Epistemonikos summaries
← vista completaPublished on October 31, 2017 | http://doi.org/10.5867/medwave.2017.08.7068
Is betahistine effective for Ménière’s disease?
¿Es efectiva la betahistina en la enfermedad de Ménière?
Abstract
PROBLEM Meniere’s disease is an inner ear disorder characterized by episodes of spontaneous vertigo, fluctuating hearing loss and tinnitus. Betahistine has been used to reduce intensity and frecuency of vertigo attacks, but there is controversy regarding its effectiveness.
METHODS To answer this question we used Epistemonikos, the largest database of systematic reviews in health, which is maintained by screening multiple information sources, including MEDLINE, EMBASE, Cochrane, among others. We extracted data from the systematic reviews, reanalyzed data of primary studies, conducted a meta-analysis and generated a summary of findings table using the GRADE approach.
RESULTS AND CONCLUSIONS We identified four systematic reviews including 12 trials overall. We concluded betahistine might reduce the number of attacks, vertigo intensity and lead to a symptomatic improvement according to global judgement in patients with Meniere’s disease, but the certainty of evidence is low. On the other hand, it probably does not have significant adverse effects.
Problem
Ménière’s disease is an inner ear disorder characterized by episodes of spontaneous vertigo, fluctuating hearing loss and tinnitus. One of the most used diagnostic criteria, although not universally accepted, includes the presence of two vertigo episodes with a duration grater than 20 minutes, audiometric confirmation of sensorineural hearing loss, plus tinnitus or aural fullness perception [1].
Ménière’s disease is caused by an increase in endolymphatic pressure in the inner ear, from unknown etiology. This leads to recurrent and frequent vertigo attacks with substantive impact on quality of life, followed by periods of remission that can last several months [2].
Betahistine has long been used to reduce intensity and frecuency of vertigo attacks and tinnitus, since it would delay progression of hearing loss in Ménière’s disease. The alleged mechanism is endolymph pressure reduction secondary to microcirculation improvement at the stria vascularis of the cochlea. Another proposed mechanism relates to vestibular nucleus activity inhibition. However, there is controversy regarding its effectiveness.
Methods
To answer the question, we used Epistemonikos, the largest database of systematic reviews in health, which is maintained by screening multiple information sources, including MEDLINE, EMBASE, Cochrane, among others, to identify systematic reviews and their included primary studies. We extracted data from the identified reviews and reanalyzed data from primary studies included in those reviews. With this information, we generated a structured summary denominated FRISBEE (Friendly Summary of Body of Evidence using Epistemonikos) using a pre-established format, which includes key messages, a summary of the body of evidence (presented as an evidence matrix in Epistemonikos), meta-analysis of the total of studies when it is possible, a summary of findings table following the GRADE approach and a table of other considerations for decision-making.
|
Key messages
|
About the body of evidence for this question
|
What is the evidence. |
We found four systematic reviews [3],[4],[5],[6] including 12 primary studies relevant for our question [7],[8],[9],[10],[11],[12],[13],[14],[15],[16],[17],[18], all of them randomized controlled trials. |
|
What types of patients were included* |
Some trials did not use the American Academy of Otolaryngology –Head and Neck Surgery guidelines’ criteria for Ménière’s disease [1]. In consequence, some systematic reviews did not include them into their analysis. In order to present direct evidence, these are presented in this table, but were not used to estimate the effect of benefits in the summary of findings table. Six trials specified the inclusion of patients with clinical Ménière’s disease [8],[10],[11],[12],[14],[17]. One of the trials included patients with progressive episodic vertigo [9], two included patients with two or three months of peripheral vertigo [7],[13] and one with recurrent vertigo defined as two or more vertigo attacks in the last month [15]. Two trials did not specify the inclusion criteria [16],[18]. |
|
What types of interventions were included* |
All trials compared betahistine against placebo. |
|
What types of outcomes |
Outcomes, according to how they were grouped in the identified systematic reviews were:
|
* The information about primary studies is extracted from the systematic reviews identified, unless otherwise specified.
