Epistemonikos summaries
← vista completaPublished on July 30, 2020 | http://doi.org/10.5867/medwave.2020.06.7982
Preventive effectiveness of varicella vaccine in healthy unexposed patients
Efectividad preventiva de la vacuna varicela en pacientes sanos no expuestos
Abstract
INTRODUCTION Chickenpox is an infectious disease caused by varicella-zoster virus. Varicella vaccine is conventionally used for its prevention, and its administration seeks to reduce the onset of the disease and complications associated. However, there is still controversy about its effectiveness.
METHODS We searched in Epistemonikos, the largest database of systematic reviews in health, which is maintained by screening multiple information sources, including MEDLINE, EMBASE, Cochrane, among others. We extracted data from the systematic reviews, reanalyzed data of primary studies, conducted a meta-analysis and generated a summary of findings table using the GRADE approach.
RESULTS AND CONCLUSIONS We identified two systematic reviews including 16 studies overall, of which three were randomized trials. We concluded that the varicella vaccine decreases the risk of contracting the disease in the long term and probably reduces the risk of developing the disease in the short term in healthy unexposed patients. Nevertheless, the vaccination increases the occurrence of local reactions 48 hours after its administration and probably increases the presence of fever and chickenpox-like rash.
Problem
Chickenpox is an infectious disease caused by varicella-zoster virus. Most cases occur in childhood (under 14 years old), so it has been identified as an important cause of school absenteeism, generating significant expenses to the community [1] [2]. Chickenpox diagnosis is clinical, characterized by pruritic, vesicular, cephalocaudal, polymorph rash, with scalp involvement, generally associated to fever.
Usually, varicella vaccine is used for disease prevention, which is a live attenuated vaccine that induces humoral immune response. Its administration would prevent the onset of disease and its complications. However, there is still controversy regarding its effectiveness in reducing chickenpox in the short and long term.
Methods
We searched in Epistemonikos, the largest database of systematic reviews in health, which is maintained by screening multiple information sources, including MEDLINE, EMBASE, Cochrane, among others, to identify systematic reviews and their included primary studies. We extracted data from the identified reviews and reanalyzed data from primary studies included in those reviews. With this information, we generated a structured summary denominated FRISBEE (Friendly Summary of Body of Evidence using Epistemonikos) using a pre-established format, which includes key messages, a summary of the body of evidence (presented as an evidence matrix in Epistemonikos), meta-analysis of the total of studies when it is possible, a summary of findings table following the GRADE approach and a table of other considerations for decision-making.
|
Key messages
|
About the body of evidence for this question
|
What is the evidence. |
We identified two systematic reviews [3], [4], which including 16 primary studies reported in 17 references [5], [6], [7], [8], [9], [10], [11], [12], [ 13], [14], [15], [16], [17], [18], [19], [20], [21], of which two correspond to randomized trials reported in three references [19], [20], [21]. This table and the summary in general are based on the latter, since observational studies did not increase the certainty of existing evidence, nor did they provide additional relevant information. |
|
What types of patients were included* |
All trials included healthy patients, with no history of chickenpox or vaccination against the disease. One trial included patients between one and 14 years old [20], while the other trial included patients between 10 to 30 months old [21]. |
|
What types of interventions were included* |
All trials evaluated one dose of Oka strain varicella vaccine [20], [21]. Both trials compared vaccination against an unvaccinated control group [20], [21]. In addition, one of the trials included a comparison with no follow-up of the control group [20], so in this summary the authors decided to evaluate it assuming the worst case scenario, meaning that no one in the unvaccinated control group develop chicken pox in the follow-up years. |
|
What types of outcomes |
Trials reported multiple outcomes, which were grouped by systematic reviews as follows:
|
* Information about primary studies is not extracted directly from primary studies but from identified systematic reviews, unless otherwise stated.
