Epistemonikos summaries
← vista completaPublished on December 28, 2017 | http://doi.org/10.5867/medwave.2017.09.7124
Is wrist splint more effective than forearm band for lateral epicondylitis?
¿Es el uso de muñequera más efectivo que el uso de banda de antebrazo en la epicondilitis lateral?
Abstract
INTRODUCTION Lateral epicondylitis is a common cause of lateral elbow pain. There are many treatments able to improvement symptoms, including orthotic devices. The main available orthosis are wrist splint and forearm band. However, it is not clear which one constitutes the best alternative for symptomatic treatment.
METHODS To answer this question we used Epistemonikos, the largest database of systematic reviews in health, which is maintained by screening multiple information sources, including MEDLINE, EMBASE, Cochrane, among others. We extracted data from the systematic reviews, reanalyzed data of primary studies, conducted a meta-analysis and generated a summary of findings table using the GRADE approach.
RESULTS AND CONCLUSIONS We identified three systematic reviews including four studies overall, all of them randomized trials. With this evidence, we concluded there might be no difference in global measure of improvement and pain free grip strength between the forearm band and wrist splint, and it is not clear whether using a wrist splint decreases pain in comparison with a forearm band, because the certainty of the evidence is very low.
Problem
Lateral epicondylitis is a degenerative condition of the lateral epicondyle of the elbow of unknown etiology, which leads to degeneration of the origin of the wrist and elbow extensor tendons, being a common cause of lateral elbow pain. Although it is self-limiting, it can present a prolonged course, in some cases exceeding the year of duration.
There are many available treatments able to improve symptoms, including orthotic devices. Wrist splint and the forearm band are some of the main types of orthotic devices classically used in lateral epicondylitis, each acting on a different anatomical substrate. Wrist splints act through provision of rest to extensor muscles, while forearm bands are equivalent to an extension of the area of origin of extensor muscles, thus reducing insertion stress.
At the moment, it is not clear which type of orthosis is the best choice for the treatment of lateral epicondylitis.
Methods
To answer the question, we used Epistemonikos, the largest database of systematic reviews in health, which is maintained by screening multiple information sources, including MEDLINE, EMBASE, Cochrane, among others, to identify systematic reviews and their included primary studies. We extracted data from the identified reviews and reanalyzed data from primary studies included in those reviews. With this information, we generated a structured summary denominated FRISBEE (Friendly Summary of Body of Evidence using Epistemonikos) using a pre-established format, which includes key messages, a summary of the body of evidence (presented as an evidence matrix in Epistemonikos), meta-analysis of the total of studies when it is possible, a summary of findings table following the GRADE approach and a table of other considerations for decision-making.
|
Key messages
|
About the body of evidence for this question
|
What is the evidence. |
We found three systematic reviews [1],[2],[3],[4], that include four primary studies relevant for the question of interest [5],[6],[7],[8]. All of them correspond to randomized controlled trials. |
|
What types of patients were included* |
The characteristics of the patients included were: Regarding the time of duration of disease; one trial included patients with at least three weeks of symptoms [8], another trial included patients with at least one month of [7], another with less than three weeks [5] and one of the trials [6] did not specify the duration of symptoms. Regarding previous treatments, one trial [5] restricted inclusion criteria to those that had not received prior treatment with corticosteroid injections or physical therapy. Another trial [6] did not allow any previous treatment, another [8] included patients who had not received corticosteroid injections in the last month. No information about this matter was reported in one trial [7]. |
|
What types of interventions were included* |
All of the trials used a forearm band as control group, described as ‘lateral epicondyle bandage’ [5], ‘Hely & Weber forearm counterforce strap brace’ [6], ‘Elbow-Band’ [7] and ‘Thamert Epi-med elbow band’ [8]. All trials compared against wrist splint, described as ‘wrist extension splint’ [5], ‘Hely & Weber wrist extension splint’ [6], ‘wrist splintage’ [7] and ‘forearm/hand splint’. Regarding the use of the orthosis, the trials advised their patients to use it in the following way: continuously, removing the orthosis no more than one hour per day [5], during hours of the day [6] and during daily activity [7],[8]. The use was indicated for: six weeks [5],[6],[8] and three months [7]. Regarding additional therapies, one trial [6] added local cold and stretching exercises to both intervention groups. |
|
What types of outcomes |
The systematic reviews grouped the outcomes as follows:
|
* The information about primary studies is extracted from the systematic reviews identified, unless otherwise specified.
Summary of Findings
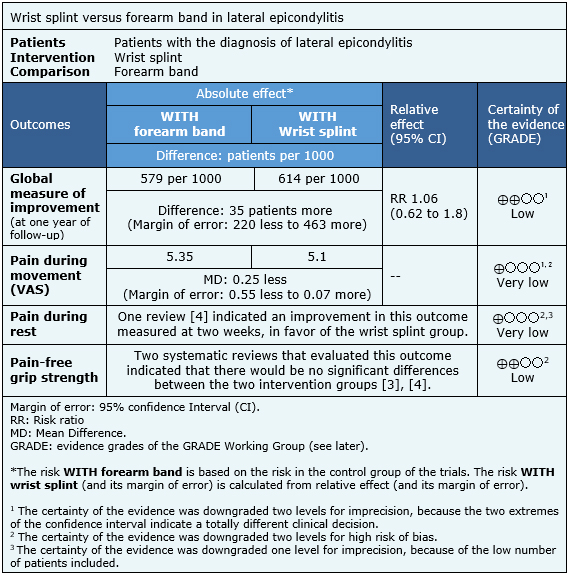
The information on the effects of both types of orthosis on lateral epicondylitis is based on four randomized trials involving 171 patients.
