Análisis
← vista completaPublicado el 20 de abril de 2026 | http://doi.org/10.5867/medwave.2026.03.3161
Colestasis intrahepática del embarazo en Chile: análisis del cambio epidemiológico y una hipótesis microbiológica
Intrahepatic cholestasis of pregnancy in Chile: Analysis of epidemiological change and a microbiological hypothesis
Abstract
Intrahepatic cholestasis of pregnancy is a gestational pathology with an unusual epidemiological and pathophysiological behavior that remains partially unexplained. Its current global incidence ranges from 0.1% to 2%. However, in Chile, the incidence reached up to 15% in the 1970s, with a marked decrease over subsequent decades, being nowadays about 1 to 2%. The reasons for this historical change are not fully understood. A literature-based analysis was conducted, focusing on clinical, microbiological, and epidemiological studies on intrahepatic cholestasis and other hepatobiliary diseases. The aim of this was to explore existing evidence and to propose a microbiological hypothesis that could help explain the epidemiological transition observed in Chile. Notably, the temporal reduction in incidence paralleled a nationwide decline in biliary disease and typhoid fever. We hypothesize that the eradication or significant reduction of certain pathogens, such as Typhi, may have contributed to the normalization of intrahepatic cholestasis of pregnancy rates in Chile.
Main messages
- Intrahepatic cholestasis of pregnancy was one of the most frequent obstetric disorders in Chile during the 1970s, with an incidence close to 15%.
- Its incidence has now declined to 1 to 2%, in parallel with the reduction of typhoid fever and other biliary diseases.
- We hypothesize that chronic Salmonella Typhi infection and changes in the gut microbiota may have contributed to the historically high prevalence of intrahepatic cholestasis of pregnancy in Chile.
- This perspective opens the possibility for new research on microbiota, infections, and intrahepatic cholestasis of pregnancy risk in the Chilean population.
- The main limitation of this analysis is that it relies on ecological/temporal correlations rather than causal evidence
Introduction
Intrahepatic cholestasis of pregnancy is a pregnancy-specific liver disorder. The epidemiology, clinical characteristics, pathophysiology, and perinatal risks make intrahepatic cholestasis of pregnancy a challenging disease [1]. The diagnosis of intrahepatic cholestasis of pregnancy is made in the presence of distinctive itching that persists for more than 48 hours, with confirmation by elevated plasma bile acids in more than > 10 µmol/L. The clinical importance of cholestasis during pregnancy does not lie in hepatic impairment itself, but rather in its association with an increased likelihood of fetal death intra utero and spontaneous preterm birth. A higher risk of meconium-stained amniotic fluid, neonatal respiratory distress, lower Apgar scores, and increased need for admission to the neonatal intensive care unit has also been reported. The risk of adverse perinatal outcomes is proportional to the severity of cholestasis, as determined by plasma bile acid levels; these levels not only classify disease severity but also guide clinical management. Notably, values higher than 100 µmol/L are significantly associated with a higher probability of fetal demise [2,3].
Chile was peculiar in the 1970s concerning its high incidence of intrahepatic cholestasis of pregnancy; during that period, one in six pregnant women in Chile developed this disease. In the last 30 years, numerous publications and consensus statements from related scientific societies have provided insights that improve our understanding of the pathophysiology of this disease and how we should manage it clinically. Additionally,over the last 30 years, intrahepatic cholestasis of pregnancy has undergone important epidemiological changes for reasons that are not well understood. In this article, we summarize key pathophysiological concepts of intrahepatic cholestasis of pregnancy, and the primary objective is to analyze its epidemiological changes in Chile, which allows us to propose a hypothesis that could explain why this disease has almost disappeared.
Methods
This is a literature-based analysis. A selective literature search was conducted in PubMed and SciELO to identify publications related to the pathophysiology and epidemiology of intrahepatic cholestasis of pregnancy, as well as associated hepatobiliary and infectious diseases. The following MeSH terms were used in PubMed: “Intrahepatic Cholestasis of Pregnancy”, “Gastrointestinal Microbiome”, “Epidemiology”, “Salmonella Typhi”. Publications in English and Spanish were considered, with a deliberate no initial date restriction because the primary objective was to analyze the historical evolution since 1970.
Observational, epidemiological, clinical, and basic science studies relevant to intrahepatic cholestasis of pregnancy were included, along with local historical studies and clinically relevant case series. Letters to the editor, commentaries, narrative reviews, and small case series without a relevant epidemiological contribution were excluded.
Given the non-systematic, selective design, the literature search was not exhaustive, and there is an inherent risk of selection bias. No formal assessment of the quality of the studies was performed. The included evidence was synthesized using a thematic narrative approach. This is not a systematic review, and no formal quality appraisal was performed.
