Epistemonikos summaries
← vista completaPublished on September 28, 2018 | http://doi.org/10.5867/medwave.2018.05.7258
What are the benefits and risks of total arthroplasty in arthrodesed knees?
¿Cuáles son los beneficios y riesgos de la artroplastia total en rodillas artrodesadas?
Abstract
INTRODUCTION The conversion of a previously arthrodesed knee to a total knee arthroplasty is an alternative seldom used. However, arthroplasty would provide greater functionality to the arthrodesed joint. Since it is a technically demanding procedure, not exempt from complications, there is controversy about the role of this intervention.
METHODS To answer this question we used Epistemonikos, the largest database of systematic reviews in health, which is maintained by screening multiple information sources, including MEDLINE, EMBASE, Cochrane, among others. We extracted data from the systematic reviews, reanalyzed data of primary studies, conducted a meta-analysis and generated a summary of findings table using the GRADE approach.
RESULTS AND CONCLUSIONS We identified two systematic reviews including 10 studies overall, none of which corresponded to a randomized trial. We concluded the conversion of knee arthrodesis to total knee arthroplasty could increase the functionality, but it is not clear whether it increases the complications or if it has any impact on pain or patient satisfaction because the certainty of the evidence is very low.
Problem
Arthrodesis is a salvage surgical procedure, whose objective is to achieve fusion between two bones and eliminate movement of the joint between them. It is used as the last surgical option in different articular conditions, usually in the knee and hip, in order to decrease pain and to improve satisfaction. Some examples are advanced inflammatory arthritis, tuberculosis sequelae, hemophilic arthropathies, tumoral lesions, among others. However, immobility secondary to the fusion and the subsequent overload of the adjacent joints, can lead to serious physical and psychosocial limitations.
On the other hand, total knee arthroplasty is a surgical procedure in which the damaged joint surfaces are replaced by modular prosthetic components. This procedure is currently recognized as the first option to treat severe knee osteoarthritis, with good results both in functionality and quality of life.
The objective of the arthrodesis to arthroplasty conversion is to restore the range of movement in the joint, leading to an improvement in the functionality of the patient. However, it is not a procedure that is performed frequently, since it is technically demanding and has a high rate of complications.
It is currently unclear what is the role of the conversion of arthrodesis to total knee arthroplasty.
Methods
To answer the question, we used Epistemonikos, the largest database of systematic reviews in health, which is maintained by screening multiple information sources, including MEDLINE, EMBASE, Cochrane, among others, to identify systematic reviews and their included primary studies. We extracted data from the identified reviews and reanalyzed data from primary studies included in those reviews. With this information, we generated a structured summary denominated FRISBEE (Friendly Summary of Body of Evidence using Epistemonikos) using a pre-established format, which includes key messages, a summary of the body of evidence (presented as an evidence matrix in Epistemonikos), meta-analysis of the total of studies when it is possible, a summary of findings table following the GRADE approach and a section of other considerations for decision-making.
|
Key messages
|
About the body of evidence for this question
|
What is the evidence. |
We found two systematic reviews [1],[2] including 10 primary studies [3],[4],[5],[6],[7],[8],[9],[10],[11],[12], none of which corresponded to a randomized trial. All primary studies were retrospective cohorts. |
|
What types of patients were included* |
All studies included patients with knee arthrodesis.The average age ranged between 39 and 68.5 years in the different studies. The reason for arthrodesis varied between studies, predominating infectious causes and osteoarthritis. Knees remained arthrodesed prior to arthroplasty for 9 to 25 years in average. Eight studies exclusively included patients with surgical arthrodesis, in which an intervention is performed to produce the arthrodesis [3],[4],[5],[7],[8],[9],[11],[12] and two also included non-surgical arthrodesis, which occur as a result of joint disease (i.e. ankylosis) [6],[10]. We excluded case reports that included only one patient and studies that only considered non-surgical arthrodesis (ankylosis). |
|
What types of interventions were included* |
Different types of prosthesis were used: non-constrained [9], semiconstrained [5],[11], with posterior stabilization [5],[8],[10], constrained [9] and hinge (rotational true hinge) [5],[12], among others. All studies compared under the assumption that each patient could be considered its own control. |
|
What types of outcomes |
The studies reported multiple outcomes, which were grouped by the systematic reviews as follows:
The average follow-up of the studies was 4.8 years, with a range between two and eight years. |
* The information about primary studies is extracted from the systematic reviews identified, unless otherwise specified.
