Epistemonikos summaries
← vista completaPublished on November 23, 2016 | http://doi.org/10.5867/medwave.2016.6607
Are erythropoiesis-stimulating agents beneficial for anemia in chronic heart failure patients?
¿Son beneficiosos los agentes estimulantes de la eritropoyesis en pacientes anémicos con insuficiencia cardiaca?
Abstract
Anemia is a common comorbidity among patients with chronic health failure and appears to be associated with increased mortality and morbidity. However, it is unclear whether correcting it with erythropoiesis stimulating agents improves clinical outcomes. Searching in Epistemonikos database, which is maintained by screening 30 databases, we identified 11 systematic reviews including 17 trials overall addressing the question of this article. We combined the evidence using meta-analysis and generated a summary of findings following the GRADE approach. We concluded the use of erythropoiesis stimulating agents in patients with chronic heart failure and anemia does not decrease mortality, and it is not clear if they decrease the risk of hospitalization or if they improve functional status because the certainty of the evidence is very low. The risk of thromboembolic events probably increases.
Problem
Anemia is a common comorbidity among patients with chronic heart failure. Multiple mechanisms may contribute to anemia, including hemodilution, activation of pro-inflammatory cytokines, chronic kidney disease and impaired erythropoiesis. Anemia in people with chronic heart failure is associated with a higher risk of hospitalization, increased mortality, and poor functional status [1].
Erythropoiesis-stimulating agents, such as the two forms of recombinant human erythropoietin (epoetin-alfa and epoetin-beta) and its analogue darbepoetin alfa, share the same mechanism of endogenous erythropoietin, and are the first-line treatment for non-iron-deficiency anemia in patients with cancer or chronic kidney disease. However, its use has been associated with increased thromboembolic events, hypertension and mortality when high hemoglobin targets are used. There is controversy about their role in patients with heart failure and anemia.
Methods
We used Epistemonikos database, which is maintained by screening more than 30 databases, to identify systematic reviews and their included primary studies. With this information we generated a structured summary using a pre-established format, which includes key messages, a summary of the body of evidence (presented as an evidence matrix in Epistemonikos), meta-analysis of the total of studies, a summary of findings table following the GRADE approach and a table of other considerations for decision-making.
|
Key messages
|
About the body of evidence for this question
|
What is the evidence. |
We found 11 systematic reviews [1],[2],[3],[4],[5],[6],[7],[8],[9],[10],[11] including 17 randomized controlled trials overall, reported in 18 references [12],[13],[14],[15],[16],[17],[18],[19],[20],[21], [22],[23], [24], [25], [26], [27],[28], [29]. One trial was reported in two articles [15], [16]. |
|
What types of patients were included |
All of the trials included chronic heart failure patients with representation of all etiologies. All of the trials included patients with symptomatic chronic heart failure and anemia. Regarding NYHA functional class, three trials included NYHA I [14],[26],[29] eight included NYHA II [12],[14],[15],[23],[24],[26],[28],[29], all included NYHA III, 13 trials included NYHA IV [12],[13],[14],[17],[18],[19],[20],[21],[22],[23],[27],[28],[29], and one trial did not report NYHA functional class [25] . Most trials included participants with low ejection fraction (<40%), with the exception of two trials; one reported a mean ejection fraction of 58% [18], and the other did not report this variable [25]. Different hemoglobin levels were used to define anemia among the trials. Two of them considered hemoglobin level < 11g/dl [20],[25], four <11.5 g/dl [21],[22],[23],[27], six <12 g/dl [13],[14],[18],[26],[28],[29], four < 12.5 g/dl [12],[15],[23], [24] and one defined anemia by hematocrit <35% [17]. |
|
What types of interventions were included |