One trial measured global measure of improvement (37 patients) [7], at one year follow up, two trials reported pain during movement (91 patients) at six weeks, one using VAS scale [5] and the other ASES Score [6].
One trial reported pain during rest (49 patients) at two and six weeks [5]. It was not possible to reanalyze data of the primary studies for this outcome, so we present the value obtained by one of the systematic reviews [4].
Three trials measured pain-free grip strength (129 patients) [5],[7],[8]. It was not possible to reanalyze data of the primary studies for this outcome, so we present the values obtained by two systematic reviews [3],[4].
The summary of findings is the following:
- There might be no difference in global measure of improvement between forearm band and wrist splint. The certainty of the evidence is low.
- It is not clear whether using a wrist splint reduces pain during movement more than the forearm band, because the certainty of the evidence is very low.
- It is not clear whether using a wrist splint could lead to a reduction in pain during rest in comparison to a forearm band, because the certainty of the evidence is very low.
- There might be no difference in pain-free grip strength between using a forearm band and a wrist splint. The certainty of the evidence is low.

Summary of Findings
The information on the effects of both types of orthosis on lateral epicondylitis is based on four randomized trials involving 171 patients.
One trial measured global measure of improvement (37 patients) [7], at one year follow up, two trials reported pain during movement (91 patients) at six weeks, one using VAS scale [5] and the other ASES Score [6].
One trial reported pain during rest (49 patients) at two and six weeks [5]. It was not possible to reanalyze data of the primary studies for this outcome, so we present the value obtained by one of the systematic reviews [4].
Three trials measured pain-free grip strength (129 patients) [5], [7], [8]. It was not possible to reanalyze data of the primary studies for this outcome, so we present the values obtained by two systematic reviews [3], [4].
The summary of findings is the following:
· There might be no difference in global measure of improvement between forearm band and wrist splint. The certainty of the evidence is low.
· It is not clear whether using a wrist splint reduces pain during movement more than the forearm band, because the certainty of the evidence is very low.
· It is not clear whether using a wrist splint could lead to a reduction in pain during rest in comparison to a forearm band, because the certainty of the evidence is very low.
· There might be no difference in pain-free grip strength between using a forearm band and a wrist splint. The certainty of the evidence is low.
Other considerations for decision-making
|
To whom this evidence does and does not apply |
|
| About the outcomes included in this summary |
|
| Balance between benefits and risks, and certainty of the evidence |
|
| Resource considerations |
|
| What would patients and their doctors think about this intervention |
|
|
Differences between this summary and other sources |
|
| Could this evidence change in the future? |
|
How we conducted this summary
Using automated and collaborative means, we compiled all the relevant evidence for the question of interest and we present it as a matrix of evidence.
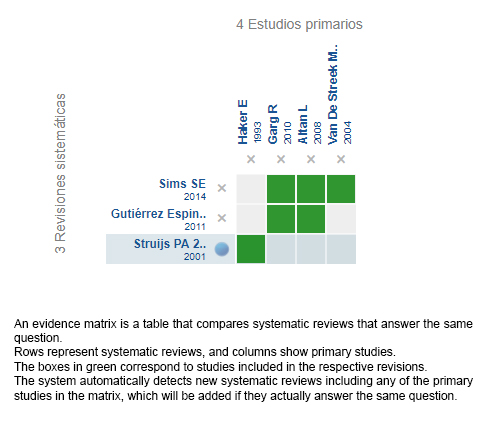
Follow the link to access the interactive version: Wrist splint versus forearm band for lateral epicondylitis
Notes
The upper portion of the matrix of evidence will display a warning of “new evidence” if new systematic reviews are published after the publication of this summary. Even though the project considers the periodical update of these summaries, users are invited to comment in Medwave or to contact the authors through email if they find new evidence and the summary should be updated earlier.
After creating an account in Epistemonikos, users will be able to save the matrixes and to receive automated notifications any time new evidence potentially relevant for the question appears.
This article is part of the Epistemonikos Evidence Synthesis project. It is elaborated with a pre-established methodology, following rigorous methodological standards and internal peer review process. Each of these articles corresponds to a summary, denominated FRISBEE (Friendly Summary of Body of Evidence using Epistemonikos), whose main objective is to synthesize the body of evidence for a specific question, with a friendly format to clinical professionals. Its main resources are based on the evidence matrix of Epistemonikos and analysis of results using GRADE methodology. Further details of the methods for developing this FRISBEE are described here (http://dx.doi.org/10.5867/medwave.2014.06.5997)
Epistemonikos foundation is a non-for-profit organization aiming to bring information closer to health decision-makers with technology. Its main development is Epistemonikos database (www.epistemonikos.org).
Potential conflicts of interest
The authors do not have relevant interests to declare.
