Resúmenes Epistemonikos
← vista completaPublicado el 29 de octubre de 2018 | http://doi.org/10.5867/medwave.2018.06.7318
Retroceso bilateral de rectos laterales comparado con retroceso/resección unilateral para el tratamiento de la exotropia intermitente básica
Bilateral lateral rectus recession versus unilateral recession/resection for basic intermittent exotropia
Abstract
INTRODUCTION Intermittent exotropia requires surgical resolution under some clinical circumstances. The main techniques are bilateral lateral rectus recession and unilateral recess/resection. Although bilateral recession is the most widely used, it is not clear whether it leads to better results.
METHODS To answer this question we used Epistemonikos, the largest database of systematic reviews in health, which is maintained by screening multiple information sources, including MEDLINE, EMBASE, Cochrane, among others. We extracted data from the systematic reviews, reanalyzed data of primary studies, conducted a meta-analysis and generated a summary of findings table using the GRADE approach.
RESULTS AND CONCLUSIONS We identified five systematic reviews including seven studies overall, of which three were randomized trials. We concluded unilateral recess/resection might achieve greater surgical success and probably decrease the rate of undercorrection/recurrence when compared to bilateral lateral rectus recession.
Problem
Intermittent exotropia is the most frequent exo-deviation in childhood and is characterized by the deviation from one eye to lateral, typically during distance fixation or periods of inattention [1]. When this exo-deviation also occurs in the near fixation, in such way that the difference of the angle of deviation between the gaze fixation for distance and for near does not exceed 10 prism diopters, it is called basic intermittent exotropia. This condition can sometimes lead to stereopsis and alteration of binocular vision (fusion), negatively affecting the vision, even though only a small proportion develop amblyopia.
In this sense, the main objective of the treatment (medical, surgical, or a combination of both) is to normalize or improve the ocular alignment while maintaining or improving binocular vision and stereopsis. However, the success and risks associated with each type of treatment varies, so the surgical option is indicated mainly in the event of failure of medical treatment, large angle of exodeviation, or by decision of parents. There are two main surgical techniques, whose common objective is to adjust position or length of the extraocular muscles on the horizontal axis: unilateral recession/resection, which consists of unilateral lateral rectus muscle recession and medial rectus muscle resection, and bilateral lateral rectus recession. Even though the latter is most commonly performed, it is not clear whether this technique is superior to the unilateral recession/resection in terms of success and/or complications.
Methods
To answer the question, we used Epistemonikos, the largest database of systematic reviews in health, which is maintained by screening multiple information sources, including MEDLINE, EMBASE, Cochrane, among others, to identify systematic reviews and their included primary studies. We extracted data from the identified reviews and reanalyzed data from primary studies included in those reviews. With this information, we generated a structured summary denominated FRISBEE (Friendly Summary of Body of Evidence using Epistemonikos) using a pre-established format, which includes key messages, a summary of the body of evidence (presented as an evidence matrix in Epistemonikos), meta-analysis of the total of studies when it is possible, a summary of findings table following the GRADE approach and a section of other considerations for decision-making.
|
Key messages
|
About the body of evidence for this question
|
What is the evidence. |
We found five systematic reviews [1],[2],[3],[4],[5] including seven primary studies [6],[7],[8],[9],[10],[11],[12], of which three were randomized trials [6],[7],[8]. One systematic review [4] did not find studies meeting its inclusion criteria and another systematic review [5] did not mention which studies were included (authors were contacted via e-mail, with no response). This table and the summary in general are based on the three randomized trials identified [6],[7],[8], since the observational studies [9],[10],[11],[12] did not increase the certainty of the existing evidence, nor did they provide relevant additional information. |
|
What types of patients were included* |
All the trials included patients with a diagnosis of basic intermittent exotropia with an exodeviation angle ranging between 22 and 50 diopters **. |
|
What types of interventions were included* |
All trials compared both types of surgeries, unilateral recess/resection versus bilateral lateral rectus recession. The surgical correction formula used by the trials, or the equivalence between them, was not reported by the included reviews. |
|
What types of outcomes |
The trials measured multiple outcomes, but the identified systematic reviews pooled them as follows:
The minimum follow-up of the studies was 12 months, with a range from 12 to 15 months. All the results reported here correspond to the last follow-up consultation. |
* The information about primary studies is extracted from the systematic reviews identified, unless otherwise specified.