Summary of findings
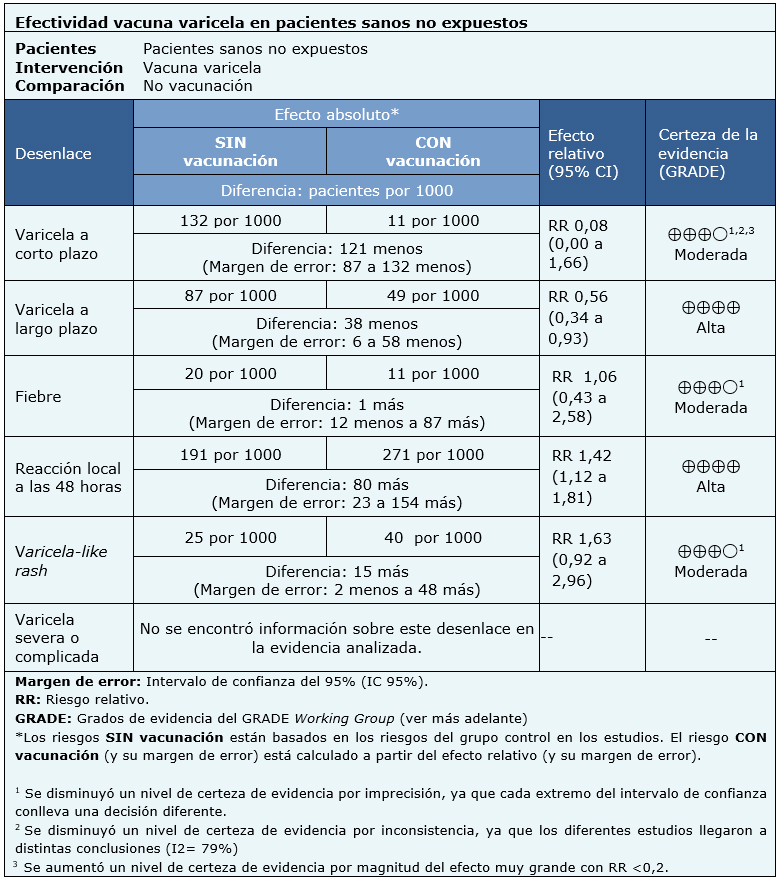
Information about varicella vaccine effects is based on two randomized trials that included 1449 patients.
Both trials measured short-term chickenpox and chickenpox-like rash as outcomes (1407 patients) [20], [21]. One of the trials measured long-term chickenpox, fever and local reactions (914 patients) [20]. No trial reported the outcome severe or complicated chickenpox.
The summary of findings is as follows:
- Vaccination against chickenpox probably decreases the risk of developing the disease in the short term (moderate certainty evidence).
- Vaccination against chickenpox decreases the risk of developing the disease in the long term (high certainty evidence).
- Vaccination against chickenpox probably results in little or no difference in the onset of fever after administration (moderate certainty evidence).
- Vaccination against chickenpox increases the occurrence of local reactions within 48 hours after administration (high certainty evidence).
- Vaccination against chickenpox probably increases the appearance of chickenpox-like rash after administration (moderate certainty evidence).
| Follow the link to access the interactive version of this table (Interactive Summary of Findings – iSoF) |

Other considerations for decision-making
|
To whom this evidence does and does not apply |
|
| About the outcomes included in this summary |
|
| Balance between benefits and risks, and certainty of the evidence |
|
| Resource considerations |
|
| What would patients and their doctors think about this intervention |
|
|
Differences between this summary and other sources |
|
| Could this evidence change in the future? |
|
How we conducted this summary
Using automated and collaborative means, we compiled all the relevant evidence for the question of interest and we present it as a matrix of evidence.
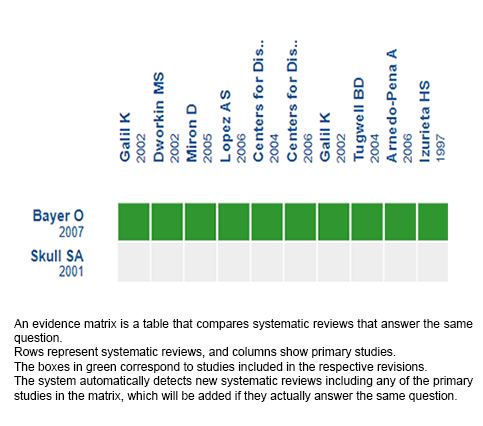
Follow the link to access the interactive version: Effectiveness of varicella vaccine in healthy unexposed patients.
Notes
The upper portion of the matrix of evidence will display a warning of “new evidence” if new systematic reviews are published after the publication of this summary. Even though the project considers the periodical update of these summaries, users are invited to comment in Medwave or to contact the authors through email if they find new evidence and the summary should be updated earlier.
After creating an account in Epistemonikos, users will be able to save the matrixes and to receive automated notifications any time new evidence potentially relevant for the question appears.
This article is part of the Epistemonikos Evidence Synthesis project. It is elaborated with a pre-established methodology, following rigorous methodological standards and internal peer review process. Each of these articles corresponds to a summary, denominated FRISBEE (Friendly Summary of Body of Evidence using Epistemonikos), whose main objective is to synthesize the body of evidence for a specific question, with a friendly format to clinical professionals. Its main resources are based on the evidence matrix of Epistemonikos and analysis of results using GRADE methodology. Further details of the methods for developing this FRISBEE are described here (http://dx.doi.org/10.5867/medwave.2014.06.5997)
Epistemonikos foundation is a non-for-profit organization aiming to bring information closer to health decision-makers with technology. Its main development is Epistemonikos database (www.epistemonikos.org).
Potential conflicts of interest
The authors do not have relevant interests to declare.
