Resúmenes Epistemonikos
← vista completaPublicado el 27 de diciembre de 2017 | http://doi.org/10.5867/medwave.2017.09.7117
¿Es efectiva la profilaxis pre-exposición para prevenir infección por VIH en hombres que tienen sexo con hombres?
Is pre-exposure prophylaxis effective for preventing HIV infection in men who have sex with men?
Abstract
INTRODUCTION Increasing rates of HIV infection remain of concern, especially for high-risk groups such as men who have sex with men. Oral pre-exposure prophylaxis has emerged as an alternative to prevention. However, doubts persist in patients and physicians about its effectiveness.
METHODS To answer this question we used Epistemonikos, the largest database of systematic reviews in health, which is maintained by screening multiple information sources, including MEDLINE, EMBASE, Cochrane, among others. We extracted data from the systematic reviews, reanalyzed data of primary studies, conducted a meta-analysis and generated a summary of findings table using the GRADE approach.
RESULTS AND CONCLUSIONS We identified six systematic reviews including twelve studies overall, of which six were randomized trials. We concluded the use of oral pre-exposure prophylaxis reduces the probability of HIV infection in men who have sex with men, has few or no adverse effects, and is a measure with a good balance between benefits, risks and costs.
Problem
Despite increased community awareness, HIV infection rates continue to rise. One of the high-risk group is men who have sex with men, so better prevention strategies are required. The use of antiretroviral drugs in uninfected individuals, or pre-exposure prophylaxis (PrEP), has emerged as a promising tool for prevention in individuals at high risk of HIV infection. The most commonly used combination of PrEP has been oral emtricitabine with tenofovir disoproxil fumarate, and to a lesser extent tenofovir disoproxil fumarate alone. Despite the approval of the first as PrEP by the FDA in 2012, physicians and patients still question the effectiveness and safety of this measure.
Methods
To answer the question, we used Epistemonikos, the largest database of systematic reviews in health, which is maintained by screening multiple information sources, including MEDLINE, EMBASE, Cochrane, among others, to identify systematic reviews and their included primary studies. We extracted data from the identified reviews and reanalyzed data from primary studies included in those reviews. With this information, we generated a structured summary denominated FRISBEE (Friendly Summary of Body of Evidence using Epistemonikos) using a pre-established format, which includes key messages, a summary of the body of evidence (presented as an evidence matrix in Epistemonikos), meta-analysis of the total of studies when it is possible, a summary of findings table following the GRADE approach and a table of other considerations for decision-making.
|
Key messages
|
About the body of evidence for this question
|
What is the evidence. |
We found six systematic reviews [1],[2],[3],[4],[5],[6] |
|
What types of patients were included* |
The patients included in the trials were HIV uninfected men who have sex with men, over 18 years of age, and considered at high risk of HIV infection (due to a history of high number of sexual partners, sexual intercourse without condom use, sex with people with sexually transmitted diseases, or sex in exchange for money). |
|
What types of interventions were included* |
All trials evaluated the use of oral PrEP in conjunction with standard prevention (including education and provision of condoms). Five evaluated the use of emtricitabine/tenofovir [11],[14],[20],[23],[29] and one the use of tenofovir alone [25]. Five trials evaluated against placebo [11],[14],[23],[25],[29] and three against a non-treatment group [14],[20],[25]. Five used PrEP on a daily basis [11],[14],[20],[25],[29] and one intermittently, before and after having sex [23]. One trial used behavioral therapy as a co-intervention [14] and one trial was pragmatic and open-label [20]. One trial included a small group of women [29], but since the vast majority of the participants were men who had sex with men, it was included in the analysis. |
|
What types of outcomes |
The main outcomes analyzed were the rate of HIV infection and adverse effects. Qualitatively analyzed outcomes included changes in risk behaviors, mainly condom use objectified by interviews [14],[25] or indirectly by incidence of other sexually transmitted diseases [20]. The average follow-up of the trials was 15 months, with a range between 4 and 33 months. |
* The information about primary studies is extracted from the systematic reviews identified, unless otherwise specified.