Summary of findings
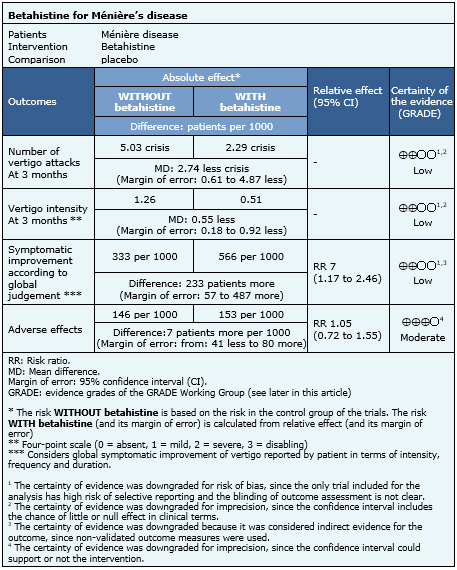
The information about the effects of betahistine on Ménière’s disease is based on 12 randomized trials. Only six trials included patients with clinical disease [8],[10],[11],[12],[14],[17] including 327 patients. Only one trial reported the number of vertigo attacks and intensity of symptoms [17] and three trials measured improvement according to global judgement of patients. Adverse effects were assessed in seven trials [7],[8],[10],[11],[13],[14],[17].
- Betahistine might reduce the number of vertigo attacks in patients with Ménière’s disease. The certainty of the evidence is low.
- Betahistine might reduce the intensity of vertigo in patients with Ménière’s disease. The certainty of the evidence is low.
- Betahistine might lead to symptomatic improvement according to global judgement of patients with Ménière’s disease. The certainty of the evidence is low.
- Betahistine probably does not have important adverse effects in patients with Ménière’s disease. The certainty of the evidence is moderate.

Other considerations for decision-making
|
To whom this evidence does and does not apply |
|
| About the outcomes included in this summary |
|
| Balance between benefits and risks, and certainty of the evidence |
|
| Resource considerations |
|
| What would patients and their doctors think about this intervention |
|
|
Differences between this summary and other sources |
|
| Could this evidence change in the future? |
|
How we conducted this summary
Using automated and collaborative means, we compiled all the relevant evidence for the question of interest and we present it as a matrix of evidence.
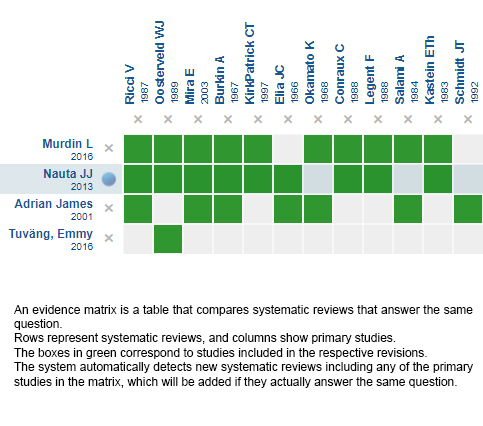
Follow the link to access the interactive version: Betahistine for Ménière's disease
Notes
The upper portion of the matrix of evidence will display a warning of “new evidence” if new systematic reviews are published after the publication of this summary. Even though the project considers the periodical update of these summaries, users are invited to comment in Medwave or to contact the authors through email if they find new evidence and the summary should be updated earlier.
After creating an account in Epistemonikos, users will be able to save the matrixes and to receive automated notifications any time new evidence potentially relevant for the question appears.
This article is part of the Epistemonikos Evidence Synthesis project. It is elaborated with a pre-established methodology, following rigorous methodological standards and internal peer review process. Each of these articles corresponds to a summary, denominated FRISBEE (Friendly Summary of Body of Evidence using Epistemonikos), whose main objective is to synthesize the body of evidence for a specific question, with a friendly format to clinical professionals. Its main resources are based on the evidence matrix of Epistemonikos and analysis of results using GRADE methodology. Further details of the methods for developing this FRISBEE are described here (http://dx.doi.org/10.5867/medwave.2014.06.5997)
Epistemonikos foundation is a non-for-profit organization aiming to bring information closer to health decision-makers with technology. Its main development is Epistemonikos database (www.epistemonikos.org).
Potential conflicts of interest
The authors do not have relevant interests to declare.