Eight trials used alfa or beta recombinant human erythropoietin [13],[17],[18],[19],[20],[21],[22],[27],), and nine used darbepoetin alfa [12],[14],[15],[23],[24],[25],[26],[28],[29]. Most trials compared against placebo, with the exception of two that compared against no treatment [13],[27]. All trials except three [12],[13],[25] associated iron supplementation to the treatment. Regarding hemoglobin targets, one trial considered a target > 11.5 g/dl [20], one >12 g/dl [22], two >12.5 g/dl [15],[27], five >13 g/dl [14],[25],[26],[28],[29], one >14 g/dl [24], one considered a hematocrit target > 45% [17], and six did not report a target [12],[13],[18],[19],[21],[23]. |
|
What types of outcomes |
The different systematic reviews grouped the outcomes as follows: All-cause mortality, all-cause hospitalization, exercise tolerance, hemoglobin level, quality of life (measured in KCCQ, MLHFQ and PGA scales), NYHA functional class, B-type natriuretic peptide levels, left ventricular ejection fraction, total thromboembolic events, myocardial infarction, deep vein thrombosis, ischemic stroke, pulmonary embolism. |
Summary of findings
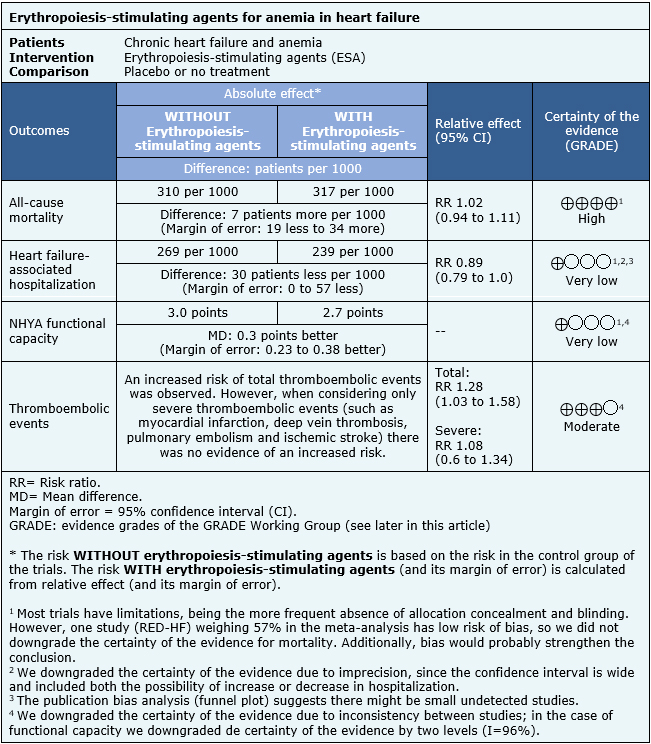
The information on the effects of erythropoiesis-stimulating agents is based on 17 randomized trials including 4617 patients. Sixteen trials reported mortality (4587 patients) [12],[14],[15],[17],[18],[19],[20],[21],[22],[23],[24],[25],[26],[27],[28],[29]. Fourteen trials reported hospitalizations by any cause (3210 patients) [12],[14],[15],[17],[18],[19],[20],[21],[22],[24],[26],[27],[28],[29], and 11 trials reported NYHA functional capacity (857 patients) [13],[14],[19],[20],[21],[22],[23],[24],[25],[26],[27],[29]. Data from thromboembolic events were reported in a way that precluded meta-analysis, therefore we present data from one review [4].
The summary of findings is the following:
- The use of erythropoiesis stimulating agents in patients with chronic heart failure and anemia does not decrease mortality. The certainty of the evidence is high.
- It is not clear whether erythropoiesis-stimulating agents decrease hospitalization in patients with chronic heart failure and anemia because the certainty of the evidence is very low.
- It is not clear whether erythropoiesis-stimulating agents improve functional status in patients with chronic heart failure and anemia because the certainty of the evidence is very low.
- The use of erythropoiesis stimulating agents in patients with chronic heart failure and anemia probably increases the risk of total thromboembolic events. The certainty of the evidence is moderate.

Other considerations for decision-making
|
To whom this evidence does and does not apply |
|
| About the outcomes included in this summary |
|
| Balance between benefits and risks, and certainty of the evidence |
|
| What would patients and their doctors think about this intervention |
|
| Resource considerations |
|
|
Differences between this summary and other sources |
|
| Could this evidence change in the future? |
|
How we conducted this summary
Using automated and collaborative means, we compiled all the relevant evidence for the question of interest and we present it as a matrix of evidence.
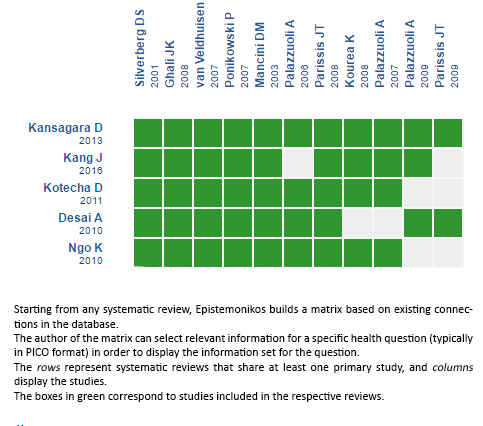
Follow the link to access the interactive version: Erythropoiesis-stimulating agents for anemia in chronic heart failure
Notes
The upper portion of the matrix of evidence will display a warning of “new evidence” if new systematic reviews are published after the publication of this summary. Even though the project considers the periodical update of these summaries, users are invited to comment in Medwave or to contact the authors through email if they find new evidence and the summary should be updated earlier. After creating an account in Epistemonikos, users will be able to save the matrixes and to receive automated notifications any time new evidence potentially relevant for the question appears.
The details about the methods used to produce these summaries are described here http://dx.doi.org/10.5867/medwave.2014.06.5997.
Epistemonikos foundation is a non-for-profit organization aiming to bring information closer to health decision-makers with technology. Its main development is Epistemonikos database (www.epistemonikos.org).
These summaries follow a rigorous process of internal peer review.
Conflicts of interest
The authors do not have relevant interests to declare.
