Resúmenes Epistemonikos
← vista completaPublicado el 11 de junio de 2019 | http://doi.org/10.5867/medwave.2019.05.7639
Efectos de la dieta mediterránea en el tratamiento de la artritis reumatoide
Effects of Mediterranean diet on the treatment of rheumatoid arthritis
Abstract
INTRODUCTION It has been suggested that environmental and lifestyle factors might contribute to the severity and progression of inflammation in rheumatoid arthritis. An intervention generating high interest due to its supposed anti-inflammatory properties is the Mediterranean diet.
METHODS We searched in Epistemonikos, the largest database of systematic reviews in health, which is maintained by screening multiple information sources, including MEDLINE, EMBASE, Cochrane, among others. We extracted data from the systematic reviews, reanalyzed data of primary studies, conducted a meta-analysis and generated a summary of findings table using the GRADE approach.
RESULTS AND CONCLUSIONS We identified seven systematic reviews including four primary studies, of which only one corresponded to a randomized trial. We concluded Mediterranean diet may make little or no difference in pain or disease activity and may slightly increase weight in rheumatoid arthritis patients, but the certainty of the evidence is low. On the other hand, it was not possible to clearly establish whether Mediterranean diet has any effect on functionality, morning stiffness or quality of life as the certainty of the existing evidence has been assessed as very low.
Problem
Rheumatoid arthritis is a chronic autoimmune disease whose etiology is not fully known. There are important variations in its frequency, which cannot only be attributed to genetic or racial factors, so it has been suggested that environmental factors, such as tobacco use and diet might contribute to both the development and the severity of the disease [1].
Moreover, the Mediterranean diet has beneficial effects in the prevention and treatment of various health conditions, which are mediated by various mechanisms, such as increasing antioxidant levels, modifying intestinal flora, promoting an anti-inflammatory lipid profile (omega 3: omega 6 ratio) and possibly decreasing inflammation in other ways [2]. Its anti-inflammatory properties have generated a particular interest in its use as part of the treatment of rheumatoid arthritis, however, if this really translates into a relevant clinical effect is a matter of controversy.
Methods
We searched in Epistemonikos, the largest database of systematic reviews in health, which is maintained by screening multiple information sources, including MEDLINE, EMBASE, Cochrane, among others, to identify systematic reviews and their included primary studies. We extracted data from the identified reviews and reanalyzed data from primary studies included in those reviews. With this information, we generated a structured summary denominated FRISBEE (Friendly Summary of Body of Evidence using Epistemonikos) using a pre-established format, which includes key messages, a summary of the body of evidence (presented as an evidence matrix in Epistemonikos), meta-analysis of the total of studies when it is possible, a summary of findings table following the GRADE approach and a table of other considerations for decision-making.
|
Key messages
|
About the body of evidence for this question
|
What is the evidence. |
We found seven systematic reviews [1], [2], [3], [4], [5], [6], [7] which included four primary studies, reported in six references [8], [9], [10], [11], [12], [13] of which only one was a randomized trial [8]. The information provided by the observational studies did not increase the level of certainty of the evidence, nor did add new relevant information. Therefore the table presented and the summary is based on the only randomized trial. |
|
What types of patients were included* |
The trial was conducted in Sweden [8] and included 51 patients, mostly women (82.3%), with rheumatoid arthritis diagnosed by criteria ACR 1987, with at least two years from diagnosis and controlled disease according to the clinician criteria at randomization. The trial excluded patients who already had a vegetarian or Mediterranean diet, with high doses of corticosteroids, or recent adjustments in therapy. |
|
What types of interventions were included* |
The trial [8] evaluated a Mediterranean diet high in oils for 12 weeks in the intervention group, compared to Western diet in the control group. The intervention was conducted in two stages with three weeks of education and diet in the hospital, followed by nine weeks of strict clinical follow-up where the food included in the diet was provided. |
|
What types of outcomes |
The trial [8] evaluated multiple outcomes, which were grouped by the systematic reviews as follows:
|
* The information about primary studies is extracted from the systematic reviews identified, unless otherwise specified.