Summary of findings
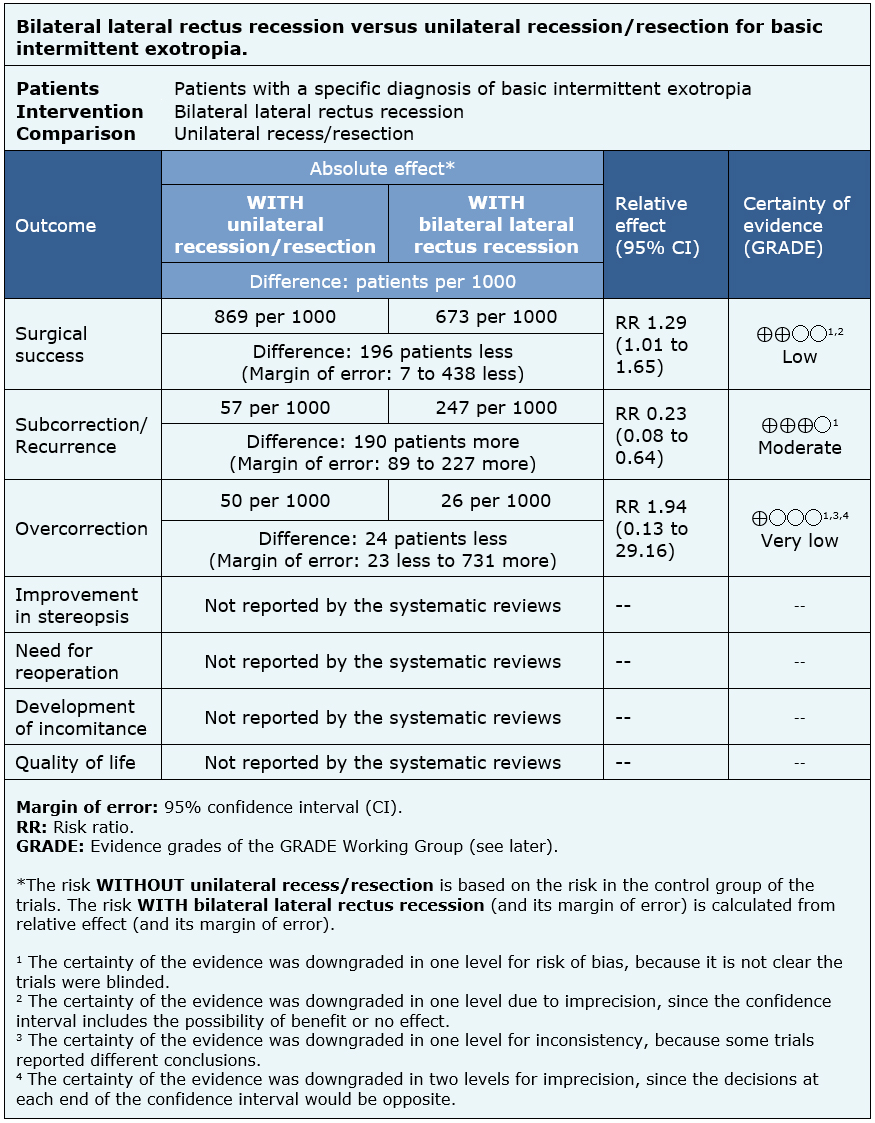
The information on the effects of unilateral recess/resection versus bilateral lateral rectus recession for the treatment of the basic intermittent exotropia is based on three randomized trials that included 201 patients.
Three trials measured surgical success (201 patients) [6],[7],[8], two trials measured undercorrection/recurrence (154 patients) [6],[8] and two trials measured overcorrection (154 patients) [6],[8].
The summary of findings is as follows:
- Unilateral recess/resection might achieve greater surgical success than bilateral lateral rectus recession, but the certainty of the evidence is low.
- Unilateral recess/resection probably decreases the rate of undercorrection/recurrence compared with bilateral lateral rectus recession. The certainty of the evidence is moderate.
- It is not clear if there are differences in overcorrection between both techniques because the certainty of the evidence is very low.
- Improvement in stereopsis, need for reintervention, development of incomitance, postoperative discomfort and quality of life were not reported by the systematic reviews.
| Follow the link to access the interactive version of this table (Interactive Summary of Findings – iSoF) |

Other considerations for decision-making
|
To whom this evidence does and does not apply |
|
| About the outcomes included in this summary |
|
| Balance between benefits and risks, and certainty of the evidence |
|
| Resource considerations |
|
| What would patients and their doctors think about this intervention |
|
|
Differences between this summary and other sources |
|
| Could this evidence change in the future? |
|
How we conducted this summary
Using automated and collaborative means, we compiled all the relevant evidence for the question of interest and we present it as a matrix of evidence.
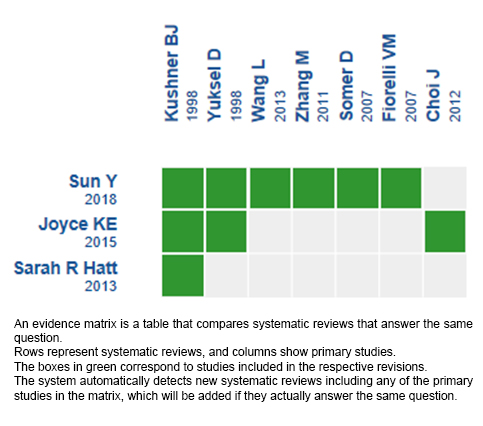
Follow the link to access the interactive version: Bilateral lateral rectus recessions versus unilateral recession/resection for basic intermittent exotropia.
Notes
The upper portion of the matrix of evidence will display a warning of “new evidence” if new systematic reviews are published after the publication of this summary. Even though the project considers the periodical update of these summaries, users are invited to comment in Medwave or to contact the authors through email if they find new evidence and the summary should be updated earlier.
After creating an account in Epistemonikos, users will be able to save the matrixes and to receive automated notifications any time new evidence potentially relevant for the question appears.
This article is part of the Epistemonikos Evidence Synthesis project. It is elaborated with a pre-established methodology, following rigorous methodological standards and internal peer review process. Each of these articles corresponds to a summary, denominated FRISBEE (Friendly Summary of Body of Evidence using Epistemonikos), whose main objective is to synthesize the body of evidence for a specific question, with a friendly format to clinical professionals. Its main resources are based on the evidence matrix of Epistemonikos and analysis of results using GRADE methodology. Further details of the methods for developing this FRISBEE are described here (http://dx.doi.org/10.5867/medwave.2014.06.5997)
Epistemonikos foundation is a non-for-profit organization aiming to bring information closer to health decision-makers with technology. Its main development is Epistemonikos database (www.epistemonikos.org).
Potential conflicts of interest
The authors do not have relevant interests to declare.