Summary of Findings
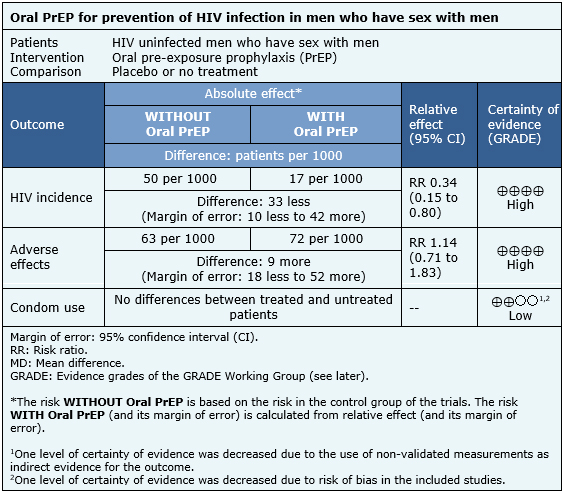
The information on the effects of oral PrEP in men who have sex with men is based on six trials [11],[14],[20],[23],[25],[29] which included 3974 patients.
It was not possible to extract enough information from the reviews identified to reconstruct the meta-analysis of HIV incidence. Therefore, the information presented is based on the results of the meta-analysis of a systematic review [1] that is based on four trials [11],[23],[25],[29] that included 3371 patients.
The information on adverse events is based on three trials [11],[14],[25] whose data were reusable from systematic reviews and included 2957 patients. The information on changes in condom use is based on three trials [14],[20],[25] that compared against no treatment, whose data were described qualitatively in the systematic reviews and included 1003 patients.
The summary of findings is as follows:
- Pre-exposure prophylaxis reduces HIV infection in men who have sex with men. The certainty of the evidence is high.
- Pre-exposure prophylaxis reduces leads to minimal or no increase in adverse effects. The certainty of the evidence is high.
- Pre-exposure prophylaxis might result in little or no difference in terms of condom use in men who have sex with men. The certainty of the evidence is low.
| Follow the link to access the interactive version of this table (Interactive Summary of Findings - iSoF) |

Other considerations for decision-making
|
To whom this evidence does and does not apply |
|
| About the outcomes included in this summary |
|
| Balance between benefits and risks, and certainty of the evidence |
|
| Resource considerations |
|
| What would patients and their doctors think about this intervention |
|
|
Differences between this summary and other sources |
|
| Could this evidence change in the future? |
|
How we conducted this summary
Using automated and collaborative means, we compiled all the relevant evidence for the question of interest and we present it as a matrix of evidence.
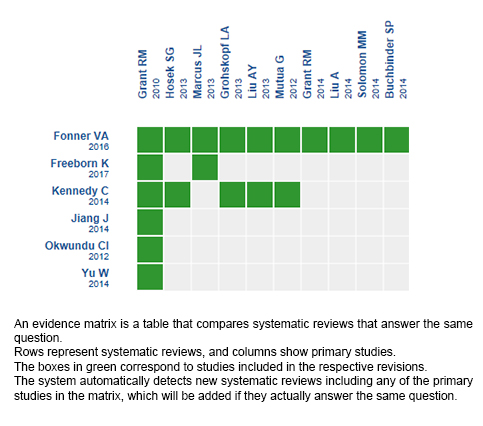
Follow the link to access the interactive version: Oral PrEP for prevention of HIV infection in men who have sex with men
Notes
The upper portion of the matrix of evidence will display a warning of “new evidence” if new systematic reviews are published after the publication of this summary. Even though the project considers the periodical update of these summaries, users are invited to comment in Medwave or to contact the authors through email if they find new evidence and the summary should be updated earlier.
After creating an account in Epistemonikos, users will be able to save the matrixes and to receive automated notifications any time new evidence potentially relevant for the question appears.
This article is part of the Epistemonikos Evidence Synthesis project. It is elaborated with a pre-established methodology, following rigorous methodological standards and internal peer review process. Each of these articles corresponds to a summary, denominated FRISBEE (Friendly Summary of Body of Evidence using Epistemonikos), whose main objective is to synthesize the body of evidence for a specific question, with a friendly format to clinical professionals. Its main resources are based on the evidence matrix of Epistemonikos and analysis of results using GRADE methodology. Further details of the methods for developing this FRISBEE are described here (http://dx.doi.org/10.5867/medwave.2014.06.5997)
Epistemonikos foundation is a non-for-profit organization aiming to bring information closer to health decision-makers with technology. Its main development is Epistemonikos database (www.epistemonikos.org).
Potential conflicts of interest
The authors do not have relevant interests to declare.