Summary of findings
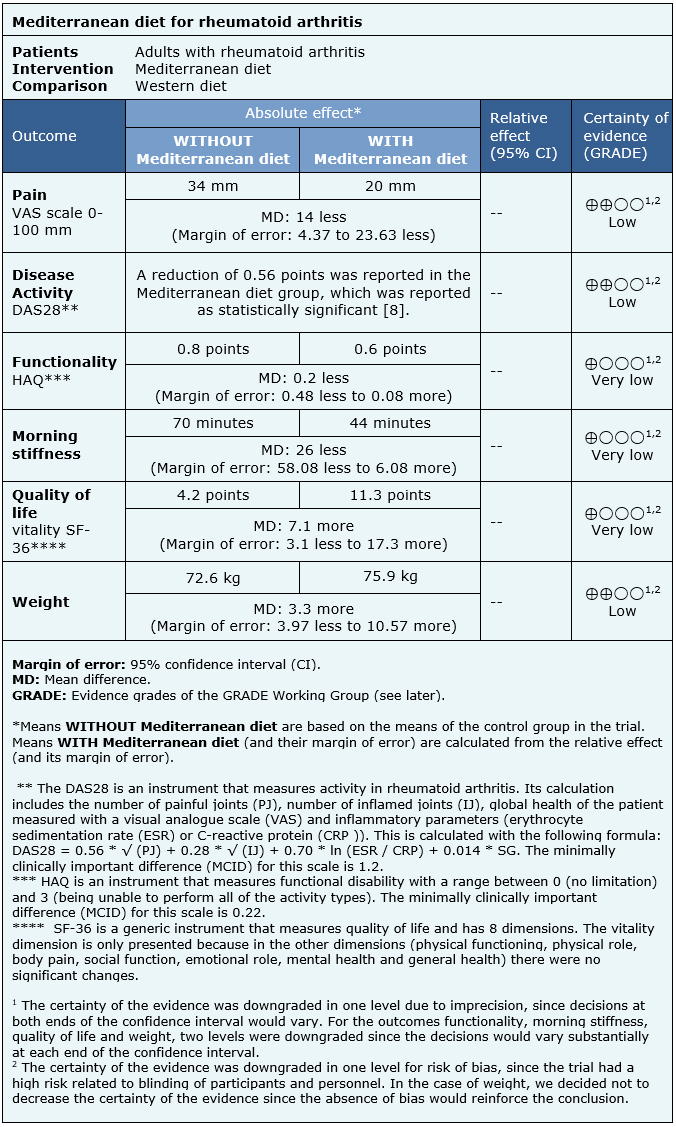
The information on the effects of the Mediterranean diet in rheumatoid arthritis is based on one randomized trial [8] that included 51 patients for the outcomes pain, disease activity, functionality, morning stiffness, quality of life and weight.
The summary of findings is as follows:
- Mediterranean diet may make little or no difference to pain in rheumatoid arthritis (low certainty of the evidence).
- Mediterranean diet may make little or no difference to disease activity in rheumatoid arthritis (low certainty of the evidence).
- We are uncertain whether Mediterranean diet improves functionality in rheumatoid arthritis as the certainty of the evidence has been assessed as very low.
- We are uncertain whether Mediterranean diet improves morning stiffness in rheumatoid arthritis as the certainty of the evidence has been assessed as very low.
- We are uncertain whether Mediterranean diet improves quality of life in rheumatoid arthritis as the certainty of the evidence has been assessed as very low.
- Mediterranean diet may slightly increase weight in rheumatoid arthritis (certainty of low evidence).
| Follow the link to access the interactive version of this table (Interactive Summary of Findings – iSoF) |

Other considerations for decision-making
|
To whom this evidence does and does not apply |
|
| About the outcomes included in this summary |
|
| Balance between benefits and risks, and certainty of the evidence |
|
| Resource considerations |
|
| What would patients and their doctors think about this intervention |
|
|
Differences between this summary and other sources |
|
| Could this evidence change in the future? |
|
How we conducted this summary
Using automated and collaborative means, we compiled all the relevant evidence for the question of interest and we present it as a matrix of evidence.
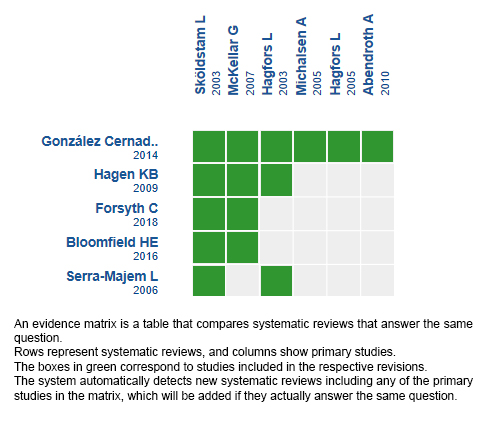
Follow the link to access the interactive version: Mediterranean diet for rheumatoid arthritis.
Notes
The upper portion of the matrix of evidence will display a warning of “new evidence” if new systematic reviews are published after the publication of this summary. Even though the project considers the periodical update of these summaries, users are invited to comment in Medwave or to contact the authors through email if they find new evidence and the summary should be updated earlier.
After creating an account in Epistemonikos, users will be able to save the matrixes and to receive automated notifications any time new evidence potentially relevant for the question appears.
This article is part of the Epistemonikos Evidence Synthesis project. It is elaborated with a pre-established methodology, following rigorous methodological standards and internal peer review process. Each of these articles corresponds to a summary, denominated FRISBEE (Friendly Summary of Body of Evidence using Epistemonikos), whose main objective is to synthesize the body of evidence for a specific question, with a friendly format to clinical professionals. Its main resources are based on the evidence matrix of Epistemonikos and analysis of results using GRADE methodology. Further details of the methods for developing this FRISBEE are described here (http://dx.doi.org/10.5867/medwave.2014.06.5997)
Epistemonikos foundation is a non-for-profit organization aiming to bring information closer to health decision-makers with technology. Its main development is Epistemonikos database (www.epistemonikos.org).
Potential conflicts of interest
The authors do not have relevant interests to declare.