Analysis
Pathophysiology
Hepatocytes produce bile acids from cholesterol metabolism. The ATP-dependent bile salt exporting pump (BSEP) secretes conjugated bile acids from the liver cell to the canaliculus [4]. Primary bile acids reach the intestine, where bacteria transform them into secondary bile salts. The sodium-dependent bile acid transporter (ASBT) recaptures bile acids from the intestine into the portal circulation. Hepatocytes reabsorb bile salts from the portal blood using the Na/taurocholate cotransporter polypeptide (NTCP) and the organic anion transporter polypeptides (OATPs). This circuit of production, secretion, absorption, and reuptake of bile acids makes up the enterohepatic circulation. Enterohepatic circulation recycles 95% of bile acids [4].
The intracellular concentration of bile acids regulates the activity of bile acid transporters. The farnesoid X receptor (FXR) detects bile acid levels and sends signals to activate genes involved in bile acid homeostasis [5]. The multidrug resistance protein 3 (MDR3) is responsible for the flux of phosphatidylcholine, another essential component of bile, which plays a protective role against BAs toxicity. The drug resistance-associated protein 2 (MRP2) exports bilirubin and conjugated drugs [4].
Genetic factors
The personal and family history are the most critical risk factors for intrahepatic cholestasis of pregnancy. About 15% of intrahepatic cholestasis of pregnancy cases would have familial aggregation suggesting genetic factors [6]. Patients with severe cholestasis have a family and personal history more frequently than other patients with cholestasis of pregnancy [2]. Mutations have been described in multiple genes encoding the proteins involved in bile formation associated with intrahepatic cholestasis of pregnancy. The most studied are mutations and variants of the ATP binding cassette subfamily B member 4 (MDR3) and ATP-binding cassette, sub-family B member 11 (BSEP) genes. In the South American population, a role for the ATP Binding Cassette Subfamily C Member 2 (MRP2) gene was reported, whereas in Europe, 10 to 15% of cases of cholestasis of pregnancy are attributable to variants in the genes encoding multidrug resistance protein 3 and ATP-dependent bile salt exporting pump [4]. The nuclear receptor subfamily 1, group H, member 4 (NR1H4) gene encodes the intracellular farnesoid X receptor, and variations in its sequence are also related to the cholestasis of pregnancy [4]. A recent case series observed mutations in bile acid transporters in severe cases, in cases of early-onset, and those with an inadequate response to ursodeoxycholic acid [7].
Hormonal influence
Besides the genetic background, the risk of intrahepatic cholestasis of pregnancy increases in a context with higher levels of estrogen and progesterone, as occurs from the second half of pregnancy and in multiple gestations. The estrogens inhibit the farnesoid X receptor (FXR), decreasing the expression of the ATP-dependent bile salt exporting pump (BSEP) in hepatocytes. Reduced ATP-dependent bile salt exporting pump expression causes abnormal bile acid transport into the canaliculus. Some progesterone metabolites can also reduce farnesoid X receptor and ATP-dependent bile salt exporting pump activity [4,8]. Until now, it appears that the onset of the cholestasis of pregnancy originates in a genetic background in the function of the bile acid enterohepatic cycle, affected or modified by the effect of the sex hormones. However, other kinds of factors must be involved.
Perinatal complications
Regarding the perinatal effects of intrahepatic cholestasis, we know that the fetal liver synthesizes bile acids from week 12 of gestation, and the placenta exports the bile acids produced by the fetus to the maternal compartment. The transporter encoded by the ATP-binding cassette superfamily G member 2 (ABCG2) gene, located in trophoblastic cells, regulates the flow of bile acids to and from the fetus [9,10]. In normal pregnancies, bile acid concentrations are higher in fetal than in maternal blood, maintaining the transport gradient. In patients with intrahepatic cholestasis of pregnancy, the transplacental bile acid gradient may be inverted, elevating bile acid concentrations in fetal plasma [8,9]. This increase in bile acids could partly explain the increased risk of meconium, premature labor, and stillbirth observed in intrahepatic cholestasis.
Due to increased bile acids in the fetal plasma, increased fetal colonic motility may explain the passage of the meconium into the amniotic cavity [11,12]. The cause of the increased risk of preterm birth in women with cholestasis of pregnancy is unknown. We postulated that increased plasma bile acids in these women activate the oxytocin receptor pathway in the myometrium, thereby prematurely increasing myometrial contractility [13]. Regarding the increased risk of stillbirth, some theories have surmised that bile acids could alter the function of cardiomyocytes, thus causing lethal arrhythmias [14]. Additionally, bile salts can generate oxidative stress and promote placental vasculature vasoconstriction, thus reducing fetal oxygenation [4].
