complications and risks, so there are also arguments for delaying its initiation.
Methods
We used Epistemonikos database, which is maintained by screening more than 30 databases, to identify systematic reviews and their included primary studies. With this information, we generated a structured summary using a pre-established format, which includes key messages, a summary of the body of evidence (presented as an evidence matrix in Epistemonikos), meta-analysis of the total of studies, a summary of findings table following the GRADE approach and a table of other considerations for decision-making.
|
Key messages
|
About the body of evidence for this question
|
What is the evidence. |
We found five systematic reviews [1],[2],[3],[4],[5] including 21 studies reported in 23 references [6],[7],[8], [9],[10],[11],[12],[13], [14],[15],[16],[17],[18],[19],[20], [21],[22],[23],[24],[25],[26],[27],[28]. Of these, only one study corresponds to a randomized controlled trial, reported in three references [10],[11],[14]. This table and the summary in general are based on the latter because observational studies did not increase the certainty of the evidence, or provide additional relevant information. |
|
What types of patients were included |
The characteristics of participants enrolled in the randomized trial [10] are:
|
|
What types of interventions were included |
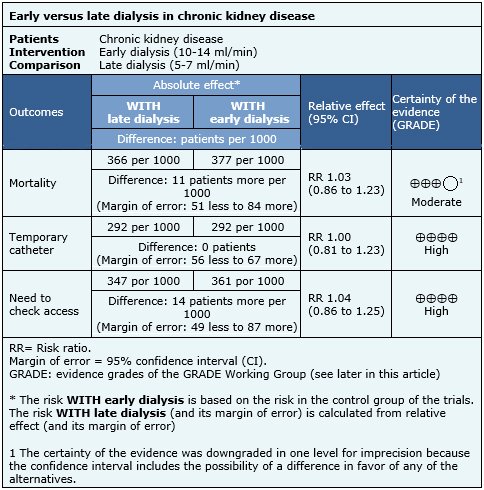
The randomized trial [10] defined early dialysis as GFR 10-14 ml/min and late dialysis as GFR 5-7 ml/min. |
|
What types of outcomes |
The outcomes were pooled by the different systematic reviews as follows:
|
Summary of findings
The information about the timing of initiation of dialysis is based on one randomized trial [10] including 828 patients. The inclusion of observational studies did not increase the certainty of the evidence.
The summary of findings is the following:
- Delaying initiation of dialysis probably does not increase mortality in chronic kidney disease. The certainty of the evidence is moderate.
- The timing of initiation of dialysis makes little or no difference in the risk of requiring a temporary catheter. The certainty of the evidence is high.
- Early initiation of dialysis makes little or no difference in the risk of having to check the vascular access. The certainty of the evidence is high.

Other considerations for decision-making
|
To whom this evidence does and does not apply |
|
| About the outcomes included in this summary |
|
| Balance between benefits and risks, and certainty of the evidence |
|
| What would patients and their doctors think about this intervention |
|
| Resource considerations |
|
| Feasibility and implementation |
|
| Differences between this summary and other sources |
|
| Could this evidence change in the future? |
|
How we conducted this summary
Using automated and collaborative means, we compiled all the relevant evidence for the question of interest and we present it as a matrix of evidence.
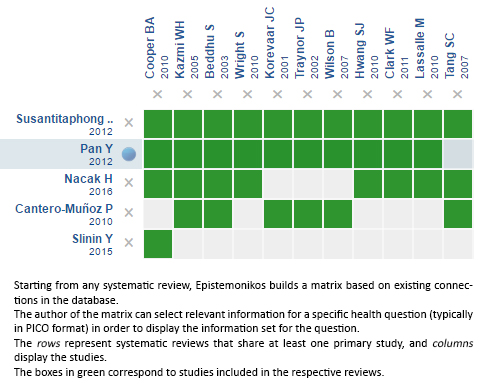
Follow the link to access the interactive version: Early versus late initiation of dialysis in end-stage renal failure
Notes
The upper portion of the matrix of evidence will display a warning of “new evidence” if new systematic reviews are published after the publication of this summary. Even though the project considers the periodical update of these summaries, users are invited to comment in Medwave or to contact the authors through email if they find new evidence and the summary should be updated earlier. After creating an account in Epistemonikos, users will be able to save the matrixes and to receive automated notifications any time new evidence potentially relevant for the question appears.
The details about the methods used to produce these summaries are described here http://dx.doi.org/10.5867/medwave.2014.06.5997.
Epistemonikos foundation is a non-for-profit organization aiming to bring information closer to health decision-makers with technology. Its main development is Epistemonikos database (www.epistemonikos.org).
These summaries follow a rigorous process of internal peer review.
Conflicts of interest
The authors do not have relevant interests to declare.