Summary of findings
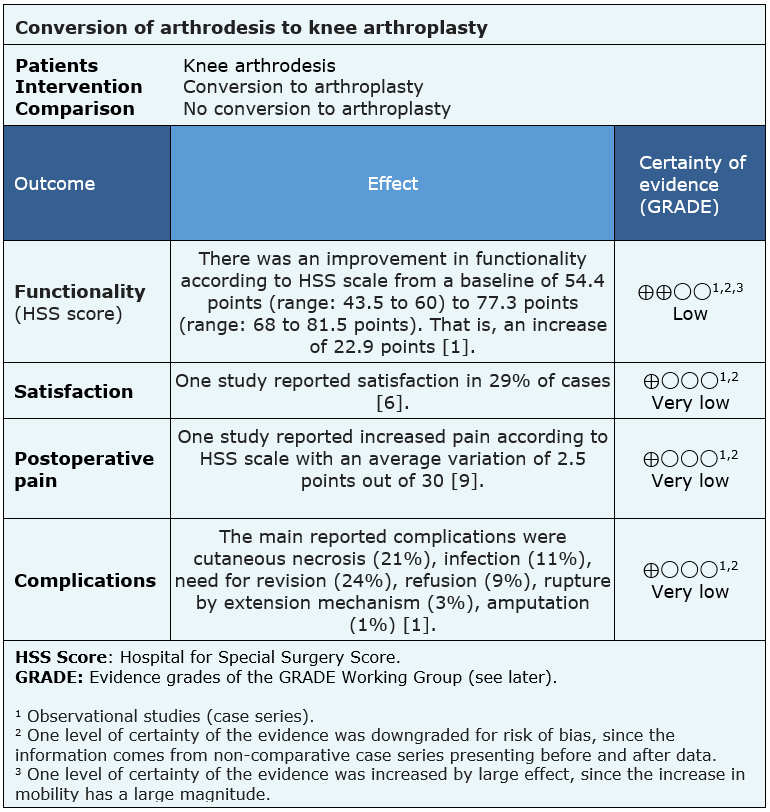
The information on the effects of the conversion of knee arthrodesis to total knee arthroplasty is based on ten primary studies including 143 patients.
Five studies reported postoperative functionality (27 patients) [4],[8],[9],[10],[12]; five studies reported satisfaction (40 patients) [5],[6],[8],[9],[12]; four studies reported postoperative pain (88 patients) [6],[9],[10],[11] and eight studies reported complications (70 patients) [3],[4],[5],[7],[8],[9],[11],[12]. None of the reviews presented data that could be re-analyzed or pooled in a meta-analysis, so the conclusions are presented as they were presented by the systematic reviews identified.
The summary of findings is as follows:
- The conversion of knee arthrodesis to arthroplasty might increase functionality, but the certainty of the evidence is low.
- It is not clear what is the effect of the conversion of knee arthrodesis to arthroplasty on patient satisfaction because the certainty of the evidence is very low.
- It is not clear what is the effect of the conversion of knee arthrodesis to arthroplasty on postoperative pain because the certainty of the evidence is very low.
- It is not clear what is the frequency or magnitude of the complications of knee arthrodesis to arthroplasty because the certainty of the evidence is very low.
| Follow the link to access the interactive version of this table (Interactive Summary of Findings – iSoF) |

Other considerations for decision-making
|
To whom this evidence does and does not apply |
|
| About the outcomes included in this summary |
|
| Balance between benefits and risks, and certainty of the evidence |
|
| Resource considerations |
|
| What would patients and their doctors think about this intervention |
|
|
Differences between this summary and other sources |
|
| Could this evidence change in the future? |
|
How we conducted this summary
Using automated and collaborative means, we compiled all the relevant evidence for the question of interest and we present it as a matrix of evidence.
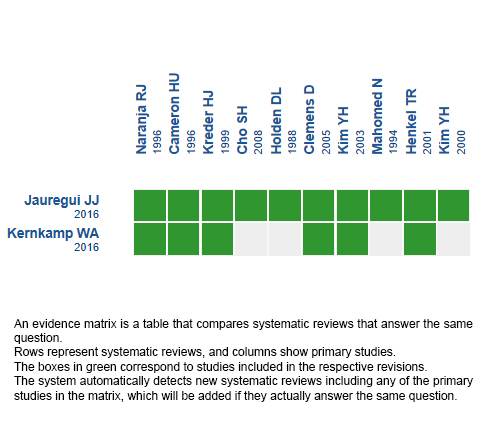
Follow the link to access the interactive version: Conversion of knee arthrodesis to arthroplasty.
Notes
The upper portion of the matrix of evidence will display a warning of “new evidence” if new systematic reviews are published after the publication of this summary. Even though the project considers the periodical update of these summaries, users are invited to comment in Medwave or to contact the authors through email if they find new evidence and the summary should be updated earlier.
After creating an account in Epistemonikos, users will be able to save the matrixes and to receive automated notifications any time new evidence potentially relevant for the question appears.
This article is part of the Epistemonikos Evidence Synthesis project. It is elaborated with a pre-established methodology, following rigorous methodological standards and internal peer review process. Each of these articles corresponds to a summary, denominated FRISBEE (Friendly Summary of Body of Evidence using Epistemonikos), whose main objective is to synthesize the body of evidence for a specific question, with a friendly format to clinical professionals. Its main resources are based on the evidence matrix of Epistemonikos and analysis of results using GRADE methodology. Further details of the methods for developing this FRISBEE are described here (http://dx.doi.org/10.5867/medwave.2014.06.5997)
Epistemonikos foundation is a non-for-profit organization aiming to bring information closer to health decision-makers with technology. Its main development is Epistemonikos database (www.epistemonikos.org).
Potential conflicts of interest
The authors do not have relevant interests to declare.