Epidemiology
The current prevalence of intrahepatic cholestasis of pregnancy is 0.1 to 2%, although it exhibits a high degree of variation. Chile had a high frequency of approximately 15% in the 1970s and 1980s [2,15]. In a multicenter cross-sectional study in Chile in the late 1970s, the incidence was 27.6% in the Araucanian population and 15.1% in the Caucasian population [15]. Since that period, the prevalence of intrahepatic cholestasis of pregnancy in Chile has decreased markedly; in 2002, epidemiological studies reported a 1.5 to 4% prevalence [16]. A wider possible hypothesis for the decrease in the incidence is a population change in diet and hygiene habits, with a consequent change in the microbiota of pregnant women in our country.
Discussion
As was previously mentioned, there is no simple explanation as to why the incidence of intrahepatic cholestasis of pregnancy in Chile has gradually decreased since the early 1990s. We observed that other epidemiological changes occurred in parallel during this time, suggesting they may be related to the decrease in the incidence of cholestasis of pregnancy.
First, it is necessary to highlight the variations in other hepatobiliary diseases that have occurred over time in Chile, such as gallstones and gallbladder cancer . The presence of gallstones is the most significant risk factor for gallbladder cancer and is also a risk factor for cholestasis of pregnancy. Gallstones and gallbladder cancer share several common factors, including distributions by gender, ethnicity, and geographic area, with higher incidences observed in women, South American countries, and indigenous populations, such as the Mapuche [17]. Gallstones are a globally rare disease but are prevalent in Chile [18]. Similarly, biliary cancer is rare worldwide but very common in Chilean women (11.7 in 100 000 women) [19]. This association of high incidence in Chile of lithiasis and biliary cancer resulted in the hypothesis of a causal role of gallstones in cancer. The incidence of cholelithiasis and biliary cancer has decreased in Chile in recent decades. This reduction is partially explained by the increase in cholecystectomies in women with gallstones [20].
Many publications have established a link between some gastrointestinal pathogens and biliary diseases. An example is an infection with Salmonella Typhi, which is the causative agent of typhoid fever. Salmonella Typhi can generate a chronic illness in 2 to 5% of patients, even colonizing the bile duct and promoting stone formation [20]. In addition, it is essential to consider that women of reproductive age have a higher risk of being carriers of Salmonella than the male population [21]. Reports from countries with endemic typhoid fever, such as India, as well as a 2014 meta-analysis, have concluded an association between carriers of Salmonella Typhi and an increased risk of gallbladder cancer [22,23]. Today, there is a consensus that Salmonella Typhi infection has a possible causative role in bile duct stones and cancer [24].
Typhoid fever has been endemic in Chile since the 1950s, reaching its highest incidence (80 in every 100 000 individuals) in the 1980s [17]. The Chilean health institutions in the 1990s made substantial efforts to prevent the cholera epidemic that spread from Peru, with improvements in hygienic conditions and the promotion of the safe handling of food products, which are sources of the contagion of the pathogen in question. These campaigns were highly successful, as they prevented the cholera epidemic and produced a sudden decrease in the incidence of typhoid fever [17].
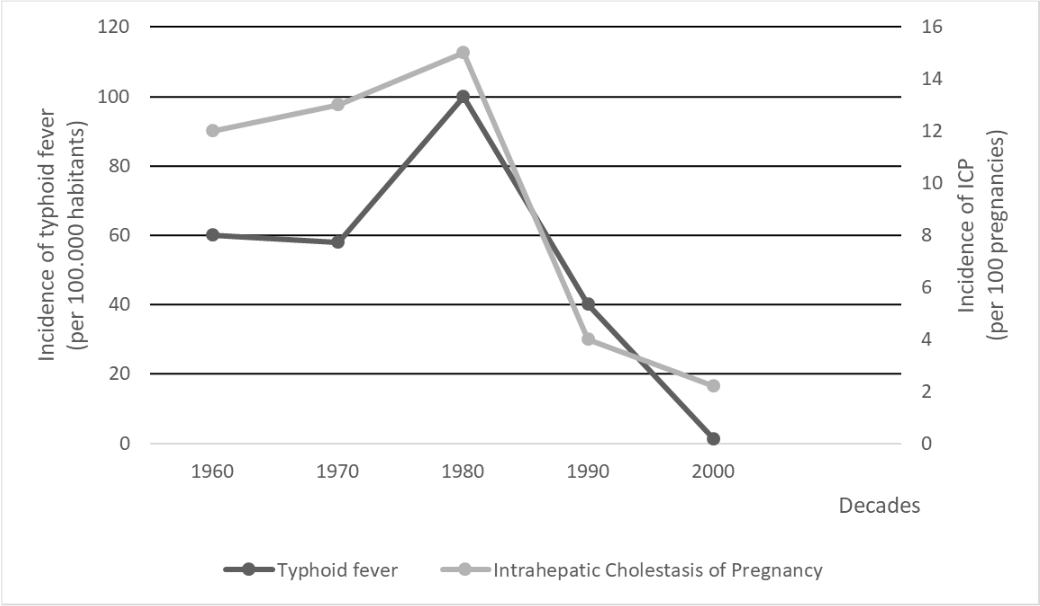
Herein, we report a significant parallel decrease in typhoid fever and intrahepatic cholestasis of pregnancy (Figure 1). The highest incidence of typhoid fever recorded in Chile in the 1980s correlates with the highest incidence of intrahepatic cholestasis of pregnancy that was recorded in the country. At later time periods, both pathologies showed a marked decrease [6,15,17,25,26]. This epidemiological association leads us to postulate Salmonella Typhi, or its chronic carriage, as a potential contributing factor in the genesis of cholestasis. There are no published studies that prove the relationship between Salmonella Typhi and pregnancy cholestasis. Nevertheless, one study showed that an intestine's permissiveness to the passage of pathogens into the porto-hepatic system could be related to this pregnancy disease [27]. Obviously, our hypothesis is ecological and based on temporal correlation; it does not establish causality.
Temporal trends in Chile showing the parallel decline of intrahepatic cholestasis during pregnancy incidence and typhoid fever rates. The peak of both conditions was observed in the 1970s to 1980s, followed by a marked reduction since the 1990s, coinciding with improvements in public health measures and sanitation.
Source: Prepared by the authors based on the cited references.
Recently, studies on the role of the microbiome in human health have increased in number. We found a few studies evaluating the associations between the gut microbiota and cholestasis in pregnancy. As we mentioned above, some bacteria are involved in the metabolism of the bile acids and lipids, mostly in the intestines. Some studies have found changes in the gut microbiota when they compared patients with intrahepatic cholestasis with controls. The authors describe a decrease in short-chain fatty acid-producing bacteria, plus an increase in the species involved in bile acid metabolism [28,29,30]. One of the studies describes that the differences in the microbiome could be detected even before the onset of the symptoms [30]. While the other proposes that microbiota changes may be the consequence of abnormal excretion of bile acids into the gut [28]. A 2021 study conducted in China, also correlated some genera of bacteria with clinical characteristics of intrahepatic cholestasis of pregnancy and found differences in microbial gene expression between mild and severe disease. Some of the genera increased in intrahepatic cholestasis of pregnancy are Parabacteroides, Bilophila, Citrobacter, Streptococcus, and Blautia. On the other hand, a decrease in the abundance has been observed in the Bifidobacteria genus [28,29,30,31]. A 2020 article demonstrated changes in microbiota in response to ursodeoxycholic acid in patients with cholestasis [32].
Limitations
This analysis has several limitations inherent to its selective non-systematic approach. First, the selection of studies was not based on a systematic methodology, which introduces the possibility of selection bias and incomplete retrieval of relevant evidence. The heterogeneity of the included studies, along with the absence of a formal critical appraisal of their methodological quality, limits the strength of the inferences that can be drawn. Additionally, the proposed hypothesis relies predominantly on temporal and epidemiological correlations, which do not establish causality and must be interpreted with caution. Other contextual factors that may have contributed to the historical decline in intrahepatic cholestasis of pregnancy in Chile—such as changes in diet, improvements in socioeconomic and sanitation conditions, and broader shifts in public health—were not evaluated in depth and warrant further exploration. Ultimately, the associations presented here should be considered exploratory, and experimental or mechanistic studies are needed to validate the proposed microbiological hypothesis.
Conclusions
Intrahepatic cholestasis of pregnancy is a clinically relevant liver disorder in pregnancy. Historically, Chile reported unusually high incidence rates, reaching up to 15% in the 1980s, which have progressively declined to approximately 1 to 2% in recent decades [33]. This temporal decline parallels the reductions in bile duct diseases (lithiasis and cancer) and in gastrointestinal infections caused by Salmonella Typhi. From an ecological and historical perspective, this observation supports the hypothesis of a possible association between chronic or population-level exposure to Salmonella Typhi and the epidemiological pattern of intrahepatic cholestasis of pregnancy in Chile, without implying causality. Another possibility is a decrease or change in other bacterial species that make up most of the microbiota in our population. Future research integrating genetic susceptibility, microbiome, and novel biomarkers may help clarify the mechanisms underlying intrahepatic cholestasis of pregnancy. Based on this microbiological framework, the present analysis could motivate studies exploring changes in microbiota and infectious exposures among Chilean women with current or previous cholestasis of pregnancy. Any potential therapeutic implications remain speculative and would require dedicated clinical and experimental research.
